
 PDF
PDF
Introduction
If something characterizes the Borderline Personality Disorder is its diagnostic complexity, its comorbidity with other types of conditions and its high ignorance on the part of many health professionals, in general, and mental health, in particular. In this review of the subject we will try to put some light on this type of psychopathology; a necessary light, not so much for the professional as for the hidden victim of this ailment, the great protagonist, not for his stigma of illness, but for his degree of vulnerability and widespread instability.
For example, when a child, adolescent or adult is seen apathetic, lacking in energy and lacking perspective in current and future life, we might think that we are facing signs of a mood disorder. But what happens to those types of people to whom some professionals, out of ignorance, predict anything and others simply diagnose them of BPD?
A Look Back
To understand the BPD, on many occasions, we will have to go back to childhood and early adolescence of this type of people, since approximately 50% of those affected already had behavioral disorders in these early stages of their life, being more frequent in men than in women. An early psychomotor development, the appearance of disorders such as Attention Deficit Hyperactivity Disorder in the child or adolescent, and/or the head or end of a sibling list, may constitute some of the necessary ingredients for an early onset of the disorder; If we add a poor diagnosis to these cases, we will obtain the necessary breeding ground for a chronic development of this psychopathology.
Drawing a Characteristic Profile of the BPD
Some authors, considering that between 10 and 33% of these people consume suicide, come to talk about BPD as an equivalent of suicidal personality or as a disorder characterized by chronic self-injurious behavior. Is this the reason why this type of patient is supposed to request greater assistance and hospitalization? Probably, the answer is affirmative, although this does not imply the greatest guarantees of life and therapeutic success. But, if we were to draw the robot portrait of the patient with critical BPD, what profile would we get?
It seems that being male, between 30 and 35 years old, with a history of childhood trauma, variable self-perception, or what is the same, with an alteration of identity; Chronic self-destructive behaviors, with manifest efforts to avoid abandonment, for which, on many occasions, third-party manipulation is used; apparatusity (theatricality), emotional blackmail, feeling special and center of attraction, along with the desire for prominence, for which you will use seductive behaviors ... are some of the genuine behaviors in these types of people. This typology could make us think that we are facing despicable beings. But, if we add to these aspects such as the feeling of loneliness and insecurity, the misunderstanding and hopelessness, the frustration, the confusion and the abandonment that they probably manifest, we realize that what we really have in front of us is, more well, an extremely vulnerable and sensitive being (see figure 1).
These last two aspects will condition in a peculiar way our future therapeutic intervention. But we will see that later.
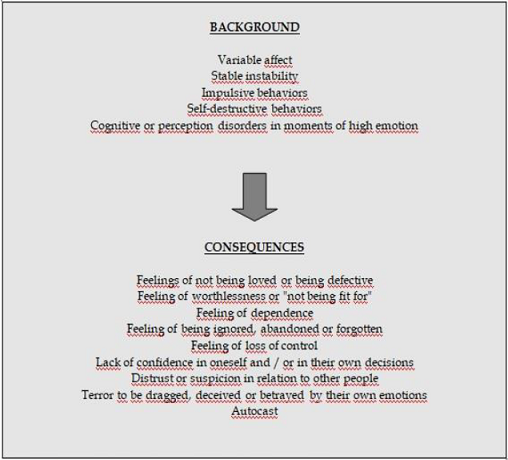
Figure: Cognitive-Behavioral Background and Consequences in the BPD.
Comorbidity of the BPD
We might think that, with what has been described so far, we already know everything about the TLP (Time-Limited Psychotherapy), but, dear reader, nothing is further from reality, since this is only an orientation that can help us, of course, a great help. We are facing one of the most complex disorders to diagnose and address in clinical mental health centers.
This type of disorder, quite frequently, occurs along with other mental disorders, such as: mood disorders, addictive behaviors, behavioral disorders and post-traumatic stress disorder. Some authors add to the previous ones: distress disorders, psychotic disorders, obsessive compulsive disorder and bipolar disorder. If this is so, and everything indicates that it is, it seems that the diagnosis, which a priori might seem like a simple task, is complicated, right? Keep calm and continue, because we are going to try to put some order to all this apparent chaos.
Types or Variations in the BPD
The BPD can have four possible variations:
· Psychotic or Unrealized BPD
· Uncontrolled Impulse BPD
· Thymic or Affective BPD
· Dystocia of the I BPD
Each of the previous variations presents its particular characteristics. As the objective of this review is not the depth but the generalization of the disorder, I will skip talking about the peculiarities of each of them.
Lets stop this short tour to silver some reflections...
Could self-injury be considered as a way for the patient to feel alive? And as a way to distract your emotional pain from the lack of personal resources to face it? During this type of episode, could there be a splitting of the person (of the I) who obeys a superior force, being self-injury a form of submission or punishment? Lets keep going…
Medicine and Pharmacology
Before we can see what we can do before such people on the psychotherapeutic level, we must warn that, although medicine and pharmacology have gained prominence in recent times within the field of mental health, it is important to note that there are no specific authorized drugs available. For the Treatment of Personality, therefore, they should only be used to alleviate the symptoms of emotional and affective instability, impulsive-behavioral control and cognitive-perceptual difficulties.
Moreover, without the intention of hurting susceptibilities, I am of the opinion that the apparent improvement of the patient after the administration of the new psychoactive drugs (last generation drugs) may be due to the fact that they act on other types of comorbid disorders with the BPD, more than the BPD itself.
Approach of the Person with Borderline Personality Disorder
When considering approaching a patient with BPD, we propose twelve basic and fundamental principles that should be taken into account, if what we seek is, among other things, to manage the extreme vulnerability and sensitivity that this type of people present.
So, these are the twelve commandments that we propose to the therapeutic community:
· Be constant
· Be patient
· Dont lose therapeutic north
· Maintain the improvement
· Be cautious
· Don´t transmit doubt
· Don´t judge
· Normalize, but not invalidate
· Keep calm
· Avoid climbing
· Flee from emotional contagion
· Believe in the possibilities of patient improvement
We must work with the treatments that work, trying to adapt and improve them in each case if it is convenient and/or necessary, without forgetting that the one who knows most about this type of ailment is the patient himself. So, let us be aware that the information that the client can provide us can be crucial for therapeutic progress.
Our first objective should be: patient safety and the avoidance of behaviors that may interfere with the therapeutic process, such as self-destructive behaviors, self-harm and suicidal ideation.
The second objective will be the need to establish a solid therapeutic alliance and a positive emotional connection, a climate of security and trust that encourages the exchange of opinions, and ensure that the patient feels as part of a work team, not as someone to which others must heal or change.
Other types of objectives can be raised in patients more functional and motivated by the therapeutic process, such as:
· Stimulate reflection, rather than impulsive action
· Achieve greater knowledge of himself and his problems
· Achieve the hope of leading a normal life in the near future
· Achieve the abandonment of self-destructiveness and self-sabotage
· Take advantage of the skills that most patients have.
· Get the functionality of the patient
An example of the Individual Therapeutic Program
We propose a Therapeutic Program of Progressive Approach (TPPA), which the therapist will try to make more flexible and adapt according to the capacity and degree of involvement of the patient with respect to the proposed therapy.
This program (TPPA) consists of six parts:
Self-observation: Is that the patient reflects
and becomes aware of their behaviors, thoughts and feelings. The use of
evaluation self-records is suggested.
Self-care: Indicated, mainly, to
address destructive and autolytic
behaviors. It is advisable to maintain reasonable limits, firmly set, but
leaving option to flexibility, depending on the circumstances of the patient.
Psychoeducation about BPD: Acts as a complement to
therapy, seeking to provide defense mechanisms for the patient, control their
impulsiveness and the reasons for their destructive behavior, minimize their
emotional vulnerability, lack of limits, alteration of identity and reduce
relational problems, among other aspects.
Intermediate Evaluations: They are proposed as a
measure of controlling therapeutic progress. It is suggested to use the written
self-assessment,
having obtained satisfactory results with this type of practice.
Emotion Management: Mainly, with the
purpose of adapting to thoughts, interpretations, judgments and beliefs. It is
convenient for the patient to distinguish between primary and secondary
emotions.
Coping Techniques: Of all these tools, it seems
that written expression and psychoeducation will
occupy a favorite place in the therapeutic choice, being the most indicated in
this type of patients.
Therapeutic Collective Program
Group Therapy may be appropriate, since, through it, you can help improve the communication and expression of feelings of the patient, and develop their sense of empathy. Through this technique, the patient can share a group of equals with their situation and experiences. But, could it not be counterproductive, if we think that the group can act as a mirror for the patient? Could this make the diagnosis worse in some less tolerant, more sensitive or more vulnerable patients? These are questions that oblige us to keep in mind the aforementioned commandments and, above all, to make each case more flexible and work in a personalized way.
Family Intervention
Although Family Intervention is not always necessary, it can be beneficial in patients who live with their relatives or who depend economically on them. Our goal will be to avoid any type of interference in therapy. However, we must bear in mind that, before starting this step, the patient must first be known, guaranteeing absolute confidentiality and credibility with respect to third parties.
Psychoeducation about the disorder to relatives is important, since it is the only way for them to understand what happens to the affected and a way to avoid interference in therapy; for example, in case of critical comments or allusions to negative behaviors, or in case of generalizations that may produce hostility in the interrelation. Emotional over-involvement and family intrusiveness can also be harmful, in the same way as attributing the role of the patient or wanting to be a shaman apprentice trying to read the patients thoughts. For these and other reasons, the patient-family relationship can range from anger to silence, having already predictable consequences.
Episodes of Crisis
Finally, say that a patient with BPD may have episodes of seizures that we must have previously considered before the end of therapy. Although crises do not respond to schedules, it is important to help the patient know how to distinguish between a real crisis and a bad time. Telephone support has proven to have good results in these types of situations. The purpose is for the patient to be able to manage himself, without having to resort to the therapist constantly. In any case, it is advisable to carry out a gradual therapeutic abandonment to, thus, counteract the fear and insecurity that may arise in the patient to know and feel that the time has come to ride the bicycle oneself, without the help of auxiliary wheels (the therapist).
Professional self-care
Last but not least, add that it will be necessary for the therapist to develop self-care, since working with mental health patients can erode our own abilities and interfere with our work to help others.
References
1. Mosquera, Dolores. Rough diamonds Vol. I and II (2004) Madrid. Ed. Pleiades, Spain.
2. Mosquera Dolores. Evaluation and Treatment of Borderline Personality Disorder. Virtual course (2005) Sixth Virtual Congress of Psychiatry, Interpsiquis.
*Corresponding author:
Jaime Senabre, Director of SINIF, University of Alicante, Spain, E-mail: jasenabre@sinif.es
Citation:
Senabre J. The stable instability of people with borderline personality disorder (2019) Edelweiss Psyi Open Access 3: 29-31.
Keywords
Borderline personality disorder, Mental health, Therapeutic approach, Comorbidity, Suicide.
