
 PDF
PDF
Abstract
Introduction: Ghana developed her adolescent reproductive health policy in october 2000 to guide implementation of adolescent reproductive health and related services. Despite a comprehensive policy implementation strategy, the burden of adolescent pregnancies in rural Ghana remains a public health challenge since little is known about the core predictors. This study therefore explores socio-demographic and economic predictors of the pregnancies in Amenfi West district.
Methods: The study design was a community based case-control study involving 80 cases and 220 controls. Data was collected using structured questionnaires and analyzed by Stata version 11 to examine associations between predictors of pregnancy and background characteristics of adolescents.
Results: Findings show that, being in school, coming from a wealthy household, contraceptive use, parental monitoring and relationship counselling offered significant protection against adolescent pregnancy (p<0.05). However, factors such as violent parental attitudes towards boy/girlfriend relationships, demanding financial support from adolescents for housekeeping and peer pressure from ever been pregnant friends predisposes adolescents to pregnancy.
Conclusion: Advocacy for increased social/parental support for adolescents, education on modern contraception and availability of services are keys to preventing adolescent-pregnancies in rural communities.
Introduction
The adolescent period occurs between the ages of 10-19years [1]. It is a period characterized by various psychological, social and biological transformation which exposes adolescents to the innate desire to experiment, natural tendency including violating parental advices and the pseudo-feeling of maturity thereby risking unplanned pregnancy [2,3]. Globally, about sixteen million adolescents deliver each year with over 10,000 adolescent girls in the United States of America having their first unprotected sexual exposure at age fifteen [4]. These statistics are worse in low- and middle-income countries as 95% of the teenage births occur in these countries [5]. In sub-Saharan Africa, adolescent birth rate is about 140 per 1000 adolescent with various country variations [6]. Despite the formulation of a national adolescent reproductive health policy in 2000 to address adolescent sexual reproductive health and related issues in Ghana, not much has been achieved in addressing adolescent pregnancies particularly in rural Ghana. In 2008, the adolescent birth rate stood at 13% and averagely one in ten adolescents began childbearing in the urban areas, whereas a double of this exists in rural communities [7].
Teenagers residing in rural areas (17%), those living in the Brong Ahafo, Central, and Volta regions (21-22%), those with no education (23%), and those in the second wealth quintile (21%) tend to start childbearing earlier than other teenagers [8]. In the Western region, the trend is a reflection of the national burden with Amenfi West being a high contributing district [9]. Western region recorded 10.1% of adolescent pregnancy for those between the ages of 15-19 and as much as 12.7% of that same age group had started childbearing [10]. The drivers of this phenomenon in rural Ghana have not been fully explored. This study therefore aims to explore the socio-demographic and economic predictors of the pregnancies in Amenfi West district to contribute to empirical knowledge for programming.
Method
Amenfi West (formerly Wassa Amenfi West) District forms part of twenty two Districts in the Western Region of Ghana with Asankrangwa being its administrative capital. It is located between Latitude 400N and 500 40N and Longitudes 10 45W and 20 10W. The District shares boundaries with Aowin district to the west, to the east with Amenfi east district, to the north with Bibiani-Anhwiaso-Bekwai district and to the South with Amenfi Central District. The current population of the Amenfi West District is projected at 186,257 at a growth rate of 3.2% per annum which is the regions growth rate. The district has many rural communities with a total population density of 53.76 people per sq.km. The district has four sub-districts with twenty widely scattered health facilities (i.e two hospitals, two health centers, three clinics and thirteen CHPS compounds). The study design was an unmatched case control with cases as adolescent girls who are currently pregnant or had been pregnant for the past two years before the interview, whilst the controls include adolescent girls who have never been pregnant. Data were collected using tructured questionnaires in ten rural communities within each of the three different sub-districts in Amenfi west district of Ghana. Three trained multi-lingual (English, Twi, Hausa, and Ga) field assistants administered the questionnaires to eligible participants or their guardians (in the case of minors) who consented to be part of the study.
Respondents who did not understand English were interviewed in their local languages of proficiency. Simple random sampling was applied to select three sub-districts out of the four sub-districts in the Amenfi west district. Each sub-district had ten communities randomly selected for the study with this method, the names of all communities in the each of the sub-districts was written on pieces of paper and folded. The folded papers was kept in a box and well shaken to adequately mix them up, i.e. communities from one sub-district at a time. A volunteer was called to pick one folded paper at a time (thirty times in all) and the names of those communities picked constituted the chosen communities for the study. The selection was done without replacement.
An unmatched case-control study design was used in the ratio of 1 case: 3 controls. Cases were any adolescent girl between the ages of 10 to 19 as per WHO definition living in the selected communities who is pregnant at the time of the interview or had been pregnant for the first time during the two years preceding the study. These criteria were used to minimize recall bias. Controls were chosen from the same neighborhood/community and consisted of any adolescent girl who had never been pregnant. The cases were identified through the help of community based volunteers who have personal knowledge of the pregnancy history of adolescents in their communities. In the case of the neighborhood controls, they were sampled in alternate houses and where there was more than one eligible control in a house, only one was chosen based on simple random sampling.
A contraceptive prevalence rate among 15-19year old of 19% was used as the percentage of the controls with the exposure [11]. The EpiInfo version 7 statistical tool calculated total of 275 as the sample size (69 cases and 206 controls).Making an allowance of 10% for non- response approximated the sample size to 320 i.e.80 cases and 240 controls. The sample size calculated was subsequently distributed according to the following percentages based on the population sizes of the three sub-districts selected: 40% to Asankragua sub-district (32 cases, 96 controls), 35% to Samreboi sub-district (28 cases, 84 controls) and 25% to Asankra Bremang sub-district (20 cases, 60 controls). Twenty of the questionnaires were pre-tested among residents of a nearby community in the adjoining district (Amenfi Central) to help correct potential difficulties with the usage of the tool. The data were stored electronically on two different laptops and analyzed using Stata version 11 (Stata IC version 11, College Station, Texas, USA).
As part of the ethical considerations, ethical clearance was sought from the Kwame Nkrumah University of Science and Technology Ethics Review Board and subsequently permission was obtained from the Amenfi west district assembly and health directorate. Written and verbal informed consent was obtained from the parents/guardians of the pregnant teenagers/mothers and verbal consent from the teenage mothers below 16 years of age respectively. All participants agree to publishing the research findings but anonymously.
Results
A total number of 320 respondents were sampled in the ratio of 80 cases to 240 controls. After cleaning, 300 responses (80 cases, 220 controls) were analyzed and presented with a response rate of 88.2%.There were few non-responses under some of the variables which did not reduce the power to detect the differences if existed. Prevalence of adolescent pregnancy shows that for the year 2014, seven hundred and thirty one (731) pregnant adolescents were registered (32 early teens and 699 late teens) at antennal care services across the district. Four thousand and ten (4010) ANC registrants were recorded over the same period. The prevalence of adolescent pregnancy in Amenfi West for 2014 based on health facility records was 18%.
Table 1 presents the socio-demographic and economic characteristics of respondents. More than half (60.7%) of the respondents were in the age group 16-19years while a little over two-thirds of them(71%) had Junior High School education or higher. Majority (64.9%) of the adolescents interviewed were currently schooling while the rest were engaged in one occupation or the other. Most of the study participants were Christians (68.3%) and involved in various marital relationships (83.9%). For the respondents who were in sexual unions (married/cohabiting), majority (64.3%) were in the age group 15-19 years, a quarter (25.5%) of the girls interviewed had their male guardians/parents who had not pursued any formal education while a little over a third (36.9%) of their female guardians/parents were not formally schooled.
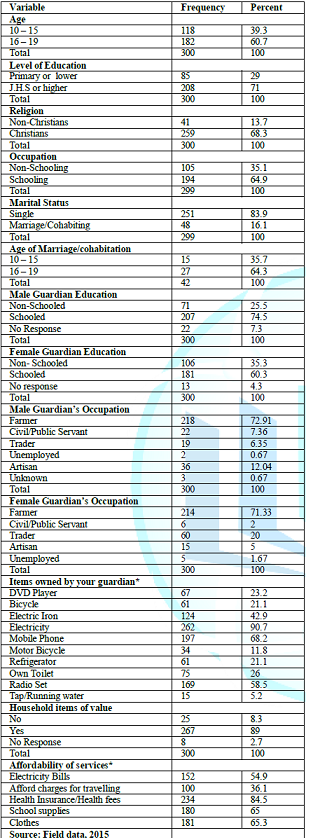
Table 1: Socio-demographic and economic characteristics of respondents.
With regards to socioeconomic characteristics of respondents using they or their guardians possession of certain household items, about 23.2% of them had Digital Versatile Disc (DVD) players, 21.1% had bicycle, 68.2% had mobile phones, 11.8% had motor bicycles whiles only 5.2% had tap/well water within the household compound. Majority of them (89.0%) conceded the items asked about were of value to them. On the ability of respondents to afford certain essential items, 27.6% of them had registered with the NHIA and could afford paying for healthcare. Almost equal numbers (21%) had regular school supplies and were satisfied with the amount of clothing they had. The school supplies were mainly stationery and fees. Majority of respondents had their male and female guardians being farmers i.e. 72.91% and 71.33% respectively. Very few of the guardians were engaged with the civil/public services i.e.7.36% for the male and 2.00% for the female guardians. Among the male guardians, 0.67% was unemployed while the females had a 1.67% unemployment rate.
Relationship between socio-demographics and adolescent pregnancy
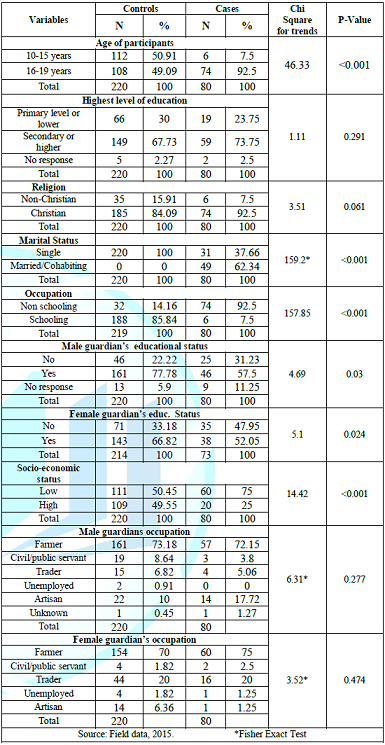
There were no significant statistical differences between the cases (adolescents that are currently pregnant or had been pregnant two years preceding this study) and controls (adolescents that had never been pregnant) with respect to their level of education (p=0.291), religion (p=0.061), and marital status (p=0.321). The cases and controls however differed significantly with respect to the age of study participants (p<0.001), occupation of respondents (<0.001), male guardian level of education (p=0.030) and female guardian level of education (p=0.024). With regards to relationship between socioeconomic status and adolescent pregnancy, there were no significant statistical differences between the cases and controls with respect to their male and female guardians occupations (p-value=0.277 and 0.474 respectively). There were however statistically significant differences between the study groups with respect to their socio-economic status (p<0.001). Those who possessed at least a minimum of five household items and could afford at least two essential services rendered were categorized to be in the high socio-economic ladder. The items asked about were electricity, motor bicycle, television, bicycle, electric iron, mobile phone, refrigerator, DVD Player and tap/well within compound. The affordability of the following services was questioned: travelling fares, electricity and hospital bills, regular supplies of school items and satisfied amount of clothes (Table 2).
Examining the adolescent-parent relationship and peer influence on the prevalence of adolescents pregnancy, it was observed that majority (56.7%) of adolescent girls were staying with both parents while approximately half of them had ever had sex education discussions with parents. Most (84.7%) of the study participants had never discussed contraceptives with guardians although 15%of their guardians patronized alcohol/abused drugs. Most (58%) of the adolescent could not discuss their relationships with their parents. Half (53.3%) of them had parents with violent attitudes towards boyfriend/girlfriend relationships.
Just a few of respondents (4%) however felt pressured by guardians to contribute towards house upkeep financially or materially. About a third (27.4%) of the respondents in the study had more than three friends with just 1%having none. About three-fifths (58.7%) of the study population never had a pregnant peer and 87.7%of their peers would be sad if they (the respondents) were to be pregnant. A third (31.4%) conceded that their friends opinion moderately influences their sexual lives. Ten percent (10%) of respondents had ever discussed contraceptives with their friends and that about five percent (5.1%) of them would advise their friends to go for an abortion in the event of getting pregnant.
A regression analysis of responsible parenthood on the prevalence of adolescent pregnancy in the study area shows significant differences between those who were staying with both parents and those who are not with respect to getting pregnant. In Model 1, those staying with both parents were approximately fifty percent less likely to get pregnant when compared with those not staying with both parent (OR=0.53, 95% CI: 0.31-0.88, p value <0.05). In Model 2, this effect was lost completely. Similarly, both parents discussion on sex and contraception offered protection against adolescent pregnancy. Discussion on sex minimized the risk of a respondent significantly. (OR=0.44, 95% CI: 0.26-0.27, p value <0.05).
Adjusting for other covariates, this protection offered by discussion of sex and contraceptives was lost. Monitoring of adolescent childrens where-about in the study area was observed as a significant parental concern as this offered protection to the adolescent whose guardians were concerned by reducing their likelihood of getting pregnant (OR= O.37, 95% CI: 0.19-0.77, p-value <0.01; AOR=0.36, 95% CI: 0.17-0.75; p-value <0.01). Violent parental attitude was found to be associated with adolescent pregnancy by increasing the odds to about twice in the unadjusted model and almost three times in the adjusted model. The odds of becoming pregnant in Model 1 were 2.32 (95% CI: 1.28-4.21, p-value <0.001). In Model 2, the odds increased to 2.93 (95% CI: 1.49-5.83, p-value <0.001). The ability of adolescents to confide in guardians about relationships was found to be statistically significant both at the bivariate and multivariate levels with the crude and adjusted odd ratios being almost same. Significance differences were also observed between feelings of being pressured by parents towards house upkeep financially and adolescent pregnancy in this study. Such pressure was found to predispose the adolescent to getting pregnant by as much as six times compared with those not pressured (OR=5.94, 95% CI: 1.74-20.33, p value <0.005). After adjusting for other covariates at the multivariate level, the effect remained similar (AOR =4.91, 95% CI: 1.06-22.86, p-value of <0.05) (Table 3).
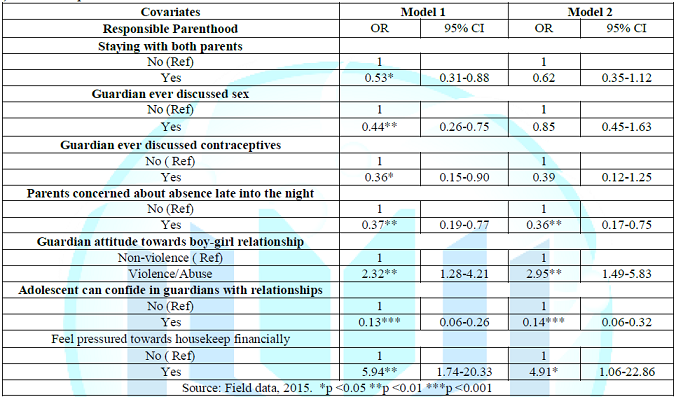
Table3: Regression of
responsible parenthood on the prevalence of adolescent pregnancy.
Peer
influence is a significant predictor of adolescent pregnancy in the study area.
There was a significant association between ones friend ever been pregnant and
the adolescent herself getting pregnant; an adolescent who had had a pregnant
peer was seven times more likelihood to get pregnant at the bivariate level
(OR=7.31, 95% CI: 4.08-13.11, p value <0.001). After adjusting for other
covariates, the predisposing effect still remained significant statistically.
The reaction of friends if one was pregnant was also seen to be associated with
adolescent pregnancy. It is seen to offer protection as a respondent whose
friend would be sad were she to be pregnant was significantly less likely to
get pregnant compared with those whose friend would be happy (OR=0.08, 95% CI:
0.04-0.18, p-value <0.001).
When the effects of other variables were held constant, reaction of friends still remained statistically significant in its association with adolescent pregnancy (AOR=0.17, 95% CI: 0.10-0.28, p-value <0.001). Who had never had pregnant friend(s) had significantly lower odds of getting pregnant (OR=0.44; 95% CI: 0.25-0.78, p-value <0.01). After adjusting for other covariates, the effect remained the same with the association still being statistically significant. (AOR=0.44, 95% CI: 0.25-0.76, p-value <0.01) (Table4).
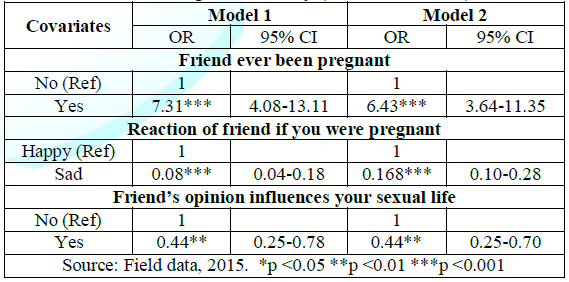
Table 4: Regression of peer
influence on the prevalence of adolescent pregnancy.
Discussion
Global statistics on adolescent pregnancy shows a huge public health challenge with a devastating consequence of increased maternal and infant mortalities particularly in rural settings of which Ghana is not an exception [5,10]. With a national prevalence of 14.0%adolescents residing in rural areas in Ghana, have a prevalence of 17%which is consistent with the finding in this study (17%versus 18%). There exist some relationships between predictors of socio-demographic and socio-economic characteristics on adolescent pregnancy as evident in this study that there was a higher odd to get pregnant within the late adolescent period. This finding is consistent with the situation in the United States where majority of the teen pregnancies were in the late adolescence period [12].
Being a student (currently schooling) showed high significance in the study with protection against the odds of getting pregnant by as much as hundred times. Education is known to increase the adolescence awareness about sexuality and avoidance of risky sexual behavior. As part of the consequences of adolescent pregnancy however is high school dropout rates, hence 6 (7.50%) of the cases in the study were school dropouts. The association between education and age at first pregnancy may be due to the possible delay of sexual activity by those still in academic pursuit or as a result of those getting pregnant, dropping out of the educational system before getting to secondary school level. This result supports findings from studies on the relationship between educational attainment and teenage pregnancy [13].
The statistical insignificance shown by the level of education attained by the respondents in the study could be due to the fact that the study being an unmatched case-control might have recruited more controls that are still in the lower age limits and are still attending the basic school. The education level of both guardians showed an association with adolescent pregnancy in the study. Mothers education level showed stronger protective association than the fathers. The finding relating female guardian education level is consistent with the findings of a similar study which showed that the education level of the adolescents mother is a predictor of adolescent pregnancy such that the higher the level, the lower the pregnancy rates [14]. This finding could also be attributed to the fact that the female adolescent in the rural areas of Ghana naturally spend much of her time with her mother and may therefore find it more comfortable discussing issues about her sexuality with the mother more than the father.
Early sexual unions emanating from cohabitation for economic reasons is increasingly gaining acceptance in the study area thereby predisposing adolescents to early pregnancy in the study area. In another study, a strong association between marital status/cohabitation and adolescent pregnancy was established [15]. About 63%of the cases were either married or cohabiting while none of the controls was in any form of sexual union. In such unions, there were early exposure to sex and hence pregnancy. In many countries, girls are married at a very young age while in others it is the age at the time of first intercourse where honor is given to young motherhood. Reasons why parents endorse such early marriages or sexual unions are varied. Inabilities to pay school fees by parents, avoidance of promiscuity, Sexually Transmitted Infections (STIs), and parents desire to obtain dowries have been cited to be among the key reasons. Again such early marriages are more common among adolescents with low levels of education [16].
The availability of household items of various kinds in the study area showed some association with adolescent pregnancy. Items such as television, electricity and ownership of motor bicycle were very significant predictors of pregnancy as most adolescent girls end up being sexually exploited whilst searching for these items predominantly from the opposite sex. The ability of the adolescents guardian to afford the payment of health services, travelling fares, and regular school supplies and clothes also showed a very strong association as a predictor of adolescent pregnancy in this study. Adolescent girls as observed in the study area have the desire to possess material things to enhance their look. In all these essential services/items, lesser percentages of the cases could afford them compared to the controls i.e. travelling fares (20.00% Vs 38.18%), health services (70.00% Vs 80.91%) regular school supplies (31.25% Vs 70.45%) and sufficient clothes (30.00% Vs 71.36%).
They will therefore go at all lengths in search of these hence are likely to be exposed to sexual relationships resulting to unplanned pregnancy. When the respondents were categorized into high and low socioeconomic classes, there was a strong association between socio-economic status and adolescent pregnancy with p-value of <0.001.Those in the high socio-economic stratum were protected and had lower odds of getting pregnant when compared with those in the lower socioeconomic class. This was consistent with a study which reported that teenage pregnancy is more common among girls who were less educated and had poor economic back grounds [17]. A similar reflection was seen in another study conducted in the United Kingdom where there was an increased sexual activity marked teenage pregnancy among girls who are living in economically deprived areas and families [18].
The adolescent-parent relationship was also observed as a predictor to adolescent pregnancy. In this study, staying with both parents was seen to be protective against adolescent pregnancy. About 61%of the controls were staying with both parents while less than half 45%of the cases were staying with both parents. The presence of both parents has been shown to be a factor in minimizing adolescent pregnancy with significant statistical difference among the cases compared with the controls. Having both parents around offers a high probability of warmth and proper monitoring being given to the adolescent. The adolescent female is likely to have most of her social and psychological/emotional needs catered for. This supports findings of a related study which observed that there is a strong negative impact of absence of one parent at home on early sexual initiation and adolescent pregnancy [19].
A little above half of the controls in this study had parents giving them sex education 129(58.64%) as compared with 31(38.75%) of the cases which showed a statistically significant difference in minimizing the odds of getting pregnant among the controls. This is in contravention with the societal perception that it could make adolescents who are not sexually active, start sexual experimentation and hence increase teenage pregnancy. The opposite however has been shown to be true in New York where sex education was not provided to the teens and as such was associated with highest rates of teen pregnancy [20]. The situation where parents concentrate on moral education and not sex education and more sadly even seeing sex education as a taboo needs some advocacy efforts to address this in rural Ghana since evidence has shown that parent-child communication that involves sex education and to large extent discussions on contraception are known to reduce teen pregnancy [21].
In this study, adolescent girls discussions with parents on contraceptives showed significant statistical difference between the cases and the controls. Adolescents who held such discussions were approximately 60% less likely to be pregnant compared with those who did not have. For example, in a multinational study across four countries to look at parental roles in adolescent sexual activity and contraceptive use, parent-child communication about sex-related matters was positively associated with contraceptive use for Ghanaian and Ugandan females and males but there was no association found between parents providing information about contraception and adolescents contraceptive use [22]. This is quite significant amidst the fact that it offered significant protection against pregnancy among the controls when compared with the cases. In another related study, the protective factors against pregnancy among others was parental supervision (OR =0.88, 95% CI: 0.81, 0.94) with the risk factor being if adolescent ever used drugs (OR =2.85, 95% CI: 2.57, 3.15) [23].
The attitude of parent/guardians towards boy/girlfriend relationship was also seen to have a significant predisposition to adolescent pregnancy. Adolescents who regarded their parents attitudes as being violent were at higher odds of getting pregnant. Adolescents who had ever suffered any violence (physical, verbal, etc.) are at higher odds of pregnancy (1.69 times) [24]. Such violent attitudes are likely to make adolescents recoil and find it difficult to open up to parents with their most sensitive sexual problems but rather result to their peers who inappropriately advises them compared to those who could confide in their parents/guardians to get matured good advices on sexuality and pregnancy prevention. In this study, parental demand for material and/or financial support from adolescent daughters tends to expose them to risky sexual behaviors hence pregnancy. In a similar study, adolescents girls whose parents never pressured them financially were significantly less likely to become pregnant compared to those constantly under pressure to support their parents financially since they are likely to resort to boyfriends and/or older men (economic and age disproportionateness) for transactional sex to help bridge such financial gaps [25]. Because of their vulnerability, they are likely to be unable to negotiate for safer sex hence end up with unwanted pregnancies and Sexually Transmitted Infections (STIs).
Peer influence on adolescent pregnancy cannot be overemphasized as adolescence is a period when peer influence is greatest. The observation in this study that about 60%of respondents among the cases have ever had a pregnant friend confirms some other research findings that adolescents, whose friends were sexually experienced, had higher odds of sexual debut [26]. The odds of pregnancy were higher among adolescents who believed they will gain respect by engaging in sex and by extension getting pregnant. The influence of peers offered protection against pregnancy by as almost 50%in this study. Having a pregnant peer significantly predisposed one to also getting pregnant. Although peer knowledge on contraceptives is believed to be misguided and inaccurate most times it is therefore recommended that exploring the use of peer educators as a source of information for contraceptive use could be useful predictor of preventing adolescent pregnancy in rural communities [27]. Additionally, advocacy for increased social/parental support for adolescents contraception use will also be helpful in complementing public health workers efforts in rural Ghana.
Ethical approval: Ethical clearance was obtained from the Kwame Nkrumah University of Science and Technology Ethics Review Board. Permission was also obtained from the Amenfi West District Assembly and Health Directorate.
Informed consent for participation and publication: Written and verbal informed consent was obtained from the parents/ guardians of the pregnant teenagers/ mothers and verbal consent from the teenage mothers below 16 years of age respectively. All participants agree to publishing the research findings anonymously.
Authors contributions: MTN conceptualized, designed the study and analyzed the data. EKA supervised the field work, EO reviewed the data analysis and provided technical advice and FYG drafted the full study report. All authors discussed the report, edited it together and approved the manuscript for final submission.
Acknowledgement
The
authors are grateful to the respondents and the Amenfi West District Health
Management Team for approving the study and for their corporations during data
collection.
References
2. ABC of counseling adolescents towards behaviour change Ghana Health Service (2008) (2nd Ed) Ghana 1-8.
3. Garfield B. Personality development of the adolescent: Peer group versus parents (2007) Sou Afri J Education 27: 177-190.
4. Coffey LT. Survey: Unprotected sex common among teens (2008) Today Parenting
5. 10 facts on adolescent health(2008) World Health Organization facts sheets
6. Adolescent pregnancy (2012) World Health Organization Fact Sheet 364.
9. Adesoka, J, Moses SA, Quagraine L and Siaw L. Incidence, causes and effects of teenage pregnancy among public JHS Girls in the WASSA Amenfi District in the Western Region of Ghana (2008) Undergraduate research project, University of Cape Coast Cape Coast, Ghana. https://doi.org/10.17660/th2017/72.1.6
10. Reproductive and Child Health (RCH) annual report (2010) http://www.mohghana.org/UploadFiles/Publications/GHS-Facts-and-Figures-2010_22APR2012.pdf
11. Teenagers in the United States: sexual activity, contraceptive use, and childbearing, national survey of family growth 2006-2008 http://www.cdc.gov/nchs/data/series/sr_23/sr23_030.pdf
12. Olausson OP, Haglund B, Weitoft RG and Cnattingius S. Teenage childbearing and long-term socioeconomic consequences: a case study in Sweden (2001) Family Planning Perspectives 33: 70-74. https://doi.org/10.1363/3307001
13. Diclemente RJ, Santelli JS and Crosby RA. Adolescent risk behaviours and adverse health outcomes (2009) Diclemente RJ, Santelli JS and Crosby RA (Eds), John Wiley & Sons, San Francisco, CA.
14. Minja KC, Shyam T, and Vinod M. Early marriage and early motherhood in Nepal (2005) Journal of Biosocial Science 37: 143-162. https://doi.org/10.1017/s0021932003006527
15. Birsen G, Aysun O and Mehmet Z. Determinants of adolescent pregnancy in an urban area in turkey: a population-based case-control study (2007) Journal of Biosocial Science 39: 301-311 https://doi.org/10.1017/s0021932006001763
16. Debbie MS and James E. Effects of area and family deprivation on risk factors for teenage pregnancy among 13–15 year old girls (2006) Psychol Health Med 11: 399-410. https://doi.org/10.1080/13548500500429353
17. Khairani O, Suriati H, Noor AM, Aida J, Syahnaz MH et al. Adolescent pregnancy outcomes and risk factors in Malaysia (2010) International Journal of Gynecology and Obstetrics 111:220-223. https://doi.org/10.1016/j.ijgo.2010.06.023
18. www.fpq. com.au/pdf/ WDForum_BriggsSpeech.pdf
19. Renee ES, Marla EE, Sandra P and Carol S. Examining the relationship between adolescent sexual risk-taking and perceptions of monitoring, communication, and parenting styles (2006) Perspectives on Sexual and Reproductive Health 38:13-19.
20. Ann B, Awusabo-Asare K, and Akinrinola B. Role of Parents in Adolescent Sexual Activity and Contraceptive Use in Four African Countries (2009) International Perspectives on Sexual and Reproductive Health 35: 72–81. https://doi.org/10.1363/3507209
21. Siziya S, Muula AS, Rudatsikira E and Ogwell AE. Prevalence of sexual intercourse among school going adolescents in Coast Province (2007) Tanzania Health Research Bulletin, Kenya 9: 159-163. https://doi.org/10.4314/thrb.v9i3.14322
22. Nicola JC, Rachel KJ, Kristin LD, Frances M, Nwabisa JS et al. Risk factors for unplanned and unwanted teenage pregnancies occurring over two years of follow-up among a cohort of young South African women (2014) Glob Health Action 7: 23719. https://doi.org/10.3402/gha.v7.23719
23. Stella B, Oleko BT, and Claudia V. Parental Factors and Sexual Risk-Taking among Young People in Côte dIvoire (2005) African Journal of Reproductive Health 9:49-65. https://doi.org/10.2307/3583160
24. Akers AY, Do MAG, Bost JE, Adimora AA, Orr PD et al. Variation in sexual behaviors in a cohort of adolescent females: The role of personal, perceived peer and family attitudes (2011) Journal of Adolescent Health 48: 87-93. https://doi.org/10.1016/j.jadohealth.2010.05.004
25. Bankole A, Biddlecom A, Guiella G, Singh S and Zulu E. Sexual behavior, knowledge and information sources of very young adolescents in four sub-saharan African countries(2007) African Journal of Reproductive Health 11: 28-43.https://doi.org/10.2307/25549730
26. Awusabo-Asare K, Abane AM and Kumi-Kyereme K. Adolescent Sexual and Reproductive Health in Ghana: A Synthesis of Research Evidence (2006) Occasional Report, The Alan Guttmacher Institute, New York.
27. Luke N. Confronting the Sugar Daddy stereotype: age and economic asymmetries and risky sexual behavior in urban Kenya (2005) International Family Planning Perspective 31: 6-25. https://doi.org/10.1363/3100605
*Corresponding author
Fred Yao Gbagbo, Department of Health Administration and Education, Faculty of Science Education, University of Education, Winneba, Ghana, Tel: +233(0)243335708, Email: gbagbofredyao2002@yahoo.co.uk
Citation
Naziru TM, Gbagbo YF, Agbeno KE and Otupiri E. Review of socio-demographic and economic predictors of adolescent pregnancies in rural Ghana (2019) Nursing and Health Care 4: 38-43.
Keywords
Socio-demographic, Socio-economic, Predictors, Adolescent-pregnancy, Ghana.
