
 PDF
PDF
Introduction
An improved super-elastic Ti–Ni alloy wire (ISW) was developed by Tokyo Medical and Dental University and marketed under the brand name L&H® Titan wire. Low-hysteresis wires deliver relatively stable orthodontic force in oral cavities [1]. In contrast to the hardness and stiffness of stainless steel wires, ISW offers three main advantages, namely shape memory, super elasticity, and absorption of shock and vibration [2]. Thus, individual occlusion through orthodontic treatment can be easily achieved using the ISW technique.

Figure 1: Facial photographs before treatment.
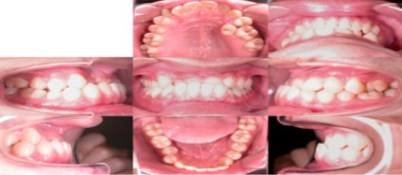
Figure 2: Intraoral photographs before treatment.
A 20-year-old man arrived at the dental clinic presenting with occlusion of his anterior teeth (Figure 1 and Figure 2). The Angle classification was Class III malocclusion. Furthermore, tooth #25 was blocked palatally in the upper left dental arch. At the anterior occlusion, the patients upper and lower incisors exhibited edge-to-edge contact. This case report provides details of ISW application for the treatment of the Class III malocclusion with anterior crossbite dentition.
History
The patient had no history of systemic diseases. He had two impacted third molars, specifically in teeth #38 and #48 (Figure 3).

Figure 3: Panoramic film before treatment.
Treatment Plan
and Progress
The following treatment plans were established: (1) Extraction of teeth #38 and #48; (2) Full-mouth direct bonding through bracket and ISW application; (3) Placing the crossbite arch between #13 and #23; and (4) Bringing #25 into alignment.
We initially extracted teeth #38 and #48. Next, we applied ISW with a crossbite arch between #13 and #23, thus forming a loop between #11 and #21 for anterior crossbite correction. A 100-gf open coil spring was placed between #24 and #26 to create space for #25 (Figure 4).

Figure 4: 0 weeks of active treatment.
After 2 weeks of active treatment, the anterior teeth formed edge-to edge contact. The ISW Multi-bends Edgewise Arch Wire (MEAW) [3] was applied on the upper right dentition for additional space creation (Figure 5). Anterior crossbite was corrected using the ISW crossbite arch technique. Meanwhile, the distalization of #27 was performed and Class III intermaxillary elastics were used to prevent the lower anterior teeth from flaring out (Figure 6).

Figure 5: 2 weeks of active treatment.

Figure 6: 3.5 Months of active treatment.
After 9.5 months, #26 moved distally because of the use of the stopper and 150-gf open coil spring. Simultaneously, #25 was tied with the ligature wire to lightly guide its movement to the buccal side (Figure 7).

Figure 7: 9.5 Months of active treatment.
After 16 months of active treatment, satisfactory occlusion was achieved (Figure 8 and Figure 9).

Figure 8: Facial photographs after treatment.

Figure 9: Intraoral photographs after treatment.
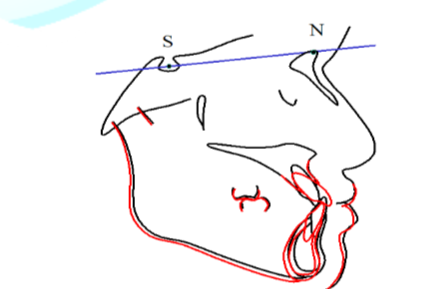
Cephalometric analysis results and superimposition revealed that the upper incisors were tipping outside between 120.1° and 135.0° on the Frankfurt horizontal plane (Figure 10 and Figure 11). The mandibular plane angle increased from 17.7° to 19.4°.
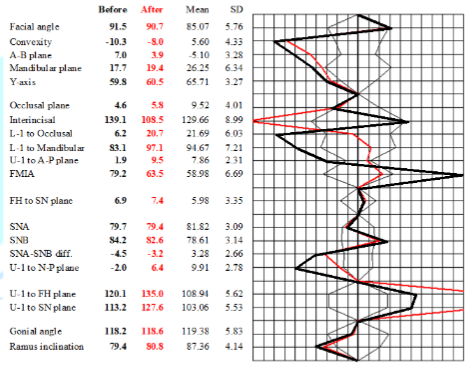
Figure 10: Cephalometric analysis. Black and red lines indicate positions before and after treatment, respectively
Discussion
In 1988, Graber defined crossbite dentition as a malocclusion in which one or more teeth might be abnormally positioned in reference to the opposing teeth. The reported incidence of anterior dental crossbite is 4%-5% [4]. The causes of reduced anterior crossbite dentition are inadequate arch length, trauma, a repaired cleft lip, an over-retained deciduous tooth, or length discrepancy between the maxilla and mandible [5]. In 1981, Rakosi and Schilli also described some of the effects of environmental factors, such as mouth-breathing and oral habits, on the etiology of Class III malocclusion. A removable acrylic plane can be used during orthodontic treatment of anterior crossbite cases of early mixed dentition [6]. Furthermore, a palatal plate with anterior springs or a quad-helix appliance to which springs can be soldered can be considered if patients are willing.
Deciding the treatment for Class III cases is always challenging in orthodontics because it is difficult and time consuming [7]. The key to achieving successful treatment outcomes lies in accurate differential diagnosis of a Class III case as a dental functional or skeletal problem. At the beginning of active treatment, we discovered that our patient exhibited a true skeletal Class III problem according to the results of a cephalometric analysis; however, clinical examination of the edge-to-edge contact of the anterior teeth revealed mild functional interference around the anterior teeth. Therefore, the crossbite dentition could be corrected without surgery. After 16 months of active orthodontic treatment, crowding was relieved and an adequate overbite and over jet were attained.
Previously, the crossbite arch dentition could not be easily corrected because treatment of anterior crossbite usually required a lingual arch with finger-like springs and a bite plane [8]. Moreover, available treatments that required a lingual arch with springs were associated with certain disadvantages. First, torque or space control was limited, and designing orthodontic appliances based on the force of the mechanism was difficult. Second, the appliances could injure the temporomandibular joint and induce some problems while using the bite plane [5]. Third, additional effort and time was sometimes required to prepare an acrylic resin or block for the orthodontists to apply on patients. In summary, an efficient and simple design for treating patients with crossbite arches is necessary. ISW crossbite arches are easily bent and do not hurt the joints because they do not increase the occlusal height (Figure 12).
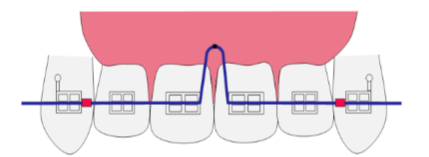
Most importantly, the degree of correction can be estimated in advance by altering the position of stoppers; furthermore, correcting crossbite requires less time and can be performed immediately at dental clinics.
References
2. Garrec P, Tavernier B and Jordan L. Evolution of flexural rigidity according to the cross-sectional dimension of a superelastic nickel titanium orthodontic wire (2005) Eur J Orthod 27: 402-407. https://doi.org/10.1093/ejo/cji014
3. Beane RA Jr. Nonsurgical management of the anterior open bite: a review of the options (1999) Semin Orthod 5: 275-283. https://doi.org/10.1016/S1073-8746(99)80021-8
4. Major PW and Glover K. Treatment of anterior cross-bites in the early mixed dentition (1992) J Can Dent Assoc 58: 574-575, 578-579.
5. Prakash P and Durgesh BH. Anterior Crossbite Correction in Early Mixed Dentition Period Using Catlans Appliance: A Case Report (2011) ISRN Dent 298931. https://dx.doi.org/10.5402%2F2011%2F298931
6. Jirgensone I, Liepa A and Abeltins A. Anterior crossbite correction in primary and mixed dentition with removable inclined plane (Bruckl appliance) (2008) Stomatologija 10: 140-144.
7. Thalanki LP. Nonsurgical treatment of Class III malocclusion (2007) J Mass Dent Soc 56: 40.
8. Ingervall B, Gollner P, Gebauer U and Frohlich K. A clinical investigation of the correction of unilateral first molar crossbite with a transpalatal arch (1995) Am J Orthod Dentofacial Orthop 107: 418-425. https://doi.org/10.1016/S0889-5406(95)70095-1*Corresponding author
Jian-Hong Yu, Professor, School of Dentistry, College of Dentistry, and Dean, Department of Orthodontics, China Medical University Hospital, Taichung-40402, Taiwan, R.O.C. E-mail: kenkoyu@mail.cmu.edu.tw
Citation
Chang YC, Tsai MK and Yu JH. Improved super-elastic Ti–Ni alloy wire treatment for skeletal class III malocclusion with anterior crossbite dentition (2019) Dental Res Manag 3: 6-8.
Keywords
Super-elastic Ti–Ni alloy, Orthodontic treatment, Crossbite dentition and Cephalometric analysis
