Introduction
Medical
schools are constantly working to improve the quality and process of the
educational experience for students, often incurring considerable investment by
faculty, students and other stakeholders. Specifically, models of clinical
rotations for third-year medical students have been explored in great depth.
Existing research has compared outcomes of students involved in these different
models, including longitudinal integrated, hybrid, and block clerkships.
Key
differences in student experiences and outcomes between discipline-specific block
rotations and the continuity of longitudinal, integrated, and hybrid clerkships
support the benefits of continuity in clinical learning. Specifically,
Teherani, et al. identified that students enrolled in longitudinal integrated
clerkships rated patient centered experiences; faculty teaching, feedback, and
observation; as well as the clerkship itself higher relative to students that
participated in hybrid or block clerkships. Yet, student performance on the
United States Medical Licensing Exam Step 2 (clinical knowledge) was equivalent
across models [1].
Results
support that integrated and continuous models are sustainable and generally
lead to improved or, at minimum, equivalent performances by students compared
to traditional rotations and may influence student choice of psychiatry as a career
[2]. Multiple lines of research support that longitudinal integrated clerkships
offer students important intellectual, professional, and personal benefits,
including better clinical preparedness, richer perspectives on the course of
illness, more insight into social determinants of illness and recovery,
and increased commitment to patients [3]. Additionally, longitudinal integrated
clerkships can be implemented successfully at a tertiary care academic medical
center [4]. These and other studies, including previous work from psychiatry and other
specialties, support that curriculum innovation may be valuable to students
overall educational outcomes.
While
the body of evidence supporting the benefits of longitudinal integrated
clerkships is apparent, there remains a gap in the understanding of the
academic outcomes of students that participated in newer clerkship models.
Longitudinal clinical placements are underpinned by two central theoretical
concepts: continuity, and symbiotic clinical education [5]. In the review by Walters,
et al, the authors concluded that further exploration into the etiologies of
the transformational nature and effectiveness of newer curricular models is
necessary [6].
Existing
literature provides key insights about the optimal measures of assessing
curricular outcomes. Multiple miniinterviews for prospective medical students,
combined with preadmission cognitive indicators, have been shown to be
predictive of clerkship and licensing exam performance [7,8]. The process by which
medical schools identify, nurture, and transform prospective academically-viable
and interpersonally-capable students into skilled, patient-centered, and
resilient physicians remains rather elusive. It is amid this backdrop, that
there appears to be nationwide fervor to develop programs that can provide this
foundation.
Likewise,
The Ohio State University (OSU) College of Medicine is in the midst of
curricular revision, namely with implementation of the Lead
Serve Inspire (LSI) program. This program
has fundamental differences compared to the existing curriculum, including
greater emphasis on clinical integration of specialties and longitudinal care,
as well as earlier exposure to patients. In addition, the revised curriculum
prominently features modifications to traditional learning strategies, such as
newer methods of content delivery, multidisciplinary presentations, and highlighting
critical appraisal skills. The LSI curriculum, itself, is unique amid an era of curricular
innovation, comprised of both longitudinal integrated and hybrid components. As
medical schools across the country are placing greater emphasis on newer modes
of learning, this study is undertaken to glean further data about the
implications for LSI in
psychiatric education.
Specifically, the purpose of this retrospective study is to compare the
clinical and examination performance of OSU medical students who participated
in a longitudinal pilot curriculum to those who participated in the existing,
traditional curriculum during their third-year of medical school.
Methods
The
Institutional Review Board at The Ohio State University Wexner Medical Center
approved this study. The LSI curriculum for third-year medical students was retooled and
positioned to occur as part of a combined experience involving the disciplines
of psychiatry, neurology, and
internal medicine. Instead of having students rotate through these specialties
via four-week consecutive blocks, students rotated in each discipline for
two-week intervals in a non-sequential manner and revisited each discipline at
defined intervals over the course of a four month period as noted in Table 1.
The
clerkship settings between students completing the LSI curriculum and the traditional pathway
did not differ in terms of student distribution and time commitment. In both
groups, approximately 70% of students were assigned to an inpatient service,
while 30% were assigned to a consultation liaison service. As ascertained by
duty hour reports completed by students, there were not appreciable differences
by either group in terms of time devoted to daily clinical responsibilities and
subsequently time available for studying.
Students
in neither group reported duty hour concerns during their clinical assignment.
Students in both the LSI and
traditional experiences each completed two on-call experiences in psychiatry and neurology, which
consist of participation in patient care activities until 10:00 pm on the call
nights. There is no on-call experience during the internal medicine rotation
for students in either the LSI curriculum or the traditional pathway.
In
addition, considerable attention was focused on having student seminars be
active, as opposed to passive learning, and enhanced to present patient care
information in a clinically relevant, instead of discipline-specific, manner.
Unlike prior curricula, content was delivered by multiple faculties with
differing specialties. For instance, an internist, neurologist, and psychiatrist all
participate in the discussions of the approach to delirium. Emphasis was also
placed on enhancing clinical and procedural skills and modeling of positive
faculty physician behavior. The Ground School consisted of week-long intensive
course in procedural and clinical essentials of the three disciplines.
This
review included data of third-year medical student clinical performance
evaluations in psychiatry and examination performance from approximately 75
medical students who participated in the clerkships described from October 2013-February
2014. In order to be a candidate for the pilot program, students had to be in
good academic standing, as defined by the College of Medicine. There were a
total of 15 students who volunteered to participate in the pilot program
described above. Sixty students enrolled in the traditional sequential block
rotations of psychiatry, neurology, and internal medicine during this same time
period served as the comparison group.
The
study endpoints included comparison of National Board of Medical Examiners
(NBME) examination scores and comparison of clinical performance evaluations
for students in both the pilot and traditional psychiatry,
neurology, and internal medicine clerkship groups. The researchers utilized
t-test statistical analyses to determine if there were trends or statistically
significant findings between the comparison groups. Demographic data on the
study participants was not available. Students also completed multiple surveys
to assess their satisfaction with faculty and the clinical experience and its
various components; however, this data was not the focus of this research
project.
Results
There
were no significant differences between the pilot vs. control students in terms
of their academic performance measures in medical school prior to the study.
The average clinical performance evaluations scores
of students participating in the LSI Pilot were 84.7, whereas
those enrolled in the traditional pathway scored 80.3 (p=.072). Data from clinical performance evaluations of students
during neurology
and internal medicine clerkships was not available for the purposes of this
study.

Table 1: Integrated, hybrid pilot schedule of Internal Medicine (IM), Neurology and Psychiatry Rotations.
Figure 1 demonstrates that the NBME subject examination class averages
of students enrolled in the combined internal medicine, neurology, and psychiatry pilot
program were all relatively higher compared to students completing these
examinations and enrolled in the traditional block rotations during the same
time period.
The data for both the clinical and examination performance did not
reach statistical significance (internal medicine p=.085, neurology p=.068, psychiatry p=.061). Measures of clinical performance, namely evaluations from
faculty, were noted to be slightly higher for pilot students compared to
students not enrolled in the pilot. In psychiatry ratings
specifically, students performed above average on clinical measures of medical
knowledge, communication skills, and diagnostic assessment and critical analysis
skills.
Discussion
Medical schools across the nation continuously look to improve the
educational outcomes and quality of the student experience; yet, there remains
a gap in understanding the meaning and significance of outcome measures in
novel curricula. In this experience, the LSI curriculum was specifically
targeted to enhance the critical thinking skills of students, drive faculty
-student interaction, and maximize the collaborative learning context of patient
care. The lack of statistically significant differences between study and
control groups suggests that the benefits, if any, of an integrated clerkship
may be negligible. However, the preliminary results of the pilot program offer
reason for educational leaders to be optimistic.
In this study, the academic profile of the pilot students was not different
than the comparison students; yet, the pilot group posted examination scores
that were on average, higher. Similarly, the pilot program was considered a
success from the results of the students clinical performance in psychiatry, in spite
of the study limitation of small sample size of the groups. Like similar studies
exploring new curricular modalities, the rationale for this difference is not clear
and this pilot study has several limitations.
Specifically, these results are difficult to interpret given the
study limitations of a small pilot group sample size, unequal numbers of students
in the pilot and comparison groups, selection bias of the curricular
assignments, and the inability to define the component of the LSI program that most readily influenced performance measures.
The pilot program was noted to have considerable obstacles to
implementation, some predictable and others unforeseen. Perhaps the greatest
challenge was faculty buy-in to a program which structurally provided less
continuity of care than traditional longitudinal clerkships that generally occur
on an outpatient basis. The sequence of two-week rotation blocks not only posed
a tactical challenge for coordinators and clerkship directors alike, but both faculty
and students commented on the frequent interruptions to begin a new service
when they were just feeling comfortable with their current teams and patient
care responsibilities.
Psychiatry
faculty, especially, were initially struggling with the concept that they would
have shorter durations of exposure to students, albeit equating to a proportionally
similar overall duration of psychiatry experience throughout the longer pilot program.
Some faculty expressed concern that shorter psychiatry rotations would allow
for less time for students to use feedback to identify and modify deficiencies
in clinical performance. However, faculty demonstrated improved buy-in as
students returned to services with reinvestment in learning psychiatry
following a hiatus for several weeks. One other limitation that could have
impacted the performance of pilot students was that they received first choice of
faculty preceptors, thus some selection bias may have favored the student-supervisor
pairings.
Due to the small size of the LSI cohort, this study did not formally
examine the relationships, if any, between curriculum completed and interest in
future careers in psychiatry. Anecdotally, one student in the LSI group stated an interest in pursuing a psychiatry residency. The
authors are considering future studies to retrospectively determine if switching
to the integrated curriculum had a positive, negative, or neutral effect on
recruitment into the specialty. Further, additional studies of larger cohorts would
be directed at measuring intangible benefits recognized by longitudinal
integrated clerkships, such as practice habits in residency suggestive of
better clinical preparedness and pre- and post-assessments of social
determinants of illness and recovery between control and study groups.
While the results of the pilot program represent a relatively small
sample of the medical student population, further information is anticipated to
be forthcoming to determine if the results are able to be generalized to the
entire third-year class. All students have subsequently been enrolled in the LSI Curriculum for the 2014-2015 academic schedule and will be
participating in this experience in years to come.
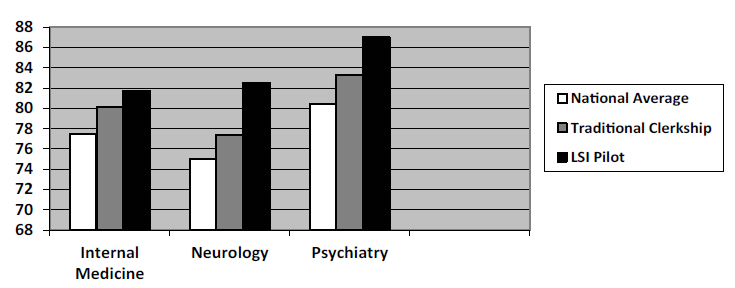
Figure 1: NBME Score Performance of Traditional Clerkship vs. LSI Pilot Students
Implications for Educators
The
results of this preliminary study support earlier lines of research
demonstrating promise in academic and clinical outcome measures with novel
curricula. Undertaking a massive curriculum revision has necessitated the investment
of considerable resources and collaboration across departments, with buy-in at
both the faculty and student level critical for the program to be successful.
References
1. Teherani A, Irby DM, Loeser H. Outcomes of different clerkship
models: longitudinal integrated, hybrid, and block (2013) Acad Med 88: 35-43.
2. Griswold T, Bullock C, Gaufberg E, Albanese M, Bonilla P, et
al. Psychiatry in the Harvard Medical School-Cambridge Integrated Clerkship: an
innovative, year-long program (2012) Acad Psychiatry 36: 380-387.
3. Hirsh D, Gaufberg E, Ogur B, Cohen P, Krupat E, et al.
Educational outcomes of the Harvard Medical School-Cambridge integrated
clerkship: a way forward for medical education (2012) Acad Med 87: 643-650.
4. Poncelet A, Bokser S, Calton B, Hauer KE, Kirsch H, et al.
Development of a longitudinal integrated clerkship at an academic medical
center (2011) Med Educ Online 16.
5. Greenhill J, Poncelet AN. Transformative learning through
longitudinal integrated clerkships (2013) Med Educ 47: 336-339.
6. Walters L, Greenhill J, Richards J, Ward H, Campbell N, et al.
Outcomes of longitudinal integrated clinical placements for students,
clinicians and society (2012) Med Educ 46: 1028-1041.
7. Reiter HI, Eva KW, Rosenfeld J, Norman GR. Multiple mini-interviews
predict clerkship and licensing examination performance (2007) Med Educ 41:
378-384.
8. Eva KW1, Reiter HI, Rosenfeld J, Trinh K, Wood TJ,
et al. Association between a medical school admission process using the
multiple miniinterview and national licensing examination scores (2012) JAMA
308: 2233-2240.
Corresponding author:
Julie Niedermier, The Ohio State
University College of Medicine, 1670 Upham Hall, Columbus, OH 43210,
USA, E-mail: Julie.niedermier@osumc.edu
Citation:
Niedermier
J, Teater J, Kasick D and Jahdi M. A Comparison of Third-year Medical
Student Clinical and Examination Performances in a Traditional
Psychiatry Clerkship to a Novel Pilot, LSI Curriculum (2015) EPOA 102:
7-10



