
 PDF
PDF
Introduction
With the development of science and technology, great changes have taken place in dental medical equipment and technology [1]. Digital technology has been rapidly disseminated in the field of stomatology [2,3]. Fast and accurate digital impression acquisition technology is the inevitable trend of future development. Digital impressions produced by intraoral and extraoral are two entry points for data acquisition. The extraoral method transfers clinical information to technicians by scanning impressions or plaster models for prosthetic reconstruction [4]. But, in the process of making impression and pouring gypsum model, it is unavoidable to produce the shrinkage of impression material, expansion in the process of gypsum hardening and various human factors, which ultimately decrease the accuracy of the digital model. Therefore, the precision of the prosthesis produced by direct method is better than that made by traditional impression [5,6].
In 1987, Sirona successfully developed the first set of in-mouth digital impression system CEREC [7]. After more than 30 years of development, digital impression technology has made rapid progress. At present, CEREC, LavaTM C.O.S, iTero, Trios and other systems are widely used in the field of prosthodontics [8]. In 2014, the Trios intraoral scanner (3 Shape Incorporated, Denmark) entered the Chinese market. Trios do not need to be sprayed in the oral cavity in advance, which provides great convenience for obtaining the intraoral digital model.
Since intraoral scanning impression technology became more and more widely available, more clinical studies should be performed to found out the appropriate parameters for clinical practice of intraoral scanning technology. Scanning number is one of the important parameter which not only has an effect on the efficiency of clinical practice, but also has an effect on the accuracy of the 3D reconstruction model. Theoretically speaking, more scanning number for a model will offer more details which will increase the accuracy of the digital model. But, is it true and necessary to do so? This paper mainly evaluated the appropriate parameters of scanning number for the accuracy of digital model by the Trios.
Materials and Methods
In order to avoid other effect from intraoral situation, 30 gypsum models in five conditions were collected and divided to 5 groups. Before scanning, these standard gypsum models were prepared and cleaned to ensure that there were no impurities in the models.
The scanning process was as flowing (Figure 1a). Connected Trios correctly, selected the research model function and entered the scan interface. The scanner was placed on the lingual side of the middle incisor, at an angle of 45° to the teeth. After starting the scan, the scanning gun moved slowly to the distal of the dental arch. During the movement, it always faced the teeth at a 45° angle. After bypassing the distal surface of the second molar, the scanning gun was slowly moved back from buccal side of the second molar to the middle line of the dental arch. Scan the other side of the dental arch in the same way and control the number of scanned sheets to 400 pictures.

Figure 1(a): Experimental flow chart.
After opening the 3 Shape Dental System (3 Shape Incorporated, Denmark), we used the 3D preview function to reconstruct the 3D version of the impression (Figure 1b), capture the 2D plane, and measured the distance of the points on each model separately.

We measured the buccal-lingual thickness of maxillary central incisors, the length from the medial to the distal of buccal cusps of maxillary second molars, the crown width of mandibular central incisors, the buccal-lingual thickness of maxillary central incisors requiring a veneer, the buccal-lingual width of the inlay of the mandibular first molar. Each model was measured three times and recorded as A1, B1, C1, D1, and E1.
Scanned the same model in the same way with a slower scanning speed, increased the image stitching, and controlled the number of scanned sheets to 1000 sheets as A2, B2, C2, D2, E2.
Statistical Analysis
The paired t-test was used to compare the differences between the two groups. Data was shown in mean ± standard deviation in each group. The test level α was set to 0.05. P <0.05 was considered statistical significant.
Results
The effect of scanning number on the precision of digital impression of natural tooth
The 1000 scanning number groups caused more time while the reconstruction process of 400 scanning number groups were more smoothly. Whats more, splicing distortion could be obviously observed in the 1000 scanning number groups in the 3D reconstructed models. Especially, the distortions in the labial side of the crown and gingival of maxillary incisor in A2, the occlusal surface in B2, the labial side of the crown in C2 were severed compared with the 400 scanning number groups (A1, B1, C1) (Figures 2-4). The differences of scanning data between the three groups were: 7.221 ± 0.010mm (A1), 6.768 ± 0.069mm (A2). 5.839 ± 0.06mm (B1), 5.524 ± 0.025mm (B2). 4.802 ± 0.036mm (C1), 4.332 ± 0.044mm (C2) (Supplementary file 1). They were all statistically significant (P <0.001). All of these suggested that 1000 scanning number required more time but it could not offer a more smoothly scanning process and induced distortions in the reconstruction of 3D models.
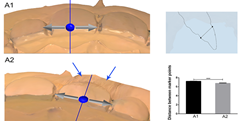
Figure 2: Three-dimensional preview and two-dimensional measurement diagram of group A. ***P <0.001.
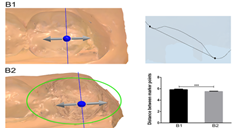
Figure 3: Three-dimensional preview and two-dimensional measurement diagram of group B. ***P <0.001.
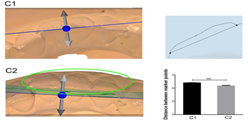
Figure 4: Three-dimensional preview and two-dimensional measurement diagram of group C. ***P <0.001.
The effect of scanning number on the precision of digital impression of maxillary central incisors requiring a veneer
D2 in the anterior veneer preparation group could not offer more details of the prepared teeth, but it caused more time in the scanning process. And the distortion could be found in the ridge of the labial and lingual side of the crown in maxillary central incisor (Figure 5) which could affect the esthetic outcome and caused restoration failure of the veneer. Whats more, the difference of scanning data between two groups was: 7.23 ± 0.026mm (D1), 6.932 ± 0.020mm (D2) (Supplementary file 1). The difference of measurement was statistically significant (P <0.001).
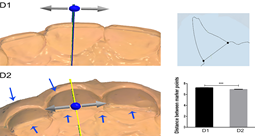
Figure 5: Three-dimensional preview and two-dimensional measurement diagram of group D. ***P <0.001.
The effect of scanning number on the precision of digital impression of mandibular first molar inlay
Similar to group D, E2 in inlay tooth preparation group also didnt display more image details, but it took longer time than group D, and the reconstruction efficiency was poor. The distortion also could be found in the buccal side of the crown. The difference of scanning data between the two groups was: 6.568 ± 0.022 (E1), 6.368 ± 0.023 (E2) (Supplementary file 1). The difference of measurement was statistically significant. (P <0.001) (Figure 6).
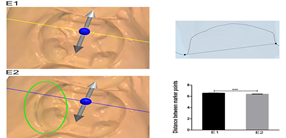
Figure 6: Three-dimensional preview and two-dimensional measurement diagram of group E. ***P<0.001.
This distortion in the 1000 scanning number groups would cause incompatibility which affected product efficacy adversely or induced restoration failure.
Discussion
Theoretically speaking, more scanning number for a model will increase the accuracy of the digital model. In this study, we explored the appropriate parameters of scanning number for producing the accuracy of digital impression in clinical practice. We found that 1000 scanning number groups could not offer more details compared to 400 scanning number groups, and it could cause 3D reconstruction distortion and longer scanning time all of which could induce esthetic out problem and restoration failure.
In 1985, Professor Werner Mormann put forward the concept of digital impression for the first time; a new technology of impression making based on digital idea came into being [9]. Researchers [10] studied the edge vertical distance of 30 right maxillary second premolars made by traditional impression method and digital impression method. The results showed that the edge adaptability of single crown by digital impression method was better than that of traditional impression method. The scholars compared the intraoral digital model obtained by Trios with the intraoral model prepared by silicone rubber, and the results showed that there was no significant difference between them. It was considered that the accuracy of intraoral scanning digital impression can reach the clinical standard [11].
Ultrafast Optical SectioningTM [12] and confocal microscopy are used in the Trios system, so the scanning speed per unit time is faster than that of other systems. Sandblasting on the surface of teeth and soft tissues can be omitted, which greatly shortens the operation time and improves the acceptance of patients [13]. The digital model is displayed on the screen as a three-dimensional image. The operator can rotate the model and observe the shape of the abutment from multiple angles [14], and transmit clinical information to the studio simply and quickly. At the same time, patients are more inclined to accept the way of making digital impressions by intraoral chairside scanning [15,16].
Considering the complicated intraoral situation, we chose the standard gypsum model, which required that the gypsum model cannot reflect light and be easily scanned and imaged. When using Trios, we need to determine the number of scanning sheets according to the size of the area to be scanned. This is mainly to avoid data mosaic caused by repeated scanning. In this experiment, the image deformation of the three-dimensional preview was observed in the experimental groups A2, B2, and C2, This may be due to the fact that when scanning normal natural teeth, the number of scanned images was too large, so that the image was fitted when the three-dimensional image was reconstructed, which caused the image to be deformed. The thinnest veneer is 0.2mm-0.3mm, which requires an extremely high precision [17]. In the scanned image of group D2, the cutting edge of the preparation part was rough and not smooth, which might mislead the mechanic to make a veneer that didnt match the preparation body, and eventually lead to restoration failure of the veneer. Since the number of scans was increased, the data processing time was very slow. We observed that during the scanning of the anterior veneers and posterior inlays, the scanning time was greatly extended and the 3D reconstruction efficiency decreased significantly. In order to avoid data splicing during digital scanning, changing the angle to fill the unswept area is an effective way to produce a more accurate prosthesis and the scanning time can be reduced. During the scanning process, when the number of scanned sheets is about 1000, the device will be stuck, which greatly affects the scanning efficiency.
According to our experiment, if there are too many scanning sheets in the same area, it will cause data mosaic, and it will take more time for pictures to build three-dimensional images, which will result in errors and data distortion, so too many scanning sheets have an impact on the accuracy of digital impression. And further research is needed to investigate the effect of other parameter on the clinical scanning accuracy.
Acknowledgments
Our study was supported by the National Natural Science Foundation of China (31400808, 81570979, and 21402018). This study was also supported by Science & Technology Committee of Yubei District (2015-01), Program for Innovation Team Building at Institutions of Higher Education in Chongqing in 2016 (CXTDG201602006) and Chongqing Municipal Key Laboratory of Oral Biomedical Engineering of Higher Education (Yujiaoke (2014)-55) and the Science and Technology Innovation Program of Social Undertakings and Peoples Livelihood Security of Chongqing Science and Technology Commission (cstc2016shms-ztzx0045). And including this study, Xiaomian Wu was awarded the Excellent Graduation Thesis Instructor of Chongqing Medical University in 2018.
References
1. Birnbaum NS and Aaronson HB. Dental impressions using 3D digital scanners: virtual becomes reality (2008) Compend Contin Educ Dent 29: 494, 496 and 498.
2. Fasbinder DJ. Computerized technology for restorative dentistry (2013) Am J Dent 26: 115.
3. Abdulaziz ABA, Kiho K, Finkelman MD, Zandparsa R and Hirayama H. The effect of variations in translucency and background on color differences in CAD/CAM lithium disilicate glass ceramics (2014) J Prostho 23: 213-220. https://doi.org/10.1111/jopr.12080
4. Davidowitz G and Kotick PG. The Use of CAD/CAM in Dentistry (2011) Dent Clin North Am 55: 559-570. https://doi.org/10.1016/j.cden.2011.02.011
5. Tsitrou EA, Northeast SE and Noort RV. Evaluation of the marginal fit of three margin designs of resin composite crowns using CAD/CAM (2007) J Dent 35: 68-73. https://doi.org/10.1016/j.jdent.2006.04.008
6. Aragón ML, Pontes LF, Bichara LM, Flores-Mir C and Normando D. Validity and reliability of intraoral scanners compared to conventional gypsum models measurements: a systematic review (2016) Eur J Orthod 38: 429. https://doi.org/10.1093/ejo/cjw033
7. Amin S, Weber HP, Finkelman M, El Rafie K, Kudara Y, et al. Digital vs. conventional full‐arch implant impressions: a comparative study (2016) Clin Oral Implants Res 28: 1360-1367. https://doi.org/10.1111/clr.12994
8. Renne W, Ludlow M, Fryml J, Schurch Z, Mennito A, et al. Evaluation of the accuracy of 7 digital scanners: An in vitro analysis based on 3-dimensional comparisons (2017) J Prosthet Dent 118: 36-42. https://doi.org/10.1016/j.prosdent.2016.09.024
9. Pieper R. Digital impressions--easier than ever (2009) Int J Comput Dent 12: 47-52.
10. Ng J, Ruse D and Wyatt C. A comparison of the marginal fit of crowns fabricated with digital and conventional methods (2014) J Prosthet Dent 112: 555-560. https://doi.org/10.1016/j.prosdent.2013.12.002
11. Fleming PS, Marinho V and Johal A. Orthodontic measurements on digital study models compared with plaster models: a systematic review (2011) Orthod Craniofac Res 14: 1-16. https://doi.org/10.1111/j.1601-6343.2010.01503.x
12. Berrendero S, Salido MP, Valverde A, Ferreiroa A and Pradíes G. Influence of conventional and digital intraoral impressions on the fit of CAD/CAM-fabricated all-ceramic crowns (2016) Clin Oral Investig 20: 2403-2410. https://doi.org/10.1007/s00784-016-1714-6
13. Xie YL and Shen G. Accuracy and reproducibility of intraoral scanning in vivo (2016) Shanghai Kou Qiang Yi Xue 25: 593-599.
14. Sang J, Lee and Gallucci GO. Digital vs. conventional implant impressions: efficiency outcomes (2013) Clinical Oral Implants Research 24: 111-115. https://doi.org/10.1111/j.1600-0501.2012.02430.x
15. Wismeijer D, Mans R, Van GM and Reijers HA. Patients preferences when comparing analogue implant impressions using a polyether impression material versus digital impressions (Intraoral Scan) of dental implants (2015) Clin Oral Implants Res 25: 1113-1118. https://doi.org/10.1111/clr.12234
16. Yuzbasioglu E, Kurt H, Turunc R and Bilir H. Comparison of digital and conventional impression techniques: evaluation of patients perception, treatment comfort, effectiveness and clinical outcomes (2014) Bmc Oral Health 14: 10-10. https://doi.org/10.1186/1472-6831-14-10
17. Turgut S, Bagis B and Ayaz EA. Achieving the desired colour in discoloured teeth, using leucite-based cad-cam laminate Systems (2014) J Dent 42: 68-74. https://doi.org/10.1016/j.jdent.2013.10.018
*Corresponding authors
*Xiaomian Wu, Chongqing Key Laboratory of Oral Diseases and Biomedical Sciences, College of Stomatology, Chongqing, Medical University, Chongqing, China, E-mail: wuxiaomian@hospital.cqmu.edu.cn , wuxiaomian898@163.com
*Ping Ji, Department of Oral and Maxillofacial Surgery, Stomatological Hospital of Chongqing Medical University, 426 Song-Shi North Road, Chongqing, 401147, P.R. China, E-mail: jiping@hospital.cqmu.edu.cn
Citation
Yang ZQ, Deng F, Hu XL, Wen YX, Ji P, et al. The effect of the scanning number on accuracy of digital impression (2019)Dental Res Manag 3: 38-41
Keywords
Digital impressions, Oral impression technique, Scanning number, 3 shape trios.
