Introduction
Dental caries is an ancient
disease that dates back to the time when agriculture replaced the hunt as the
main source of food, although its prevalence and severity were at much lower
levels at that time compared to prevalence of dental caries today. Previous
studies showed the decline of dental caries by using fluoride in the developed
countries. On the hand, the lack of public awareness and motivation, inadequate
resources for sophisticated dental treatments and changing eating habits causes
higher significantly caries prevalence in undeveloped and developing countries
[1]. Indeed, the use of fluoride has been recognized as one of the most
successful measures to
prevent dental caries
in the history of public health. Indeed, the use
of fluoride has been recognized as one of the most successful measures to
prevent dental caries in the history of public health.
But
"fluoride is often referred to as a double blade weapon" - the
optimal and reasonable use of fluorine offers maximum protection against
cavities, while unwanted and excessive systemic exposure can lead to chronic
fluoride intoxication, which is manifested as dental and skeletal fluorosis [2]. In view of
this, a more precise definition of the optimum concentration of fluorine in
drinking water (which is not a universal constant and varies depending on
environmental conditions) becomes even more important. Clinical trials of the
effects of fluoride on humans could not be feasible due to ethical and many
other practical obstacles. Endemic areas, where people are naturally exposed to
increased amounts of fluoride, serve as natural laboratories to study the
effect of fluoride
concentration on dental caries and dental fluorosisat the same time [3].
In
the past in the Republic of Macedonia, there were three endemic fluorotic regions
(Kumanovo, Veles and Prilep region). Tsarchev et al., in 1992 [4] conducted a
study in which the dependence of fluoride in drinking water and caries
frequency in endemic areas were investigated. This has prompted us to undertake
this study in order to determine the prevalence of dental caries in
12-year-olds from the Vardar region.
Material and
Methods
The
clinical trial consisted of defining the DMFT of the 12-year old children in accordance
with the basic criteria for assessment of oral and dental health and the need
for rehabilitation, which is recommended by the World Health Organization (WHO,
ORAL HEALTH ASSESSMENT FORM, 1997). We estimate the intensity of dental caries
according to the generally accepted Klein-Palmer index "DMF", which
is a set of decayed, missing and filled teeth. The examinations were carried
out by two dentists in accordance with the recommendations stemming from the
basic criteria for assessment of oral and dental health recommended by the WHO
[5].
The
12-year-old children who were included in the examination were from the
following elementary schools in the eastern region: ОU Dame Gruev from city
Gradsko, regional primary school Dame Gruev from village Vinicani, regional
primary school Todor Janev from village Melnica and central primary school OU
Jordan Konstantinov Dzinot from city Veles.
For
the determination of the fluorine concentrations by laboratory examination, we
used samples of water from all urban and rural settlements, where the children
from the Vardar region of the Republic of Macedonia live.
In
our study, an electrochemical procedure was used to determine the concentration
of fluoride with an ion-selective electrode. A major part of the ion-selective
electrode is the lanthanum
membrane fluoride.
When the membrane is in contact with the solution containing fluoride (in this
case water), the difference in potential is measured. This potential depends on
the amount of free fluoride ions and is described by the Nernst formula
Е=Ео-СlogА
E-measured
potential of the electrode
E-reference
potential (constant)
A-quantity
of fluoride in the solution
C-slope
of the electrode
The
samples were collected in 100 ml polyethylene containers with a cap that had
threads. The measurement was carried out as soon as the water samples arrived
in the laboratory. After shaking the water bottle, 1 ml of each sample is taken
and mixed with 0.1 ml Total Strength Adjusting Buffer. The fluorine
concentration of all samples was determined using the ionic-selective electrode
(Thermo Orion Ion Plus Fluoride Electrode) and the ionometer (pH / ISE
meter-Thermo-Orion) at the Public Health Institute. For chemical
analysis 10% of TISAB Aluminon was used. Fluoride standards with a
concentration of 0.01 to 1.00 mg / l were used to calibrate the measurements. Before
the starting of the fluorine measurement, some preparations must be made to
check the correctness of the measuring instrument and the slope of the
electrode. This is done according to the manufacturers instructions. When the
instrument is ready, the measurement can begin.
Results
The
group of 12-year-old respondents from the Vardar Region consists of 85
children, of which 52.94%are male and 47.06% are female. In the ethnic
structure, the Macedonians dominate, with 65 (76.47 %) respondents, followed by
the Turks, represented by 11 (12.94%) respondents.
More
than half of the respondents from this group are from the city, 37.65% of the
children live in Veles, 21.2% in the municipality of Gradsko, while the
children from villages Melnica and Vinicani make up the group of 41.2% children
at the age of 12, originating from a rural area (Table 1).

Table
1:
Distribution of the children in relation to the gender, nationality and the
place of living.
Figure 1 and Figure 2 show the distribution of the presence of decayed, extracted and
filled permanent teeth in the group of
12 year old children from the Vardar region. Thirty five of them do not have
cavities 35 (41.2%), while from the group of 50 (58.8%) children with cavities,
the greatest number of children were with two decayed teeth - 16 (18.8%) registered.
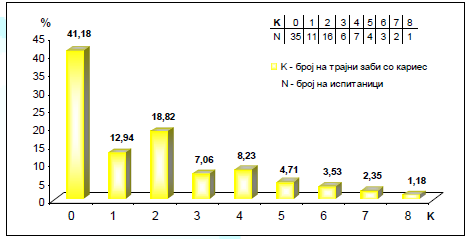
Figure 1: Distribution of
the children in relation to the number of the decayed permanent teeth.
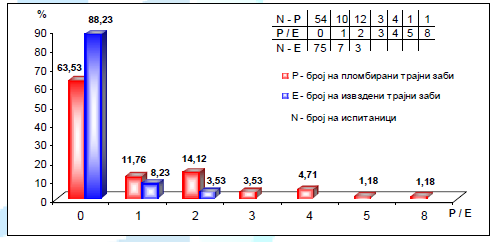
Figure 2: Distribution of
the children in relation to the number of filled and missing permanent teeth.
In
10 (11.8%) children from this group, teeth extractions were performed, and in 7
children, one tooth was removed, and in 3 children two teeth were extracted.
Without filled teeth were 54 (63.5%) children, while in the group with filled
teeth the highest number of children were with two filled teeth -12 (14.1%).
The
descriptive statistics on the number of decayed, extracted and filled teeth was
presented in Table 2. The number of
decayed and filled permanent teeth ranges between 1 and 8, the number of
missing teeth ranges from 1 to 2, while half of the 12-year-old children from
the Vardar region have dental caries on more than 2 teeth, have extraction on
more than one tooth, and have fillings on more than 2 teeth.
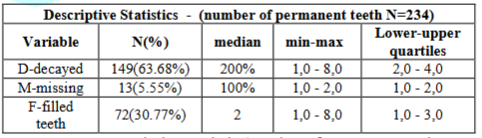
Table 2: Descriptive
statistic /number of permanent teeth.
The
value of the DMFT index of permanent teeth in the group of 12-year-old children
from the Vardar region is shown in table number 3 and ranges from 0 to 13, and
on average it is 2.75 ± 2.56 (Table 3).
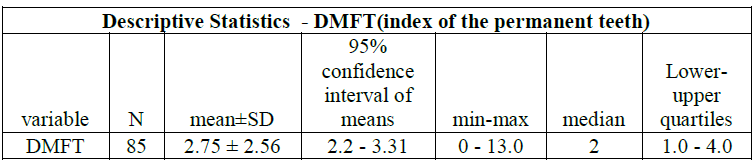
Table 3: Descriptive statistic/DMFT
index of the permanent teeth.
Female
children at the aged of 12 years from the Vardar region significantly more
often than male children have dental caries on permanent teeth (p = 0.049),
they have more frequently extracted teeth (p = 0.38), but not significantly and
have more fillings on teeth (p = 0.52), but also not significantly (Table 4).

Table 4: Distribution of
decayed, missing and filling permanent teeth in relation to gender.
The
average value of the DMFT index of permanent teeth in the group of male
children was 2.27 ± 2.43, while in the group of female children the average
value of DMFT was 3.3 ± 2.62. The gender of 12 year old children from the
Vardar region has significant impact on the value of the DMFT index of
permanent teeth (p=0.039) as a result of significantly higher DMFT values in
the female respondents group (Table 5).
Table 6 shows the values of the fluoride concentration in drinking
water from
all places were the children live.
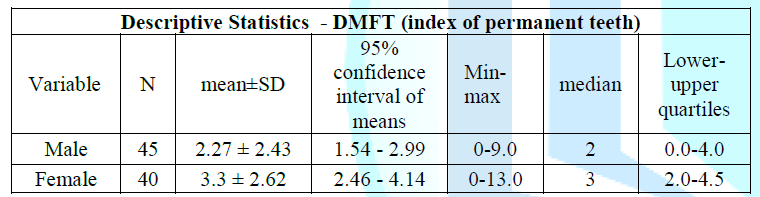
Table 5: Descriptive
statistics of the DMFT index of the permanent teeth/differences in gender.
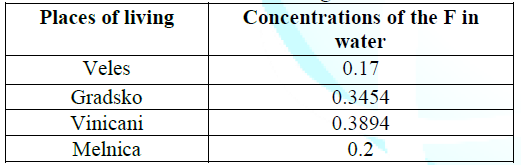
Table 6: Distribution of the concentration of fluorine in
water in relation to the place of living.
Figure 3 shows the
correlation between the value of the DMFT index of permanent teeth within 12-year-old
children and the concentration of fluorine in drinking water from the Vardar
region. The value of Spearmans coefficient of rank correlation of R = - 0.393
shows that there is a negative or indirect correlation between these two
variables. Which means, by increasing the concentration of fluorine in water,
the value of the DMFT index of permanent teeth decreases, and vice versa. For a
value of p <0.01, and statically this connection is confirmed as highly
significant, i.e. highly significant.
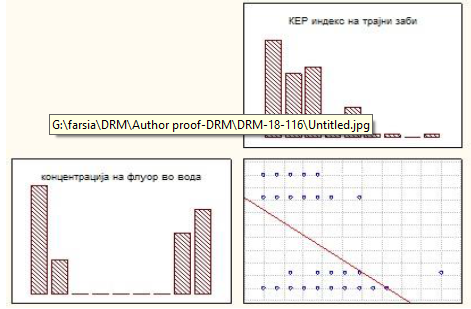
Figure 3: Correlation-DMFT
index of the permanent teeth /concentration of the fluorine in the water
Table 7 shows the
results of the Linear regression analysis for quantifying the significant
relationship between the value of the DMFT index of permanent teeth for a group
of 12 year old children as the dependent variable and the concentration of
fluorine in the water in the Vardar region. The R Square value of 0.188 implies
that 18.8% of the changes in the DMFT index can be explained by the
concentration of fluorine. The coefficient β, whose value is -11.176, shows
that with each increase in unit of the fluorine concentration, the value of
the DMDT index decreases by an average of 11.176 (16.255-6.098).

Table 7: Linear Regression
Analysis - DMFT/concentration of fluorine.
Discussion
The
Correlation between DMFT score of the permanent teeth of 12-years old
children from the Vardar region and the concentration of fluoride in drinking
water was negative, with the value of the Spearman-Conns rank correlation
coefficient of R = - 0.393, which showed that between these two variables, the
correlation was negative or indirect. For the value of p<0.01, this
relationship was confirmed as a highly statistically significant or highly
significant.
Markovic
N, et al., in their cross-sectional study conducted in 2004 on the territory of
Bosnia and Herzegovina within the group of 1,120 children at the age of 6 and
12, found the mean dmft/DMFT index of 4.16 ± 2.92 in 12 years old, and 6.71 ±
3.89 in 6 year old children. Non-restored decayed teeth constituted the bulk of
the DMFT index, 45.43% for 12-year-old and 88.79% for 6-year-old children [6].
Hysi D et al. in their study examined the average DMFT index in a group of 372,
12 year old children from Tirana and found that it was 3.8. The significant
caries index in the same group of children was 7.06, while the prevalence of
children without caries was 14.5% [7]. In the course of 2006, Djuričković M et
al conducted a survey of 455 pupils at the age of 12 in the northern, middle
and southern regions of Montenegro. The average DMFT index of 12-year-old from
Montenegro was 3.43, the SiC index was 6.35, while the prevalence of caries was
88.35% [8]. The results of another study in Montenegro show an increase in
caries prevalence with age. Thus, 91% of 12-year-olds have one or more carious
lesions, with a maximum value of 97% for 15 years old and 98% for children at
the age of 18, respectively, the average DMFT index for 12 years is 4.4, year,
8.25 and 18-year-olds, 10.9 [9].
In
the past in the Republic of Macedonia there were three endemic fluorotic
regions (Kumanovo, Veles and Prilep region). Tsarchev et al. in 1992 [4]
conducted a study in which the dependence of fluoride in drinking water and
caries frequency in endemic areas and other control settlements. In the
Kumanovo endemic region (from Tromedje, from AjudckaCheshma, from Puckovo and
from BeleiGramadi), the mean mgF / L in the drinking water from the wells was
2.75, and from the taps 1.48, while in the control settlement (Staro Nagorichane)
was 0.20 mg F / L. In the endemic area, the average DMFT index ranged from 0.79
to 1.92, while in the control settlement it was 5.92. In the Veles endemic
region (v. Vinicani) the mean mgF / L in the drinking water of all objects were
1.24, and in local wells 0.58, while in the control settlement (village
Gradsko) was 0.58 mgF/L.
In
the endemic area, the average DMFT index was 2.30, and in the control
settlement 6.24. In the Prilep Endemisk Region (Novovo Lagoovo village), the
mean mg mg/l in drinking water in October 1985 was 1.93, and in June 1986 1.60,
while in the control settlement (village Berezovci) was 0.20 mgF/L. In this
endemic region, the average DMFT index was 2.10, while in the control
settlement 3.83 [4].
The
studies of numerous authors have found that fluoride concentration in drinking
water of 0.8-1.5 mg / L can lead to a reduction in dental caries by more than
60% [5,10,11]. Drinking water in the Republic of Macedonia, and especially
those consumed in larger cities, contain fluoride concentrations, usually less
than 0.2 mg / L [12-14].
In
her research, Kolevska et al has found the highest fluorine values in the
groundwater in Pelagonia, Ovche Pole,Vardar and in some spring waters of
Belasica and Osogovo. She noted that in most of these cases, there are many
small sources intended for water supply of settlements that are in decline of
population and with an unfavorable age structure, withthereduced number of
childrens population. These are the villages in the municipalities of Veles,
Negotino, Prilep, Bitola, Kratovo, KrivaPalanka, Sveti Nikole, Stip and
Probistip. Municipalities in which the villages show demographic expansion with
a large number of children are predominantly located on sites with water
sources containing mostly small fluorine quantities. The waters are from the
springs of Shar Planina, Suva Gora, Bukovik, Korab-Deshat, SkopskaCrna Gora,
Jablanica. In the eastern part of our country and partly in the groundwater in
the Vardar Valley, Ovchepolyeto, along the riverBregalnica, there are some
higher values, which are close to the optimal fluorine concentration, but as a
rule, the mineralization is higher. Natural fluoride-containing sources are, as
a rule, of small or very low capacity. These sources are mainly found in
eastern Macedonia where there is a triangle with a geological composition of
erupted rocks and where a significant number of the investigated waters have a
concentration close to the optimal (the municipalities of Kumanovo, Kocani,
Stip, Radovish, Strumica and Sv.Nikole) [14].
Recent
research in Lithuania indicates lower values of the average DMFT index 2.0 in
12-year-old children from regions (1.7 ppm) with high level of fluorine in
drinking water, and higher values of an average DMFT of 3.5 in areas with low
fluoride levels ( 0.2 ppmF) [15].
Our
results show that spring waters have relatively low fluorine content. Greater
content is found in well water, while the surface water content is also low.
The waters that originate from deeper depths are richer with fluorine compared
to those of smaller depths. Water with less hardness also contains less
fluorine, while hard waters have higher fluorine content. The content of
fluoride in water depends on the geological composition of the land with which
the water comes in contact with its movement [16].
All
official data on dental caries, both nationally
in Macedonia (Department of Dental Health Protection within the
Ministry of Health) and internationally (World Health Organization, WHO),
register caries only when manifested as cavity, while (the initial carious
lesion is not registered [17]. In the complex interaction of predisposing
factors, the urban and rural environment significantly affect the prevalence of
caries.
The
school time is a period when habits are permanently created and when health
education measures are most beneficial. Children must be convinced that the
mouth and teeth mirror
health
and that there is no complete health in the absence of oral health. Wennhall I
et al. showed that adjusted preventive programs for children living in a
multicultural society with low socio-economic development are cost-effective
and of great benefit to society as well as great benefit for the individual
[18].
The
nutrition is part of the everyday life of every living creature, and even of
man, which affects not only the oral, but also the health as a whole. Dental
caries risk is directly related to the frequency and amount of carbohydrate
intake, especially in the time intervals between meals [19,20].
In
fact, it is well known for many years that the lack of regular oral hygiene
habits plays a significant role in the development of dental caries. Oral
health of children can be influenced by the attitudes and behavior of parents
towards oral health, as well as by their parent oral health [21-23].
On
the Macedonian market, toothpastes containing fluoride can be easily found, but
as a consequence of irregular hygiene and lack of teeth brushing, the benefits of
this measure for the prevention of dental caries are insufficient.
Fluoride
tablets are also available on our market, but despite being on the positive
list of drugs, they are not prescribed regularly enough in children with a high
caries risk profile and in caries-active children by dentists, gynecologists
and pediatricians. Fluoride gels and varnishes for professional use contain
high levels of fluorine, but due to the privatization process of dental practice, dental dentists do not pay
enough attention to this preventive measure, so its benefits are missing. They
need to apply to children with high caries risk, and this is a strictly
controlled process by pediatric dentists where the child
is being treated.
Good
health is an important resource for social, economic and personal development.
Political, economic, social, cultural, environmental, behavioral and biological
factors can improve or worsen health. Health promotion actions are directed
towards taking appropriate measures, making these conditions suitable for
health [24].
We
hope that this study will help the decision makers to improve oral health by studying the
unwanted causes that have led to oral health state in our country and will act
in a way to improve the situation and adequately prevent and treat dental
caries in the childrens population.
References
1.
Kulkarni
SS, Deshpande SD. Caries prevalence and treatment needs in 11-15 year old
children of Belgaum city (2002) J Indian Soc Pedo Prev Dent 20: 12-15.
2.
Devaranavadagi
BB, Satishkumar and Chandrakanth KH. Fluoride- A double edged sword (2007) Anal
Med 10: 2.
3.
Sharma
A, Gupta A and Gupta S. Dental caries prevalence in endemic fluoride areas of
Haryana State, India (1998) J Indian Dent Assoc 69: 97-99.
4.
Carcev
M, Gorgev D, Neceva Lj, Docevska V and Filjanski P. Fluorine in drinking water
and caries frequency in the endemic areas of Macedonia (1992) Mac Dent Rev 16: 51-57.
5.
WHO:
Fluorine & Fluorides. Environmental Health Criteria 36, World Health
Organization (1984) Geneva.
6.
Markovic
N and Muratbegovic AA. Oral health in Bosnia and Herzegovina Schoolchildren-Findings
of first national survey (2014) Austin J Dermatol 1: 4.
7.
Hysi
D, Droboniku E, Toti Ç, Xhemnica L and Petrela E. Dental caries experience and
oral health behavior among 12-year-olds in the city of Tirana, Albania (2010)
Oral Health and Dental Management in the Black Sea Countries 9: 229-234.
8.
Djuričković
M and Ivanoviæ M. Oral Health Conditions in Children Aged 12 Years in
Montenegro (2011) Vojnosanit Pregl 68: 550-555.
9.
Matijević
S. Connected to the health of the health of patients with pathogenesis in
Montenegro (2009) Acta Stomatologica Naissi 25: 59.
10.
Gorgev
D, Neceva Lj, Filjanski P, Kolevska L, Pashu M, et al. Some aspects of
nutritional and dental status among school children in endemic-fluorotic zones
in SR Macedonia (1989) Mac Med Rev 3: 83-85.
11.
Tavchiovski
I, Rafajlovski R, Stevanovic M, Kederov P, Stojanovski J, et al. Multiple
examination of the ratio between dental caries and fluoride concentration in
drinking water (1979) Mac Dent Rev 3: 209-214.
12.
Ambarkova
V, Topitsoglou V, Iljovska S, Jankulovska M and Pavlevska M. Fluorine Content
of Drinking Water in Relation to the Geological-Petrographical Formations From
FYROM (2007) Balk J Stom 11: 163-166.
13.
Ambarkova
V, Topitsoglou V, Iljovska S and Carcev M. Natural fluoridated drinking water
from the Republic of Macedonia (2005) Macedon Stomatol Review 29: 177-82.
14.
Koleva
L, Filjanski P, Cvetkoska T, Gorgev D and Mitrikeska M. The contents of
fluorine in the drinking water from SR Macedonia (1985) Mac Med Review 4:
103-106.
15.
Narbutaité
J, Vehkalahti MM and Milciuviené S. Dental fluorosis and dental caries among
12-year-old children from high- and low-fluoride areas in Lithuania (2007) Eur
J Oral Sci 115: 137-142. https://doi.org/10.1111/j.1600-0722.2007.00434.x
16.
Ambarkova
V, Topitsoglou V, Iljovska S, Sijakova-Ivanova T, Jankulovska M, et al. Relation
between the fluorine content of drinking water and geological formation
Relation between the fluorine content of drinking water and geological
formation (2008) Macedon Stomatol Review 232: 1-7.
17.
Carcev
M, Milosevski B, Spirovski V, Getova B, Sarakinova O, et al. Guidebook for
Implementation of the National Strategy for Prevention of Oral Diseases for
children of 0-14 year of the Republic of Macedonia (2010) Ministry of Health,
Department for Dental Health Care, Skopje.
18.
Wennhall
I, Norlund A, Matsson L and Twetman S. Cost- analysis of an oral health
outreach program for preschool children in a low socioeconomic multicultural
area in Sweden (2010) Swed Dent J 34: 1-7. https://doi.org/10.1111/j.1365-263X.2007.00903.x
19.
Johansson
I, Holgerson PL, Kressin NR, Nunn ME and Tanner AC. Snacking habits and caries
in young children (2010) Caries Res 44: 421-430. https://doi.org/10.1159/000318569
20.
Bruno-Ambrosius
K, Swanholm G and Twetman S. Eating habits, smoking and tooth brushing in
relation to dental caries: a 3-year study in Swedish female teenagers (2005)
Int J Paediatr Dent 15: 190-196.https://doi.org/10.1111/j.1365-263X.2005.00621.x
21.
Adair
PM, Pine CM, Burnside G, Nicoll AD, Gillett A, et al. Familial and cultural
perceptions and beliefs of oral hygiene and dietary practices among ethnically
and socio-economically diverse groups (2004) Community Dent Health 21: 102-111.
22.
Mattila
ML, Rautava P, Aromaa M, Ojanlatva A, Paunio P, et al. Behavioural and
demographic factors during early childhood and poor dental health at 10 years
of age (2005) Caries Res 39: 85-91. https://doi.org/10.1159/000083152
23.
Poutanen
R, Lahti S, Seppa L, Tolvanen M and Hausen H. Oral health related knowledge,
attitudes, behavior, and family characteristics among Finnish schoolchildren
with and without active initial caries lesions (2007) Acta Odontol Scand 65: 87-96.
https://doi.org/10.1080/00016350601058077
24.
World
Health Organization. The World Health Report (2002) Reducing risks, Promoting
Healthy Life, Geneva.
*Corresponding author:
Ambarkova Vesna, Department
for preventive and pediatric dentistry, Faculty of dentistry, University
Ss.Cyril & Methodius, Skopje, Republic of Macedonia, E-mail: ambveki@yahoo.com
Citation:
AmbarkovaV. The effect of water fluoride
concentration on DMFT index in vardar population in Macedonia (2018) Dental
Res Manag 2: 56-60


