
 PDF
PDF
Introduction and Background of the Study
Women comprise nearly half of the 40 million people living with HIV/AIDS and constitute the majority of the group with new HIV infection in the world [1-4]. The interrelationship between domestic violence and spread of HIV/AIDS significantly explains the paradigm as an issue of public health concern in the control of HIV/AIDS [5,6]. Although men also experience domestic violence women have been found to suffer effects of domestic violence pertaining to health more than men as biologically domestic violence has been found to exacerbate HIV transmission in women than men due to the larger surface mucus membrane exposed by women during sex than men, higher transfer of fluids from men to women and the higher viral load in male fluids [7,8]. Different studied paradigms explain the link between intimate partner violence (IPV) and HIV/AIDS and this can be examined in 3 ways: through forced sex with an infected partner; or compromised negotiation for safe sex and or increased risk for sexual risk behaviors [4]. The 1992 British crime survey established that less than 4% of women over 60 years of age reported any form of physical violence in their relationships compared to 17% from their counterparts between 18-24 years. This is in line with the Scottish police which reported 1.2% cases of domestic violence from an old person above 60 years. However data from the British crime report 2001 showed that the 50 years and above are more likely to recognize domestic violence as abusive compared to the age group 16-24 years hence revoking the view that the 50 years and above old were more likely to accept domestic violence for failure to recognize it as abusive [9].
Statement of the problem
In Uganda studies on domestic violence have provided the estimates of domestic violence among the age group 15-49 years. Koening [10] found that 70% of men and 90% of respondents justified wife beating to burnt food, if the spouse left house without consent from the husband, neglect of children or refused to have sex. It seems hard for the 50 years and above olds to seek help when faced with domestic violence as services available do not meet their needs and care givers seem to neglect their needs. Domestic violence is blamed for exacerbating HIV/AIDS spread as it compromises women to make decisions on safe sex practices [4]. The Ugandan government has recognized domestic violence as abusive and exploitative and to curb domestic violence the government of Uganda has adopted the Domestic Violence Act 2010 that allows the incidence of domestic violence to be prosecuted under the general penal code as assault or homicide. In addition a revised law has been drafted by government that handles issues of domestic violence, marriage and divorce that a person in a domestic relationship who engages in domestic violence commits an offence and is liable on conviction or to a fine not exceeding forty eight currency points or imprisonment not exceeding two years or both and the court may, in addition to imposing a fine or imprisonment, order the offender in a case of domestic violence to pay compensation to the victim of an amount deemed fit by court. However the 50 years and above PLWH have different needs from the age group 15-49 years were most of the research on domestic violence has been centered [11]. Understanding of domestic violence issues and integrating them in the current treatment regimens is critical for success of treatment regimens of the 50 years and above old PLWH as domestic violence is blamed for hampering adherence to ARVS and ART, condom use among others [7]. Church of Uganda Mukono hospital is offering HIV/AIDS programmes that target 50 years and above old. However understanding factors associated with domestic violence among the 50 years and above PLWH and integrating them in their treatment is a critical component in the success of interventions which include: offering of ARVS, screening, testing and diagnosis and home based care. However no research has been done in regard to factors associated with domestic violence among the 50 years and above PLWH.
General objective
The general objective of the study was to identify the factors associated with domestic violence among the 50 years and above old population living with HIV/AIDS.
Specific objectives
- Establish the individual/background factors associated with domestic violence among the 50 years and above of age population living with HIV/AIDS.
- Define the socio-economic factors associated with domestic violence among the 50 years and above of age population living with HIV/AIDS.
- Find out the influence of substance of abuse associated with domestic violence among the 50 years and above of age population living with HIV/AIDS.
Research Questions
What individual/background factors associated with domestic violence among the 50 years and above of age population living with HIV/AIDS?
What are the socio-economic factors associated with domestic violence among the 50 years and above of age population living with HIV/AIDS?
What is the influence of substance abuse associated with domestic violence among the 50 years and above of age population living with HIV/AIDS?
Significance of the study
The study is expected to be used by CoU to design appropriate policies that can curb domestic violence among the 50 years and above of age and hence limit its drive of HIV/AIDS. The study is expected to be used by policy makers to design policies that can combat the level of domestic violence among the 50 years and above of age PLWH so as to curb its effect on the current treatment regimens. The study is an informative report that is expected to be used by gender activists to advocate for the integration of variables associated with domestic violence in the planning and designing of treatment regimens of the 50 years and above PLWH. The study is expected to be used by the above 50 years PLWH to reflect on their relationships and hence improve them to combat domestic violence and HIV/AIDS.
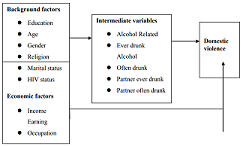
Conceptual framework
In the conceptual frame work above, individual or background and economic factors interplay with intermediate factors to cause the outcome (domestic violence) though background and economic factors can act independently of intermediate factors to cause domestic violence. Intermediate factors like alcohol consumption are risk factors of domestic violence however the older the person the less likely that they are to get involved in heavy alcohol consumption which is likely to lessen episodes of domestic violence.
Justification for the study
Despite the fact that domestic violence is blamed to exacerbate HIV/AIDS [5], present research on domestic violence has been centred among the age group 15- 49 years and hence has not unearthed factors associated with domestic violence among the 50 years and above of age PLWH. However domestic violence affects the treatment regimens of the above 50 years of age PLWH through compromised decisions for women on safe sex practices and adherence failure to ARVS [4]. Hence it is critical to establish factors associated with domestic violence among the above 50 years PLWH so as to address domestic violence issues that affect the treatment regimens of the 50 years and above of age PLWH.
Literature Review
There is no single variable that can independently explain the cause of domestic violence and research has advanced an interrelatedness of factors to aid understanding of domestic violence in context of specific societies and communities. Several cultural and institutionalized cultural factors account for domestic violence in cultural and institutional specific areas and thus cultural, economic, legal and political factors significantly cannot for domestic violence which is stirred by the unequal power relationships [3]. Furthermore factors responsible for the unequal relationships include social economic factors and dynamics, fear and control over female sexuality, family institution and structure where power relations are enforced as patriarchal, belief in male superiority over female and male inheritance, legislations and cultural barriers and sanctions that bar women from legal recognition and status for instance owning land and property and k that deprive women from economic independence.
Predisposing factors for domestic violence
Economic factors
Heise argues that the link between lack of economic resources and domestic violence is circular and operates in an endless chain that resource stricken women accept low paying employment, fail to secure employment and settle for home exploitative work that deprive them of economic independence that keeps them in violent and abusive relationships. However high violence levels are found in relationships of economically independent women as men use sex violence to subdue women in order to assert their manhood and authority over economically independent women, men use sex violence as a weapon to subdue women and this is specifically true when the male partner is unemployed and feels that his power is threatened in the household.
Cultural factors
Cultural factors provide justification for wife beating in some circumstances as in developing countries culture places men as family heads and household decision makers which is an irony that subdues women as subordinates to men that denies them property rights and making them dependent. Traditional culture ranks women as inferior to men that a man is justified to divorce and remarry while it is abominable for a woman to divorce her husband even when faced with violence a tradition that compels women to be submissive to men [12]. In addition women are ranked inferior to men that concur with Uganda Demographic Health Survey 201, that found that 44% of men compared to 58% of women justified wife beating where the most reported justification for wife beating was wife neglecting children that was reported at 45% compared to 56% in 2006. Other causes of domestic violence reported by the survey were wife going out without consent from her husband although the percentage of women who justify wife beating when a woman denied her husband sex fell to 22% in 2011 from 31% in 2006 while of women who justify wife beating when a wife prepared food badly declined to 17% in 2011 from 23% in 2006. Wife beating remains profound from African societies and stems from the cultural orientation which ranks men above women and that regards women as inferior to men and hence required to seek consent from their husbands before going anywhere. Women are required to look after children, prepare food and sexually serve their husbands against their consent [13].
Education of women
Findings from the UDHS [14] indicate that wife beating is highly justified and legitimate among women with primary education than their counterparts with post-secondary education and among households with low income levels which concurs with Rani et al. [13] who in analyses of data sets of Demographic Health Surveys from seven countries including Uganda, Malawi, Benin, Ethiopia, Rwanda, Zimbabwe and Mali used a multivariate analysis to identify factors that where significantly associated with wife beating and found that the likelihood of support for wife beating was low among women with post-secondary education across the seven countries than women without formal education .
Denying a husband sex
The Uganda Demographic Health survey 2011 highlighted that wife beating is justified when a woman declines to offer sex to her husband that was reported at 22% in 2011 compared to 33% UDHS, [15] survey findings which is still high which affirmed that women are not in full control of their bodies. Decisions on sex are highly dictated by men were refusal to offer a husband sex provokes an episode of domestic violence according to Worlds women and Girls data sheet 2011 which reported that 31% of Ugandan women compared to 19% of Ugandan men having condoned wife beating when a wife refused to give her husband sex. However, understanding attitudes and beliefs between women and men behind wife beating and domestic violence is a critical component in investing domestic violence as it determines acceptability and reporting.
Perception of a male partners HIV/AIDS status
Perception of a male partners HIV/AIDS status is a predisposing factor that exacerbates domestic violence. Koening et al. [10] who found that women who were somewhat likely to perceive their male partners as HIV positive had OR= 1.84, 95% CI= 1.45-2.33, P= 0.000 to experience domestic violence while women who perceived that their male partners were very likely to have been exposed to HIV/AIDS had OR=3.72, 95% CI= 2.81- 4.92, P= 0.000 compared to women who did not know the HIV status of their husbands who recorded OR=1.05,95% CI= 0.85- 1.29, P= 0.675 thus the perception of a male partners HIV status is a significant predisposing factor for domestic violence.
Length of current relationship
Koening et al. established an inverse relationship between odds for domestic violence and period of current relationship where short relationship periods were associated with higher odds of domestic violence compared to longer relationship periods which were associated with relatively lower odds for domestic violence. Hence as relationship period increases the odds for domestic violence decrease this means that orientation about the relationship changes.
Relationship to most recent partner
Koening et alin the same survey established that in relationships where women are in a wife - husband relationship the odds for domestic violence were 1 compared to a relationship were it is consensual OR=1.32, 95% CI=1.05-1.67, P= 0.020 and OR= 0.41, 95% CI= 0.30-0.56, P= 0.000 where a relationship was a boyfriend relationship. Thus odds decrease with recognition of a husband - wife relationship and this can be partly attributed to the nature of the husband - wife relationship hence understanding the attitudes and nature of the relationship is critical in explaining the limited violence in the relationship. However, Koening in his study focused on the age group 15-49 years and neglected the above 50 years who have different needs compared to the age group 15-49 years.
Number of living children
Koening et alfound that women with 0-1 child had 1 odd to experience domestic violence compared to women who had 2-3 living children who had OR=0.85(95% CI 0.68-1.07) P= 0.161 compared to women who had 4-5 living children who had OR=0.87 (95% CI 0.65-1.16) P= 0.344 and compared to women who had at least 6 living children who had OR=0.64,95% CI= 0.45-0.91,P= 0.012. Hence odds of living in violent relationships decreased with increase in number of children living .
Womans age at first intercourse (Years)
Koening et alestablished that a womans age at first intercourse significantly predicted domestic violence as women who had their first sexual intercourse before 15 years had OR=1.93 95% CI=1.47-2.52, P= 0.000. Women who had their first sexual intercourse between 15-17 years had OR=1.58, 95% CI= 1.24-2.03, P= 0.000 odds for living in violent relationships as compared to odds of women who had their first sexual intercourse at least at 18 years who had 1 odd for living in violent relationships. However Koenig did his study in Rakai district which is rural thus the sample size having different attitudes, knowledge, education and exposure compared to the urban setting were this study is centered. However the Rakai study was done in Rakai which is a village setting where people have different knowledge and attitudes from people in the urban setting.
Consumption of alcohol
Koening et al established that a womans consumption of alcohol significantly predicts domestic violence at OR= 1.22, 95% CI= 3.44-6.21, P= 0.042 compared to those who did not consume alcohol. In addition alcohol and illicit drugs like marijuana and Viagra arouse sexual urge that under the influence of illicit drugs, users lose conscience and may not know that they are committing violence against their partners which drives sexual violence against women. In Canada an examination of perpetrators of gender based violence almost found that 40% had consumed multiple substances like cocaine, marijuana and gamma hydroxybutyrate which induce men to sexually abuse their partners Canadian Panel on violence against women, 1993.
Childhood history, experience and witness of domestic violence
Childhood sexual abuse is an act of violation of childrens rights through domination and use of power over children. The abuser uses his position of power and authority over the child to subdue the child to sexual violence. The abusers position and knowledge is higher than that of the child as the child depends on the adult for affection. Thus the abuser exploits the power difference to subject the child to sexual violence. This can be through coercion hence any time a child is sexually abused there is coercion [16]. This builds in the child that he recognizes violence as legitimate that he does it in adulthood. A child who was exposed to sexual violence or witnessed his mother or relatives being exposed to sexual violence is likely to subject violence to others in adulthood as revenge or because of the feeling that women have no right to refuse sexual acts [17]. This justifies that the above 50 years are not free from sexual violence though research has mainly focused on the age group above 15-49 years.
Level of domestic violence among adults above 50 years of age
Domestic violence is prevalent in both low, middle income and developed nations of the world. It happens that the rates of domestic violence in Europe and Eurasia are synonymous to those recorded in other parts of the world. A systemic review on worldwide prevalence by the WHO [18] reported that women having experienced domestic violence from a romantic partner in Philippines and Paraguay ranged from 10% to 67% in Papua New Guinea and Nicaragua. 1.3-3% in United States and Canada. However it is imperative to note that concern could be taken when reporting prevalence of domestic violence as evidence has shown that there is underreporting of episodes of domestic violence due to stigma, fear of more possible episodes of domestic violence from the perpetrator and at times fear of rejection from family members and the community [19,20]. Level of domestic violence may vary between regions due to the differences in methodologies employed; the way people perceive violence and their willingness to disclose violence and abusive actions to researchers and hence caution could be taken when interpreting low rates of domestic violence in a particular region. Population surveys have documented that a very small population of women survivors of domestic violence come to the attention of authorities and service providers [20,21]. This concurs with survey findings from the Europe and Eurasia on domestic violence which found that only 1-20% of survivors of domestic violence reported to police or social health workers. Thus estimates of domestic violence do not give realistic approximation rates of the phenomenon as many women suffer in silence due to fear of stigma however domestic violence has been reported at 5% in New Zealand to 81% in Egypt [3]. In Bucharest 28% of women hospitalized women were being beaten by their romantic partners [22]. However under reporting is synonymous as many survivors were found not to seek assistance from authorities due to fear of potential violence from the perpetrator. Studies on domestic violence try to quantify the prevalence of domestic violence among the abused and statistics have found that women who are subjected to domestic violence experience a range of abuses including physical, emotional, financial and sexual abuses. However it was found that women fail to report the frequent abuses they suffer on a regular basis [23,24]. Studies in Uganda concur with global trends on the burden of domestic violence, a study in Uganda found out that 68% of ever married women aged between 15 and 49 years experienced domestic abuse from an intimate partner [15]. However, in Uganda there is under reporting as a number of cases of domestic violence are not reported due to fear of prosecution of the perpetrator as victims could be depending on the perpetrator [25].
Understanding of domestic violence at the international level
At the global arena domestic violence came to the limelight during the first Womens conference Decade (1975-1985) and in the nineties it turned into a major focus at the international fora. The Vienna conference on human rights in 1993 identified that even though domestic violence manifests in the family domain it is an abuse of human rights and this was developed by the Belem do para Convention of the organization of American states in 1994 which gave birth to the designation of the Inter American courts for survivors of domestic violence. These treaties and codes have developed mechanisms, policies and frameworks that help to define domestic violence cases and how to deal with cases to hinder subsequent occurrences however confusion and loopholes are still manifested in the way populations perceive and interpret domestic violence in South America, analysis on institutional feedback has given contradicting results, in Venezuela for instance, domestic violence is only considered when there is a stable relationship. In Brazil domestic violence is not considered when it is between concubines and unmarried spouses. Controversies manifest on to which call points to use to address domestic violence as counselors are used to counsel perpetrators and survivors to prevent further occurrence instead of seeking medical and support from legal authorities. This is adopted to minimize legal costs that would be incurred by the perpetrators. In numerous cities societal approaches had been used to help out battered women as temporary shelters would be constructed where they would get help [26]. Categorically this would just exacerbate the problem as it was a short term remedy that not a sustainable solution. Hence the controversies in perceptions, definition and recognition of domestic violence vary from region to region and contribute to reporting level of rates of domestic violence which in turn affects the prevalence estimates of the burden of domestic violence. However violence is perceived as a means of solving differences and is highly appreciated as a tool of socializing children [27]. The Uruguayan survey found that 40% of households had a record of previous violence and 80% of households had a record of present violence.
Sexual violence against the above 50 years populations
Studies on sexual violence have unearthed that sexual violence can occur at any age in ones life [28,29]. They add that victims of reported rape at childhood stand chances of suffering sexual violence even in adulthood thus confirming that the old are prey to sexual and physical violence unlike the common school of thought that exonerated them from sexual abuse [30-32]. However many cases of sexual violence are not reported to authorities for fear of stigma and fear for further violence from the perpetrator hence prevalence rates of sexual violence are significantly affected by under reporting. About 10.4% (11.7 million) men in the United States revealed to have had a partner who insisted on getting pregnant without their consent and 8.7% reported to have had an intimate partner who insisted to get pregnant though they never wanted while 3.8% reported to have had an a romantic partner who declined to use a condom.
Cultural and gender dynamics in defining violence
These significantly determine the constructs in which people perceive and define abuse. Cultural and gender dynamics vary from society to society and determine what entails abuse that determines the reporting rates for domestic violence in a given society as it justifies it or condemns it [24].A study in Macedonia found that women declined to allow researchers to code slapping as physical violence because they felt that this was something casual and normal as it was frequently happening in many household [33].Contradictions in defining domestic violence were found in a study in Macedonia where men classified physical violence as only when aggression is associated with injury while women reported physical violence even when physical violence was not associated with injury [34].
Level of domestic violence among the above 50 years
It was found that in Australia 25% of women in 1996 experienced domestic violence [11]. However even in the developed world like Australia old people live in a world where domestic violence is not talked about and have to follow the footprints of their mothers who yielded into abuse. This is because society and norms are designed to think that the above 50 years do not experience abusive acts from their intimate partners. Hence Australian olden women have hardly been exposed and brought to the limelight of the influence of women empowering movement than the young women. Research on domestic violence among the above 50 years has been low because realities of the old people are lost when age is seen as the only factor exacerbating the abuse [35]. Hence the plight of the old is abused and their voices are hardly hard at the interface of domestic violence. Unlike the common school of thought that domestic violence is manifested among young, the above 50 years are also vulnerable to the problem, a survey conducted among the above 50 years in Argentina found that 51% of the above 50 years had been subjected to emotional violence and 11% mainly women had been subjected to physical violence on part of family members and no significant difference was established between economic level [36].
Effect of intimate partner violence on domestic violence
IPV hampers intimate partner communication and decision on safe sex practices for instance use of condom, HIV status disclosure and sexual faithfulness. Kalichman et al. established that women with abusive partners were more likely to decline negotiating condom use thinking that her persistence may be viewed as manifesting unfaithfulness or untrustworthiness of either partner. Further studies have shown that a womans fear and anticipation of potential violence from the perpetrator in suggesting condom use hampers negotiation for safe sex practices and is a critical component that exacerbates HIV transmission [37,38]. Subsequently the fear of violence determines whether a woman takes voluntary counseling and testing services.
Methodology
Methodology of the study, the study design, study population, sample size calculation, data collection tools and techniques, plan for data analysis and ethical considerations among others. The methodology is derived from the problem statement and study objectives.
Study Design
The study took a descriptive cross sectional survey. It employed both qualitative and quantitative data. The design was adopted to capture an in depth understanding of the burden of domestic violence among the 50 years and above old PLWH attending CoU hospital Mukono. The study used focus group discussions to capture an in depth narrative about the study variables and different focus group discussions for male and female respondents were organized. The use of two different data collection methods enhanced data triangulation and validity.
Sources of Data
The study used both primary and secondary data. Primary data was collected from the 50 years and above old PLWH attending CoU Mukono and from CoU Mukono hospital, selected key informants, while secondary data was captured from CoU Mukono hospital records like patient registers which reflected participant serial numbers, date of birth, place of residence and language of communication among other variables. Both primary and secondary data was used to aid data triangulation to ensure validity.
Study population
The study population constituted 196 adults 50 years and above old PLWH attending CoU hospital Mukono. Also 6 selected key informants were selected from CoU hospital Mukono. The 50 years and above old PLWH were captured from CoU Mukono data base following the inclusion and exclusion criteria. Study participants were on ART and proficient at either Luganda or English.
Inclusion criteria
Selected participants had to be 50 years and above of age
Selected participants had to be able to speak Luganda or English fluently.
- Exclusion criteria
Participants who did not speak English or Luganda fluently
Participants who were suspects of HIV/AIDS for instance on PEP. This information could be obtained from the data set as it included patients on ART and patients on post exposure prophylaxis.
The study targeted all the 6 key informants attending to the 50 years and above PLWH, Sample size calculation: Using the sample size calculation formula. However the study studied a sample of 196 respondents as 67 questionnaires had errors and never conformed to study standards and required procedures during data processing and editing for instance some questionnaires never conformed to prescribed age cut offs.
Sample Selection
Register sheets containing all the 50 years and above PLWH attending CoU Mukono hospital were used to generate the sampling frame in that the data base was controlled for the 50 years and above PLWH that random numbers were assigned to study units. A study sample of 263 was generated using simple random numbers that had been assigned to study units following the inclusion and exclusion criteria. Simple random sampling was used to generate the study sample of 263 respondents. This is being probabilistic minimizes study bias. However 196 respondents were studied as 67 questionnaires had errors. The method was also used because it increases generalizability among the target population. All the 6 key informants were selected for the focus group discussions and 30 respondents were selected for the focus group discussion through quota sampling. Two focus group discussions of females and males with each constituting of 15 participants were held to aid comparison of responses.
Study Variables
Dependent Variable
Level of domestic violence was the outcome variable that a scale running from 0-20 was used to determine if a participant lived in a violent relationship or a violent free relationship.
Independent Variable
Independent variables included the individual/background factors for instance gender, age, education, marital status, religion and HIV/AIDS. Socio-economic factors which included income and occupation among others and substance abuse like alcohol consumption. Covariates associated with domestic violence among above 50 years PLWH were used to predict the dependent variable and were coded as 1. The study is holding level of domestic violence as a dependent variable and holds covariates predicting domestic violence as independent variables among the above 50 years PLWH.
Domestic violence Screening Tool (HITS Instrument)
Clinical Research and Methods
The domestic violence scale tool in Table 1, was used to measure domestic violence which was the outcome variable. Each item was scored from 1-5, thus, scores for this inventory range from 4-20. A score greater than 10 was considered positive and indicates that a participant has suffered domestic violence while a score less than 10 was negative and indicated that a participant had not suffered domestic violence. Domestic violence was measured as a binary outcome and a binary logistic regression was used to test for significant predictors at both bivariate and multivariable levels.
Table 1: Domestic violence Screening (Measuring) Tool.
Data collection techniques
Questionnaires
The study used questionnaires which captured the objectives of the study that were interviewer administered for purposes of quality Control and compliance to the WHO ethical guidelines with selected respondents [39]. Questionnaires were translated to Luganda language in which they were administered and then translated to English during data entry to maintain content validity. Questionnaires were administered by trained field researchers in domestic violence.
Focus Group discussions were held with selected key informants and respondents to capture qualitative data about the study variables. Female interviewers held focus group discussions with a group of 15 female participants and male interviewers held a focus group discussion with a group of 15 male participants. These groups where separated to aid comparison in the collected data between the groups.
Plan for Data analysis
Data was collected, edited, coded, sorted and analyzed using the STATA software and it was tabulated and presented in tables. A Pearson chi-square statistic was used at bivariate level to analyze the association between a given predictor variable and domestic violence and given the association it was analyzed at bivariate and at multivariate level using the binary logistic regression. A fitted logistic regression was used to analyze and identify predictors that statistically significantly explain domestic violence among the above 50 years PLWH attending CoU Mukono. At a bivariate level, the Chi square statistic was used to obtain significance levels of predictor variables which were tested using the logistic regression. Significance was determined using the probability value cut off of 0.05 and variables with a probability value of less than 0.05 were determined significant at bivariate and multivariable level. Chi square analysis relied on the following equation.
Where; j=1,2,…, = k
I=1,2,…= r
Oij is the observed frequency
Eij is the expected frequency
k is the number of categories of the dependent variable
r is the number of categories of the independent variable
At a multivariate level the logistic regression was fitted using all variables through a backward elimination method using the following method
Where;
Pi is the probability of occurrence of the dependent variable domestic violence
1-pi is the probability that the dependent variable will not occur (pi + 1-pi =1)
Xs are the independent variables used to predict the dependent variable
bo is the intercept of the slope and is a constant
bj are the regression parameter estimates
A fitted Binary logistic regression was used to test the significance of variables at the multivariate level using ORS and the probability values. Significant variables were identified which were deemed to significantly explain domestic violence among the above 50 years PLWH attending CoU hospital Mukono. Qualitative data was analyzed through thematic analyses of themes from focus group discussions from key informants and selected participants and qualitative data was presented in themes.
Quality Control Issues
Field researchers were trained in researching violence among the above 50 years PLWH and results of a pilot study were analyzed and compared with study results. Questionnaires where transcribed to Luganda in which they were administered and then transcribed to English during data entry to maintain content validity. Questionnaires were administered by trained field researchers in domestic violence.
Plan for dissemination of data
Findings were compiled into a report and presented to the Institute of Health Policy and Management at International Health Sciences University Kampala. A copy of the dissertation will be submitted to the Belgian Technical Cooperation Kampala and Raising Voices.
Ethical issues
Female researchers interviewed female respondents and similarly male field researchers interviewed male respondents. This was adopted to maximize privacy and confidentiality. It is one of the guidelines in conducting research on domestic violence.
Respect of autonomy: participation in the study was voluntary that only respondents who gave an informed consent were interviewed. Respondents had a right to consent to the study or to opt out of it without any threats or intimidation.
Principle of Beneficence: the study maximized benefits and minimized risks to study participants and a thorough explanation about the benefits and risks of the study to participants was read and explained to respondents for them to choose whether or not to participate in the study. They were explained the purpose, objective and goal of the study and how it benefits them. Participants were assured of confidentiality and privacy that all data would be used for only study purposes and no names of participants would appear in the final report.
Principle of Harm: The harm principle was observed where all respondents were assured of confidentiality and privacy of all their responses that all the information would be stored and kept safely to avoid external viewing so that it is only used for study purposes. During presentation of results no information will show its source or particular respondents who gave specific pieces of information as this can provoke more episodes of violence from the perpetrator. Participants where offered mobile numbers of counselors who would counsel them in case of emotional discomfort caused by some of the questions.
Respect of persons: Respondents had a right to autonomy that participants with diminished or impaired autonomy where excluded from the study as the study never employed joint confidentiality for privacy. Selected participants had a right to halt the interview at any time in case of any interruption and interviews were scheduled at the respondents convenience. Respondents fixed appointments for interviews and determined interview spots.
Principles of justice
The study targeted the above 50 years PLWH as it is aimed at curbing domestic violence issues that affect their treatment regimens. Hence the burden of research was only felt by the above 50 PLWH and on ART that it never targeted suspects of HIV or people below 50 years as benefits of the study would not accrue to them.
Limitations of the study
The study used a sample of the 50 years and above PLWH from Mukono which cannot be generalized to other 50 years and above PLWH in other areas. The study lacks statistical power to be generalized to external areas and hence findings exclusively define domestic violence among the 50 years and above PLWH though they give a snap shot of the problem and can be based on to conduct an extensive study. This is descriptive cross sectional study hence it suffers weaknesses of a cross sectional study for that it cannot test for causation. Data on both independent and dependent variables was collected at the same point in time hence it can hardly test causation as it mainly depends on previous data to explain the dependent variable which is subject to memory and recall bias. However to minimize memory and error biases the very 50 years and above for instance above 95 years were eliminated from the study and data on possible confounders was collected.
Results of the Study
Introduction
Study findings which are tabulated in percentages, frequencies to show the level of domestic violence and presented in χ2 and Odds ratios to test for associations between study variables and domestic violence the outcome variable and to identify significant variables at both bivariate and at multivariable level.
Socio Demographic Characteristics of Respondents
Table 2 presents demographic characteristics of the studied respondents who attend CoU Mukono hospital which are presented in percentages scores. A descriptive analysis of demographic variables is tabulated to aid interpretation of the study sample and to aid analysis of results in relation to study objectives (Table 2).
To view Table 2 click below
Table 2: Socio Demographics of respondents.
Of the 196 respondents studied 76.53% (150) were between 50-79 years and 23.43% (46) were above 79 years. According to Table 3, age showed a χ2= 9.55, P = 0.002 which is a significant association. This means that age was associated with domestic violence hence interventions to curb domestic violence so as to improve treatment regimens of the 50 years and above PLWH should meet the domestic violence related issues of different age groups. Percentage scores reported on religious affiliation indicated that 17.86% (35) were Protestants, 25% (49) Catholics, 20.92% (41) Muslims, 19.39% (38) Pentecostal and 16.84% (33) from other religions hence Catholics were the majority and those from other religious denominations were the least in the study sample. Hence according to the table 3 below, religion was not associated with domestic violence with a χ2= 8.8678, P =0.064 thus interventions to curb domestic violence among the 50 years and above PLWH should not target religion as religion is not associated with domestic violence. The study findings established that 25.51% (50) had no formal education, 25 % (49) had primary education, 17.86 % (35) had secondary education, 13.78% (27) had university education and 17.86% (35) had tertiary education which implies that 50.51% had utmost primary education. According to table 3 below, education is not associated with domestic violence as a χ2= 2.03, P=0.729 was obtained thus interventions to curb domestic violence in order to improve treatment regimens among the 50 years and above PLWH should not target education levels as education level is not associated with domestic violence. Of the 196 respondents studied 22.96% (45) were married compared to the 77.04% (151) who were unmarried though with regular sexual partners which gave a χ2 =28.66, P = 0.000 which is a significant association as seen in table 3 below. Hence marital status is associated with domestic violence and therefore interventions to curb domestic violence in order to improve the treatment regimens of the 50 years and above PLWH should target domestic violence issues of different marital statuses of patients. Of the 196 respondents studied females constituted 37.24% compared to the males who constituted 62.75% which according to Table 3 below, gave χ2= 2.16, P = 0.14 which shows that domestic violence is not associated with gender. Hence interventions to curb domestic violence should not target gender as gender difference is not associated with domestic violence but should focus at associated factors with domestic violence for instance marital status of patients. Among the 196 respondents studied 21.94% were involved in professional works including teaching, medical work and other professional works, 13.27% were taxi drivers working directly as taxi drivers or owning taxis, 9.69% worked as motor riders or owned motor bikes, 11.73% worked in bakery business, 10.20% owned saloons or were employed in saloons as hair dressers while others worked as barbers, 13.27% worked as shoe repairers and 19.90% were employed in other occupations. According to table 3 below, this gave χ2=3.15, P=0.789 which is not a significant association implying that there is no association between domestic violence and occupation. Therefore interventions to curb domestic violence in order to improve the treatment regimens of the 50 years and above PLWH should not target occupations as domestic violence is not associated with occupation but should focus at associated factors with domestic violence as seen in Table 3.
Domestic violence and significant conceptualized predictors
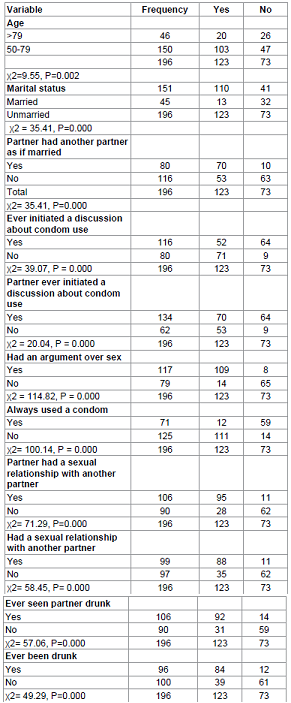
Table 3 presents χ2 results of significant factors associated with domestic violence and are interpreted using a 95% CI, P=0.05. Interpretation of results is related to study objectives and policy implications are given to contribute to policy formulations in order to curb domestic violence and identify areas of further research (Table 3).
To view Table 3 click below
Domestic violence across age: According to the Table 3, age is significantly associated with domestic violence with a χ2 = 9.55, P= 0.002. Hence interventions to curb domestic violence should meet the domestic violence issues of different age groups in order to improve the treatment regimens of the above 50 years PLWH as age is associated with domestic violence.
Domestic violence across marital status: According to Table 3 above, domestic violence is associated with marital status with a χ2= 28.66, P = 0.000. Hence interventions to curb domestic violence in order to improve the treatment regimens of the above 50 years PLWH should meet the domestic violence issues related to marital status of patients.
Domestic Violence across partners who had partners who lived with other partners as if married: According to the Table 3, domestic violence is associated with a partner having other partners as if married with a χ2= 35.41, P = 0.000. Hence interventions to curb domestic violence in order to improve the treatment regimens of the above 50 years PLWH should discourage patients from having other partners as if married as having another partner as if married is a risk factor to domestic violence
Domestic across ever initiated a discussion about condom: According to Table 3, domestic violence is statistically associated with having discussions about condom use with a χ2= 39.07, P = 0.000. Hence interventions to curb domestic violence so as to improve the treatment regimens of the above 50 years PLWH should integrate mechanisms that hamper violence accruing due to discussion about condom use among patients.
Domestic Violence across partner ever initiated a discussion about condom use: According to Table 3, domestic violence is associated with a partner having ever initiated a discussion about condom use with a χ2 = 20.04, P = 0.000. Hence interventions to curb domestic violence in order to improve the treatment regimens of the above 50 years PLWH should integrate issues of promotion of violent of discussions about condom use to promote positive discussions about condom use to avoid violence.
Domestic Violence across ever had an argument over sex in the last 12 months: According to Table 3, domestic violence is associated with having an argument over sex with a χ2 = 114.82, P = 0.000. Hence interventions to curb domestic violence in order to improve the treatment regimens of the above 50 years PLWH should address issues of containing arguments over sex as having arguments over sex is a risk factor to domestic violence.
Domestic violence across always used a condom in the last 12 month with regular partner: According to Table 3, domestic violence is associated with frequent condom use with a χ2= 100.14, P = 0.000. Hence efforts to curb domestic violence in order to improve the treatment regimens of the 50 years and above PLWH should integrate issues of designing safe mechanisms for negotiation of condom use among patients.
Domestic violence across partner having had a sexual relationship with another partner: According to Table 3, domestic violence is associated with a partner having had sexual relationships with another partner in the last 12 months before the study with a χ2= 71.29, P=0.000. Hence interventions to curb domestic violence in order to improve the treatment regimens of the above 50 years PLWH should integrate issues of containing partners from having sexual relationships with other partners in their design.
Domestic violence across having had a sexual relationship with another partner in the last 12 months: According to Table 3, domestic violence is associated with having had a sexual relationship with another partner in the last 12 months before the study with a χ2= 58.4532, P= 0.000 which is a significant association. Thus efforts to curb domestic violence in order to improve the treatment regimens of the above 50 years PLWH should discourage patients from having sexual relationships with other partners.
Domestic violence across ever seen partner drunk in the last 12 months: According to the Table 3, domestic violence is associated with having ever seen a partner drunk with a χ2= 57.0659, P=0.000 which is a significant association. Hence interventions to curb domestic violence in order to improve the treatment regimens of the above 50 years PLWH should integrate issues of containing alcohol consumption among patients.
Domestic violence across respondents who had ever been drunk: According to Table 3, domestic violence is associated with a respondent ever have been drunk with a χ2= 49.29, P=0.000 which is a significant association. Hence efforts to curb domestic violence in order to improve the treatment regimens of the above 50 years PLWH should integrate issues of containing alcohol consumption as alcohol consumption is associated with domestic violence.
Domestic violence across respondents who had been often drunk: According to the Table 3, domestic violence is associated with a patient being often drunk with a χ2= 39.80, P=0.000 which is a significant association. Hence interventions to curb domestic violence in order to improve the treatment regimens of the above 50 years PLWH should integrate issues of retraining alcoholism in design and programming as alcoholism is associated with domestic violence.
Domestic violence across respondents who saw their partners often drunk in the last 12 months: According to the Table 3, domestic violence is associated with a respondent having seen his partner drunk with χ2= 38.6313, P=0.000. Hence interventions to curb domestic violence in order to improve the treatment regimens of the above 50 years PLWH should focus at encouraging patients to refrain from being often drunk as a patients seeing his partner often drunk is significantly associated with domestic violence.
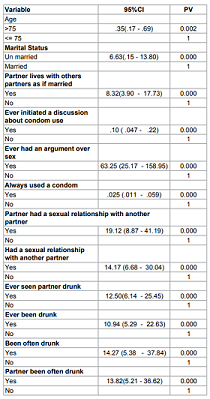
Presentation of results of the bivariate logistic regression: The table 4 presents results of the binary logistic regression and presents variables that are associated with domestic violence at bivariate level which are computed at a 95% CI, P=0.05. Interpretation of results is related to study objectives and policy implications are given to contribute to policy formulations in order to curb domestic violence so as to improve the treatment regimens of the above 50 years PLWH and identify areas of further research (Table 4).
To view Table 4 click below
Table 4: Binary logistic Regression.
Age
According
to Table 4, domestic violence is significantly associated with age with OR=.35, 95% CI=.17 - .69, P= 0.002. Hence respondents
above 79 years have 0.65 odds less of living in violent relationships as
compared to their counterparts below 79 years. This is in line with table 3
results that established a significant association between domestic violence
and age. Thus interventions to curb domestic violence should be mainly geared
towards patients less than 79 years as they are 65% times more likely to live
in violent relationships as compared to those above 79 years.
Marital
status
According
to Table 4, there is a significant relationship between domestic violence and
marital status with OR= 6.60, 95 CI= 3.15 - 13.80, P= 0.000. Respondents who
were unmarried had 7 odds more of living in violent relationships as compared
to odds of respondents who were married. This means that interventions to
combat domestic violence should be mainly targeted at unmarried patients so as
to curb domestic violence in order to improve the treatment regimens of the
above 50 years PLWH.
Partner lives with other partners as if married
According
to Table 4, domestic violence is significantly associated with living with
another partner as if married with OR= 8.32, 95% C.I = 3.90 -17.732, P=
0.000.This implies that respondents who lived with other partners as if married
had 8 odds more of living in violent relationships as compared to odds of
respondents who never lived with other partners as if married. Hence odds of
domestic violence increase with sexual unfaithfulness thus interventions to
curb domestic violence should promote sexual faithfulness in order to improve
the treatment regimens of the above 50 years PLWH.
Ever initiated a discussion about condom use
According to Table 4, domestic violence is significantly associated with initiation of condom use with OR =.102, 95% C.I= .0470 - .2256, P= 0.000. Hence respondents who ever initiated a discussion about condom use had 0.898 odds less of living in violent relationships as compared to odds of respondents who never initiated a discussion about condom use. Thus interventions to curb domestic violence should be mainly geared towards patients less than 79 years as they are 65% times more likely to live in violent relationships as compared to those above 79 years. However the above 79 years old lived in less violent relationships as compared to the age group less than 79 years old as it was hard for them to start new relationships. Marital status of respondents: According to Table 4 there is a significant relationship between domestic violence and marital status with OR= 6.60 95 CI= 3.15 - 13.80 P= 0.000. Respondents who were unmarried had 7 odds more of living in violent relationships as compared to odds of respondents who were married. This is in agreement with Koening who established that the married lived in less violent relationships as compared to the unmarried. Therefore interventions to combat domestic violence should be mainly targeted at unmarried patients and should clearly address domestic violence issues affecting the unmarried in order to improve the treatment regimens of the above 50 years However the married lived in less violent relationships because of the respect they had for each other as compared to the unmarried who thought they could always get a new partner. Partner lives with other partners as if married: According to Table 4 domestic violence is associated with partners living with other partners as if married with OR= 8.320 95% C.I = 3.904 -17.732 P= 0.000. Hence respondents who lived with other partners as if married had 8.3 odds more of living in violent relationships as compared to odds of respondents who never lived with other partners as if married. This is in line with AI that established a strong correlation between domestic violence and sexual unfaithfulness. Ever initiated a discussion about condom use: According to Table 4 domestic violence is associated with having a discussion about condom use with OR =.102 95% C.I= .047 - .225 P= 0.000. This implies that respondents who ever initiated a discussion about condom use had 0.9 odds less of living in violent relationships as compared to odds of respondents who never initiated such a discussion. This is in line with Kalichman et al and hence interventions and programmes aimed at combating domestic violence should involve mechanisms that promote condom use among patients in order to curb domestic violence so as to improve the treatment regimens of the above 5
Keywords
HIV/AIDS, Domestic Violence, Alcohol

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}