
 PDF
PDF
History
Tracheostomy is among the oldest surgical procedures and has been known for over 5000 years. It has been noted on Egyptian stone tablets which are dated some time around 3600 BC. It has also been mentioned in ancient Hindu canonical texts such as the Rigveda (2000 BC.) It was also known to the ancient Greek and Roman physicians. Asclepiades from Bythinia was probably the first known individual to have performed a tracheostomy in 100 BC. The first successful tracheostomy was described by the Italian physician Antonio Musa Brasavola in 1546. Up until the 18th century it was occasionally used but only after 1820. did it become a widely used and well recognized surgical procedure. After the report by P. Bretonneau about successful treatment of a laryngeal obstruction due to dyphtheria, tracheostomy became more popular as a treatment option, however still as a last resort measure.
Surgical tracheostomy as we know it today, was first described by C. Jackson in 1909 [1]. The technique was somewhat changed in the 1940s during the poliomyelitis epidemic, but it is still essentially the same as the technique in use today. Throughout the period between 1500. and 1833. only 28 successful tracheostomies have been reported. During this time period, the mortality rate from the procedure was 70%.
Surgical tracheostomy is the most common surgical procedure in the intensive care unit (ICU), on patients who require prolonged mechanical ventilation. Percutaneous tracheostomy (PT) was first described by Shelden et al. in 1957 [2]. In 1967, Toy and Weinstein described the Seldinger approach.
In 1985, Ciaglia et al. presented the percutaneous dilational tracheostomy (PDT), a technique which utilises a needle, guide wire and subsequent dilation of the entry tunnel with several incrementally wider dilators [3].
In 1989, Schachner et al. presented the Rapitrac, a dilational surgical instrument which uses a sharp point to quickly access the trachea through a guidewire, hence forming an opening for the tracheal cannula [4].
Next year Griggs et al. presented a similar technique (GWDF, guide wire dilating forceps) and a new Rapitrac which in contrast to the older one, did not have such a sharp point, thereby reducing the likelihood of bleeding and severe trauma [5].
Procedure
Percutaneous tracheostomy is not indicated in an emergency setting [6]. It is most commonly a bedside procedure in the ICU when the patient is under analgesia, sedation, occasionally relaxation and strictly monitored [7]. Immediately prior to the procedure, the patient is preoxygenated with 100% oxygen and this inspiratory concentration is maintained throughout the procedure, until the cannula is firmly in place, until we are sure that there is no airway obstruction and the blood oxygen saturation is satisfactory. The neck is prepared in accordance with surgical asepsis techniques as for any other surgical procedure. Note must be made of the adequate size of the surgical field so that the individual performing the procedure may comfortably and reliably palpate the landmarks (mm sternocleidomastoideus, incisura jugularis, cartilago thyroidea, cartilago cricoidea, cartilago trachealis) (Picture 1).
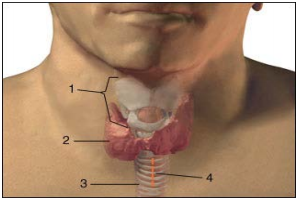
The puncture site is most commonly the fibromuscular part of the trachea, between the second and third tracheal cartilaginous rings. It is most easily located by moving the index finger from the laryngeal prominence and in the mid line descending down to the second tracheal cartilaginous ring. The laryngeal prominence is more emphasized in men (Adams apple) and there is less subcutaneous fatty tissue in men. In any condition with thyroid enlargement, when the thyroid isthmus is close to the puncture site, it is wiser to perform a surgical tracheostomy in which the surgeon can visualise each layer of tissue in advancing deeper towards the trachea.
Even when the initial puncture is uneventful, all of the subsequent procedures such as tissue dilation with instruments, may cause a concealed haemorrhage (Picture 1).
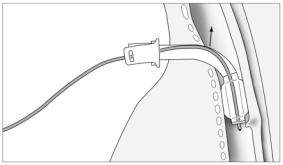
In the planned site of puncture, a transversal incision of the skin and subdermis, of approximately 1.5-2 cm in length, is made. The skin and subdermal tissue contain small arteries and veins which may bleed during the incision. Most commonly it will suffice to gently compress the bleeding vessel and wait for the coagulation mechanism to stop the bleed. If this does not suffice, sometimes it may be necessary to ligate or cauterize the vessel. Just before incision, the area is usually anaesthetized with 3-5 ml of 1% lidocaine with adrenaline (1:200000) to minimise the bleeding. Puncture is performed using a 14G needle with a plastic cannula, which remains in the trachea after the needle is pulled out. We must keep in mind that the trachea is most often quite superficial and usually just 1 cm under the skin, so caution must be exercised during puncture in order to avoid pushing the needle too deep and puncturing the vessels beneath the trachea, such as the brachiocephalic trunk, which may cause a potentially fatal haemorrhage. Anterior and superficial to the trachea, sometimes there is thyroid tissue and it also can bleed profusely. The direction of the needle is perpendicular to the skin. During puncture the position of needle insertion depth is verified by aspiration of air from the trachea into the syringe, which is usually filled with normal saline (Picture 2).
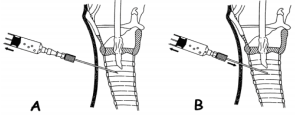
The appearance of air in the syringe which is prefilled with normal saline, is an indicator of correct position. The endotracheal tube, which was retracted approximately 2-3 cm prior to incision, is gently rotated 30 degrees to either side after puncture, to make sure that the needle did not puncture the endotracheal tube. The aspiration test will not distinguish the lumen of the tube from that of the trachea. Once the correct intratracheal position is confirmed, a guidewire is inserted through the plastic insertion cannula and is left in place while the small insertion cannula is removed (Picture 3).
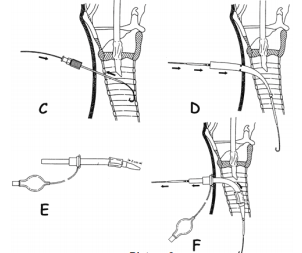
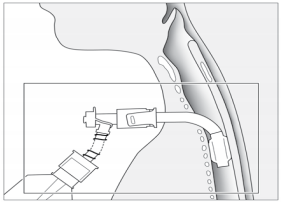
Up to this point, both of the most common techniques are essentially the same. Ciaglias technique further recommends a blunt dissection of the tracheal aperture via a rigid plastic dilator of a smaller diameter. After this dilation, a cone shaped dilator is inserted over the guidewire and is inserted up to the marked line which indicates that the aperture is wide enough for insertion of the cannula. A cone shaped catheter is inserted through the cannula with its tip coming slightly out in front of the cannula and this serves for easier passage of the cannula through the tracheal aperture. The cannula with the catheter is inserted over the guidewire and once the cannula is in the right position, the guidewire and catheter are removed from the cannula and the cannula remains in place (Picture 3).
Griggs technique forms an initial stoma with the aid of a plastic dilator and the uses a special speculum like forceps which is placed over the guidewire into the trachea and is then widened causing a blunt spreading of the tracheal tissue and thus a widening of the aperture (Pictures 4 and 5).


Both techniques may require significant physical force because the surrounding tissue may prove to be quite resistant to blunt dissection. Once the tracheal aperture is assessed as sufficiently wide and appropriate in shape, the tracheostomy cannula is inserted. The cannula must be well lubricated with gel so it can easily bypass the tissue around the aperture. A problem which may arise while passing the cannula through the trachea is when the rigid tracheal cannula tip gets stuck or encounters the tracheal rings en route. If the curved introducer is inserted in through the cannula, it will curve the cannula and make its passage easier along the tracheal rings and further through the trachea. Another problem which may potentially arise is the necessity of extraction of the guidewire prior to cannula insertion and subsequent possibility of paratracheal cannula insertion. In younger patients with a more firm trachea and well formed aperture there are usually no significant difficulties in inserting the cannula without the guidewire in situ, however, in older patients sometimes it is almost impossible to insert the cannula without the guidewire. The problem should be solved once the manufacturers make an additional opening for the guidewire through the curved introducer which goes into the cannula, so the guidewire will not have to be removed. When advancing the cannula through the trachea, caution must be exercised in following the curvature of the wire which follows the anatomical curvatures of the aperture and trachea. The guidewire may also be contorted immediately below the tip of the cannula if the cannula tip is at a steep angle in relation to the guidewire, that is why it is necessary to slightly and gently move the guidewire in and out while advancing the cannula into the trachea, to ensure it has not curved and has remained mobile. This same maneuvre is recommended while performing tracheal aperture dilation with the forceps in Griggs technique.
After inserting the tracheal cannula, the trachea should be suctioned and with an aspiration catheter. The cuff should be inflated with attention to cuff pressure and ventilation may commence via the cannula. The endotracheal tube is removed and hygiene of the oral cavity and upper airways is performed. Cannula position and patency is verified by auscultation, chest –xray and fiberoptic bronchoscopy. Fiberoptic bronchoscopy before, during and after tracheal cannula insertion will give a complete insight into the condition of the trachea and envisage any potential complications (bleeding, tracheal wall lacerations, tracheal cartilage trauma or rupture) in a timely manner.
Complications of the Procedure
The time needed to carry out a percutaneous tracheostomy has become important in assessing the success of this technique in comparison to other techniques. The inability to adequately dilate a traheal aperture, increased number of attempted dilations (more than one attempt) and prolonged cannula insertion time are indicators of complications and they are indicative of categorizing a tracheostomy as insufficiently dilated. It is necessary to mention the complication of tracheal cannula obstruction with consequential desaturation of arterial oxygen which can occur a few days after successful percutaneous tracheal cannulation (usually occurs between day 2 and 21 post tracheostomy). Partial obstruction may occur due to the weight of the cannula itself and the weight of the tubing connected to the respirator. When a patient is in the supine position for a prolonged period of time, there is usually some degree of lateral deviation of the cannula due to the continued traction by the hosing system on the side of the respirator, while in seated patients who require mechanical ventilation support, the cannula usually deviates downwards. The weight of the whole system causes the cannula to deviate in position and the walls of the cannula are no longer in alignment with the walls of the trachea
Obstruction occurs for two reasons. Tracheal wall trauma makes the wall of the trachea softer and easy to deform so the deviation of the cannula and the traction on the tissue causes mucosal folds to appear in front of the cannulas meatus thereby causing a partial obstruction to the free flow of air. The same happens when the cuff of the cannula deflates or loses its elasticity and movement of the cannula causes a cuff herniation and consequential partial obstruction of the airway (Picture 7).
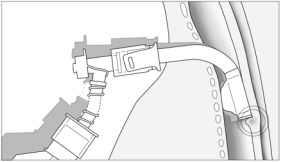
In scenarios where there is a desaturation of arterial oxygen content it is always prudent to perform a fiberoptic bronchoscopy however it is not always easy to ascertain the problem due to the fact that when a fiberoptic bronchoscope is inserted, the cannula is usually straightened and the obstructions may disappear in that moment (Picture 8).
The problems and solutions were discovered empirically, while performing airway suction and cleaning maneuvres. It was noticed that in certain positions of the cannula there was an occurence of desaturation and return to normal values when the cannula was repositioned (Picture 6).
Advantages of Percutaneous Tracheostomy
The advantages of percutaneous tracheostomy need to be considered in comparison to classic surgical tracheostomy. Outcomes and results of numerous studies which have been comparing various techniques mostly depend on study designs and observed parameters. Even though there are no definite and conclusive results meta analyses of studies suggest that percutaneous tracheostomy is less time consuming, less traumatic, associated with fewer intraoperative and postoperative complications and is more cost effective than a classical surgical tracheostomy [8]. Note must be made of the studies which conclude that percutaneous tracheostomy showed more periprocedural complications, especially those studies that mention fatalities and cardiac arrest. These meta analyses were made on the basis of all percutaneous tracheostomies irrespective of the technique used [9].
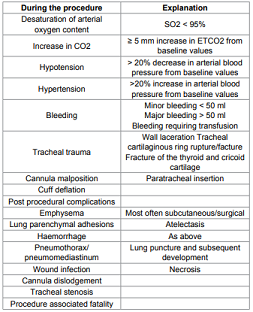
Outcomes and results also differ between the techniques of percutaneous tracheostomy. Griggs GDWF method, is somewhat less time consuming whereas for the associated bleeding which is During the procedure Explanation Desaturation of arterial oxygen content SO2 < 95% Increase in CO2 ≥ 5 mm increase in ETCO2 from baseline values Hypotension > 20% decrease in arterial blood pressure from baseline values Hypertension >20% increase in arterial blood pressure from baseline values Bleeding Minor bleeding < 50 ml Major bleeding > 50 ml Bleeding requiring transfusion Tracheal trauma Wall laceration Tracheal cartilaginous ring rupture/facture Fracture of the thyroid and cricoid cartilage Cannula malposition Paratracheal insertion Cuff deflation Post procedural complications Emphysema Most often subcutaneous/surgical Lung parenchymal adhesions Atelectasis Haemorrhage As above Pneumothorax/ pneumomediastinum Lung puncture and subsequent development Wound infection Necrosis Cannula dislodgement Tracheal stenosis Procedure associated fatality Table 1: Complications. Apparently more incidental with GWDF and apparently more pronounced hypotension there is no statistical confirmation [10]. Both techniques are equally reliable when observing the overall outcome with a differential emphasis on increased peak airway pressure with GDWF and tracheal ring fracture in Ciaglias technique, however without statistically significant difference. Most studies failed to find significant differences between the two techniques [11].
All comparisons, between classical surgical and percutaneous tracheostomies and between percutaneous tracheostomy techniques, put a significant emphasis on the skills of the operator carrying out the procedure [12]. There was a significant reduction in the rate and severity of complications if the operator had more experience with 15 or more successful previous tracheostomies.
In the Clinical department of Anesthesia, Reanimation and Intensive Care Medicine at University Hospital Dubrava, we have performed 250 percutaneous tracheostomies through 10 years. We have applied both of the mentioned techniques and have even combined the two techniques to make a third separate technique. Among the complications were ten minor bleeds, three were converted ultimately to a classical surgical tracheostomy due to bleeding from the thyroid and a few of the patients experienced an increase in arterial blood pressure during the procedure. There were no instances of oxygen desaturation in any of the cases. Four of the patients died a month after the procedure with the tracheostomy cannula in situ. These were one neurosurgical, one maxillofacial and two cardiosurgical patients respectively.
Conclusion
We consider that tracheostomies are a vital element of the intensive care treatment armamentarium irrespective of the technique used. They are recommendable as treatment options for patients who require prolonged mechanical ventilation. They are very effective, easily performed and should be a required skill for all intensive care physicians. Experience in indicating the procedure and appropriate timing are equally as important as the manual skill in performing the procedure. We recommend an early consideration for the procedure, preferably within a week if there is no anticipated likelihood of weaning from mechanical ventilation and extubation, in order to reduce the risks associated with prolonged intubation. As with every invasive procedure, percutaneous tracheostomies have their advantages and complications. Based on the discussion in this review, especially considering the advantages in comparison to a classical surgical tracheostomy, we can recommend percutaneous tracheostomy as a safe and effective method of treatment, however with a note that a classical surgical tracheostomy still has its indications and should always be considered with regard for the safest treatment option for the patient.
References
1. Jackson
C. Tracheostomy. (1909) Laryngoscope 19:285-290.
2. Shelden CH, Pudenz RH, Tichy FY. Percutaneous tracheotomy. (1957) J Am Med
Assoc 165: 2068-2070.
3. Ciaglia P, Firsching R, Syniec C. Elective percutaneous dilatational tracheostomy.
A new simple bedside procedure; preliminary report. (1985) Chest 87:715-719.
4. Schachner A, Ovil J, Sidi J, Avram A, Levy MJ. Rapid percutaneous tracheostomy
(1990) Chest 98: 1266-1270.
5. Griggs WM, Worthley LI, Gilligan JE, Thomas PD, Myburg JA. A simple percutaneous
tracheostomy technique. (1990) Surg Gynecol Obstet 170: 543-545.
6. Ciaglia P. Improving percutaneous dilational tracheostomy. (1997) Chest 112:
295.
7. Fantoni A, Ripamonti D. A non-derivative, non-surgical tracheostomy: the
translaryngeal method. (1997) Intensive Care Med 23: 386-392.
8. Polderman KH, Spijkstra JJ, Remco de Bree, Christiaans HMT, Gelissen HPMM,
et al. Percutaneous Dilatational Tracheostomy in the ICU* Optimal Organization,
Low Complication Rates, and Description of a New Complication. (2003) Chest.
123: 1595-1602.
9. Dob DP, McLure HA, Soni N. Failed intubation and emergency percutaneous
tracheostomy. (1998) Anaesthesia 53: 72-74.
10. Añón JM, Gómez V, Escuela MP, De Paz V, Solana LF, et al.. Percutaneous
tracheostomy: comparison of Ciaglia and Griggs techniques. (2000) Crit Care 4:
124-128.
11. Basaranoglu G, Erden V. Failed intubation due to posterior fossa haematoma requiring
emergency percutaneous tracheostomy (2002) Br J Anaesth 88: 310-311.
12. American Society of Anesthesiologists Task Force on Management of the Difficult
Airway. Practice guidelines for management of the difficult airway: an updated
report by the American Society of Anesthesiologists Task Force on Management of
the Difficult Airway. (2003) Anesthesiology 98: 1269-1277.
*Corresponding author
Anđelko Korušić, Department of Anaesthesiology, Reanimatology and Intensive Care, University Hospital Dubrava, Av. Gojka Šuška 6, 10000 Zagreb, Croatia, Tel: 385 1 2902797/+385 98 358262; Fax: 385 1 2902793 E-mail: akorusic@gmail.com
Citation
Korušić A, Đuzel V, Jeleč V, Nikolić I, Župčić M, et al. (2016) Percutaneous Tracheostomy – Advantages and Complications. NHC 103: 14-18
Keywords
Percutaneus Tracheostomy
