
 PDF
PDF
Introduction
Diabetes in all its forms imposes unacceptably high physical, social and economic burden on the communities and countries at all income levels. Pre-diabetes is a serious health condition where blood sugar levels are higher than normal, but not high enough yet to be diagnosed as type 2 diabetes. Pre-diabetes puts one at an increased risk of developing type 2 diabetes, heart disease, and stroke [1].
The risk factors for Pre-diabetes include:
· Being overweight
· Being 45 years or older
· Having a parent, brother, or sister with type 2 diabetes
· Being physically active less than 3 times a week
· Ever having gestational diabetes (diabetes during pregnancy) or giving birth to a baby who weighed more than 9 pounds
· Having Polycystic Ovary Syndrome
· Race and ethnicity (certain races are more prone)
Diabetes in the UAE
World Health Organization (WHO)-Diabetes country profiles, 2016 illustrate that Diabetes accounts to 3% mortality all ages in the UAE [2]. Figures from the International Diabetes Federation (IDF) reveal that, in 2017, 17.3% of the United Arab Emirates (UAE) population between the ages of 20 and 79 had type 2 diabetes. There are over 1 million people living with diabetes in the UAE, placing the country at 15th place worldwide for age-adjusted comparative prevalence. Trends also indicate that the prevalence of diabetes in the UAE is rising at a faster rate than both the MENA region (Middle East and North Africa region) and the rest of the world. Rapid economic growth, sedentary lifestyles and unhealthy diets characteristic to the UAE are all risk factors, leading to the number of people with diabetes expecting to double to 2.2 million by 2040 [3].
Diabetes in Dubai
Additionally, Dubai Diabetes Survey conducted by Dubai Health Authority (DHA) in 2017 reported the total prevalence of Diabetes amongst Emiratis in Dubai is 19%, while the undiagnosed diabetes cases amongst Emiratis accounts to 11% and the prevalence rate of pre-diabetes amongst Emiratis is 18.6% [4]. This alarmingly high percentage undoubtedly represents a worrying indication about the future impact of diabetes as a major threat in Dubai.
Oral Health Consequences of Diabetes
Of late, there is an ample evidence to explain the two-way relationship between diabetes and periodontal disease. The primary cause of periodontal disease is plaque that contains pathogenic bacteria that cause inflammation of the gums, leading to the destruction of tooth-supporting periodontal tissues. Physiologically active substances associated with the inflammation are released from periodontal pockets and then delivered to all parts of the body, where they increase insulin resistance. Additionally, the hyperglycemic state weakens the immune function which protects the body from bacterial infection, leading to easy development and progression of periodontal disease.
Considering the facts and figures expressed above, there is a dire need to develop an effective screening tool to be able assess the risk for diabetes and direct the efforts towards its prevention across Dubai. Since the natural history for diabetes is well understood and it is detectable in the preclinical stage, it is wise to devise a cost-effective, safe and acceptable screening tool that could be easily and widely used in any environment. Diabetes risk calculation can be performed by several health professionals in different settings, of which a dental office could be an ideal site to carry it out as the former caters to patients of all age groups with varied medical backgrounds. More so, the nature of dental treatments mandates multiple visits for most patients, and dental professionals easily develop a rapport with the patients and thus it is conceived feasible to administer a simple, chair-side screening tool for diabetes in the dental offices setting across Dubai. Consequently, if this tool proves accurate and can detect the affected patients, it will prove very valuable not only to prevent the progression of active diabetes, but also limit its complications.
On a similar line, the Centers for Disease Control and Prevention (CDC) also suggest that the dental office may be a useful setting in which to identify individuals with undiagnosed Pre-diabetes or diabetes. However, no study has been conducted so far to estimate the risk for diabetes in the population of Dubai, especially in a dental setting. This is the first study of this kind in Dubai
Aim of the study
To detect the individuals who are at high risk of developing diabetes and correlate with their clinical periodontal disease status.
Materials and Methods
A cross-sectional study was carried out in a primary health center of DHA to assess the risk for diabetes, using the Finnish Diabetes Risk Score (FINDRISC) questionnaire followed by the HbA1c blood test stipulated only for the patients identified to be at risk. However, the periodontal examination was carried out for all the patients regardless of the risk category (Figure 1).
Sample design and Subjects
A simple random sample of the population visiting the dental clinic of Al Mizhar Primary Health Centre was chosen for this study. Both females and males aged 20-70 years were included from the morning and afternoon shifts of dental clinics at the above mentioned health center. Patients sitting in the waiting area of dental clinics were approached and if found interested, a written consent was given to them to be signed and the entire procedure was explained. A total of 20 participants refused to participate, the response rate was 95%. Later, consent forms were given to a total of 400 participants, out of whom 16 were excluded.
Exclusion criteria
· Patients previously diagnosed with diabetes, Pregnant females and
· Patients taking anti-coagulant medications.
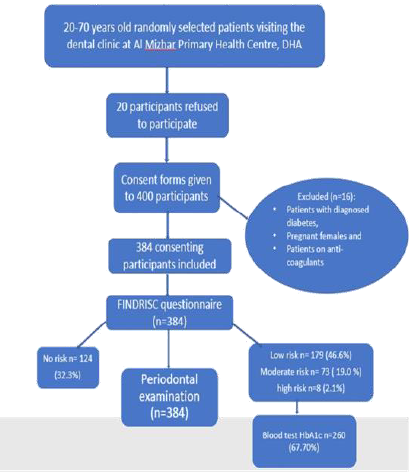
Figure 1: Flowchart depicting the procedure of sample selection and clinical examination.
Finally, 384 consenting participants were included in the study. The subjects were screened over a period of 12 months, with 32 patients screened each month, divided over five days a week (around 6 patients per day) in the dental setting of Al Mizhir Primary health center, DHA, Dubai. The screening was accomplished daily based on the availability of the sample with the required criteria.
The Questionnaire
A screening chart that was simple, practical, non-invasive and inexpensive namely FINDRISC was used. FINDRISC has been successfully implemented as a practical screening instrument to assess diabetes risk and to detect undiagnosed type 2 diabetes in diverse populations.
FINDRISC questionnaire is a validated risk assessment tool to predict type 2 diabetes. It estimates the probability of a person to develop diabetes within the next 10 years. It requires no laboratory testing and uses age, Body Mass Index (BMI), physical activity, vegetable and fruit intake, medical treatment of hypertension, history of hyperglycemia and family history to determine risk of developing diabetes [5].
After procuring the consent forms and completing the registration formalities, each patient was given a FINDRISC questionnaire (appendix 1), which takes 2-3 minutes to complete. The questionnaire has eight scored questions, with the total test score providing a measure of the probability of developing type 2 diabetes. The results categorize the participant as high risk, moderate risk, low risk or no risk individual. Resultantly, patients falling in the no risk category received a report on their condition and given printed advice and tips on how to stay healthy (Table 1) [6].
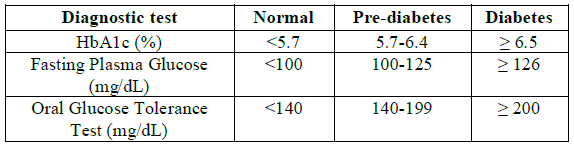
Table 1: CDC recommendations for Pre-diabetes and diabetes identification.
HbA1c Blood Test
Next, patients at the high risk, moderate risk or low risk categories were requested to take a finger-prick blood sample collection for in-office HbA1c testing with Metrika A1c Now (Bayer Health Care, Sunnyvale, CA), as rapid one-step test. It takes five minutes for the results to appear and the reference HbA1c values were followed as per the CDC guidelines.
Periodontal Examination and Charting
Five dentists and five assistants were involved in the examination, which were trained and calibrated before initiating the data collection. All the patients attended their usual appointment and a periodontal charting was done for them after filling out the FINDRISC forms and the blood test. Community Periodontal Index of Treatment Needs (CPITN) was used for the periodontal evaluation. Three indicators of periodontal status are used for this assessment [7]:
· Presence or absence of gingival bleeding
· Supra or sub-gingival calculus
· Periodontal pockets-subdivided into shallow (4-5mrn) and deep (6mm or more).
A specially designed lightweight probe with a 0.5mm ball tip was used, bearing a black band between 3.5 and 5.5mm from the ball tip.
Sextants: The mouth is divided into sextants defined by teeth numbers 18-14, 13-23 24-28,38-34, 33-43 and 44-48. A sextant should be examined only if there are two or more teeth present and not indicated for extraction. When only one tooth remains in a sextant, it should be included in the adjacent sextant.
Statistical Analysis: For the purpose of inter-examiner reliability, the Kappa coefficient (Cohens Kappa) was used as a measure of agreement between the examiners. 10% of the sample was extracted and measured and a value of 0.6 was recorded which shows good agreement.
The collected data were loaded into Microsoft excel and thereafter proof reading was done. Statistical analysis was carried out using IBM-SPSS version 24. All the categorical variables were expressed as proportion and continuous variables as means and standard deviation. To know the association between socio-demographic factors and FINDRISC score, HbA1c and periodontal health, the Pearson chi square and contingency coefficients were used. Pearson correlation was used to figure out the correlation between FINDRISC score, HbA1c levels and periodontal measurements. Further, to find out the factors influencing the periodontal charting, regression analysis was performed keeping the periodontal scores as the dependent variable. The predicted probabilities were calculated for periodontal scores, later receiver curve was also drawn to know the specificity and sensitivity of the periodontal scores based on the predicted probabilities values. The significance level was fixed at P<0.05 with 95% confidence interval throughout.
Ethical Approvals: Approval from Ethical Committee for Scientific Research, Dubai Health Authority was obtained.
Results
Distribution of the Study Participants
Out of a total of 384 subjects interviewed, majority 71.6% (275) were female participants and 61.2 % (235) were local population. The mean age of the participants was 38.90 ± 10.74 and a large proportion i.e. 52.9% (203) belonged to 20-40 years, while 44.55% (171) belonged to 41-60 years age group. In relation to health conditions of the participants, 87.5% (336) were healthy individuals (Table 2 and Figure 2).
All the 384 participants completed the FINDRISC questionnaire, of which 32.3% (124) participants were categorized as having no risk followed by 46.6% (179) participants were with low risk of developing diabetes, while 19% (73) and 2.1% (8) of them were having moderate and high risk of developing diabetes respectively. Further, a total of 32.3% (124) were exempted from the blood test as they were at a low risk from the FINDRISC questionnaire and the remaining participants were tested for serum HbA1c Level. Accordingly, 46.1% (177) participants had normal HbA1c followed by 18.0% (69) and 3.6 % (14) participants were Pre-diabetic and diabetic respectively. All the participants were subjected to periodontal charting and it was observed that 19.3% (74) participants had a pocket measuring more than 4mm and 15.9% (61) had periodontal pocket measuring more than 6mm (Table 3 and Figure 3).
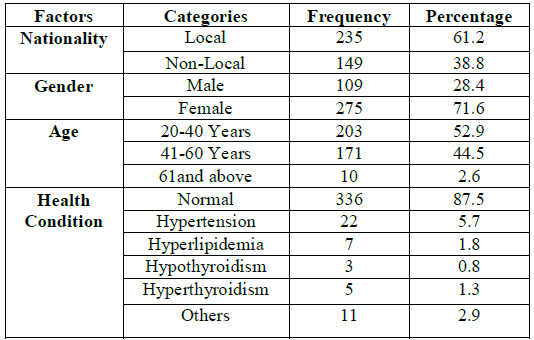
Table 2: Distribution of the study population according to the demographic factors and health condition.
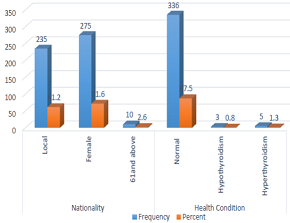
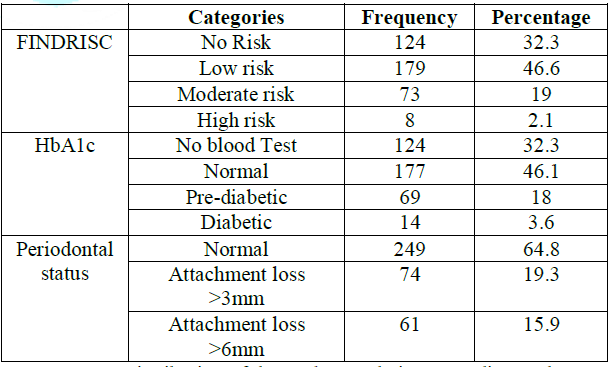
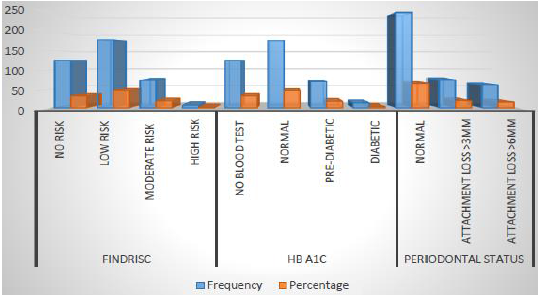
Figure 3: Distribution of the study participants according to FINDRISC, HbA1c and Periodontal Condition.
Association between Demographic Factors and FINDRISC Score
With respect to nationality, local participants had greater scores of FINDRISC questionnaire as compared to the non-local participants with 52.3% (123) vs. 37.6% for low risk, 19.6% (46) vs. 18.1% (27) for moderate risk and 2.6% (6) vs. 1.35(2) high risk scores respectively. Also, female participants had a higher FINDRISC score compared to male participants with 20.4% (56) vs. 15.6% (17) for moderate risk score, while 2.9% (8) of the females had a high-risk score whereas no male subjects were found with FINDRISC score of high risk. In terms of age, higher the age of the participant, greater is the FINDRISC score with 60% (6), 33.9% (58) and 4.4% (9) of the high-risk score for the 20-40 years, 41-60 years and 61 years and above group respectively.
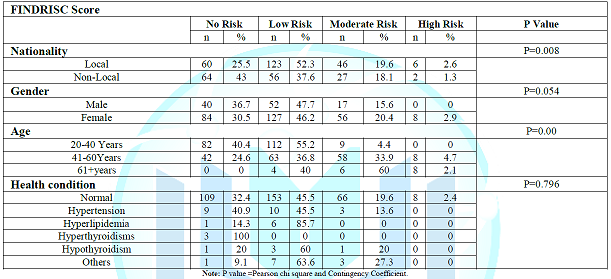

Table 5: Association between the Demographic Factors and HbA1c Score.
The health condition of the participants had no significant association with the risk scores assessed by the FINDRISC questionnaire, however, only 1 subject with hypothyroidism (19.6%) and 3 subjects (27.3%) with other health conditions showed a moderate risk for diabetes (Table 4 and Figure 4).

Figure 4: Association between demographic factors and FINDRISC scores.
Association of Demographic Factors with Serum Hba1c Levels
The association of demographic factors with an HbA1c level showed fashion similar to that of FINDRISC Score. A total of 68.1% (47) and 85.7% (12) of the local participants had Pre-diabetic and diabetic levels of HbA1c compared to 31.9% (22) and 14.3% (2) of non-local Participants. Next, 60.9% (42) of the females were in the Pre-diabetic stage compared to 39.1% (27) of the males. Likewise, 57.1% (8) females and 42.9% (6) males were diabetic stage of HbA1c levels. With respect to age, 60.9% (42) belonging to 40-60 years were Pre-diabetic compared to the younger age group which is 34.8% (24), also 85.7% (12) participants had diabetes level of HbA1c compared to the younger counterparts 14.3% (2).
The health condition of the participants again posed no significant association with the HbA1c level, however, 2 subjects with hypertension and 2 subjects with hyperlipidemia had Pre-diabetes as measured by HbA1c (Table 5 and Figure 5).
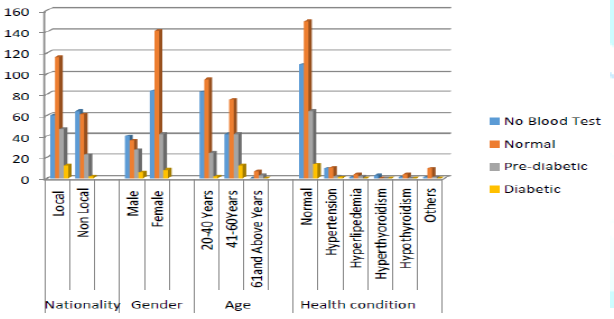
Figure 5: Association between demographic factors and HbA1c levels.
Association of Demographic Factors and Periodontal Condition
Among the subjects having periodontal loss of attachment 82.2% (37) were locals presenting with periodontal pockets more than 4mm compared to 17.8% (8) non-locals, similarly 72.5% (29) locals had a periodontal pocket more than 6mm compared to 27.5% (11) non-locals.
With respect to gender, a greater number of female subjects were observed with periodontal pocket more than 4mm 86.7% (39) vs. 13.3% (6). Similarly, pockets measuring 4mm was found more among the younger adults (20-40) 46.7% (21) vs. 42.2% (19), whereas pockets measuring more than 6mm were more among the older adults (41-60), 67.5% (27) vs. 32.5% (13) (Table 6 and Figure 6).
Association of FINDRISC Score, HbA1c Levels and Periodontal Conditions
The presented revealed that a statistically significant association between the periodontal condition and find risk scores as 66.7% (30) and 75% (30) subjects belonging to the low risk group had pockets measuring more than 4mm and 6mm respectively. Next, 11.1% (5) of the subjects in high risk group had pocket more than 4mm.
Similarly, 50% (20) of the subjects belonging to Pre-diabetic and 25% (10) subjects belonging to diabetic stage of HbA1c levels were observed with pockets more than 6mm. Additionally, 45.8% (127) of periodontally healthy subjects presented with normal HbA1c levels and 13.7% (38) of periodontally healthy subjects fall in the Pre-diabetic HbA1c category. These observations were statistically significant (Table 7 and Figure 7).
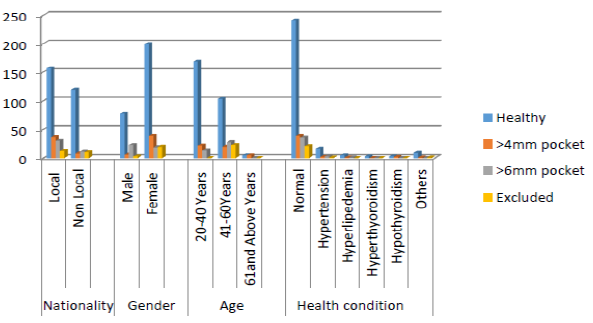
Figure 6: Association between demographic factors and periodontal condition.
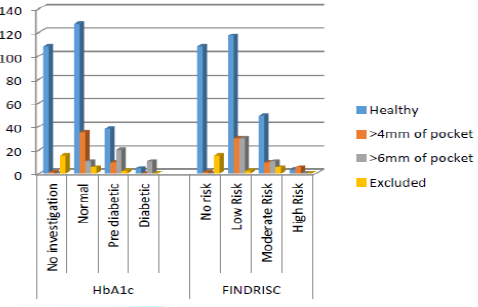
Figure 7: Association between FINDRISC score, HbA1c level and periodontal condition.
Accuracy of Periodontal Measurement
Using the regression model, the sensitivity and specificity periodontal diagnostic was assessed for the periodontal condition which showed 76.4% sensitivity and 82.01% of specificity. In addition, Area Under curve was measured using predictive probabilities of logistic regression for periodontal condition using receiver operating curve that showed a significantly good accuracy of periodontal measurement (Table 8).
Relationship between FINDRISC, HbA1c and Periodontal Scores
Further, a correlation matrix was established using the continuous scores of FINDRISC, HbA1c level and predicted probability of periodontal scores. The correlation matrix showed significant relationship between these three variables (Table 9).
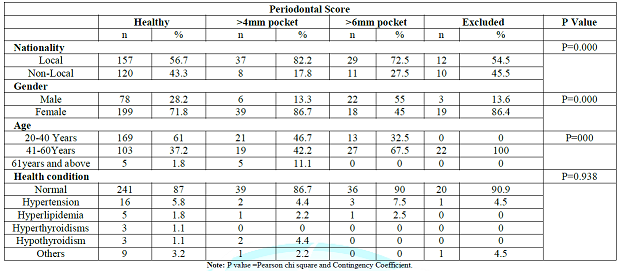
Table 6: Association between the demographic factors and Periodontal Condition.

Table 7: Association between the FINDRISC score, HbA1c Level and Periodontal condition.
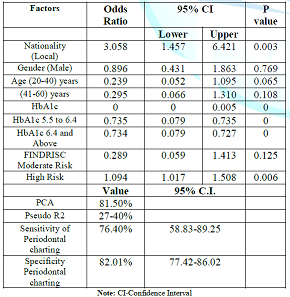
Table 8: Regression analysis for periodontal conditions and nationality, age, gender HbA1C and FINDRISC scores.

Table 9: The Correlation matrix between FINDRISC, HbA1c and Predictive probabilities of periodontal condition.
Discussion
Findings from the present study suggest a potential correlation between FINDRISC, HbA1c level and predicted probability of periodontal scores. Emirati participants and females posed a higher risk for diabetes. Female participants presented with more and deeper periodontal pockets too. All the high-risk participants belonged to a higher age group. It was also discerned that statistically significant association exists in terms of nationality, gender and age with FINDRISC score and the diabetic stage. However, the health condition of the participants in this study was found to have no significant association either with the HbA1c level or with the periodontal condition.
Almost two-thirds (67.7%) of the participants in this study were found to have low, moderate or high risk for diabetes and nearly a fifth of the surveyed population posed higher HbA1c levels indicating pre-diabetic or diabetic stages. An alarming proportion i.e. more than a fifth of the study sample (21.6%) were discovered to be either pre-diabetic or diabetic. Further, of all the pre-diabetic individuals, more than two-thirds (68.1%) were UAE nationals and likewise even amongst the diabetics, a majority (85.7%) were UAE nationals again. A potential explanation for this skewed distribution could be that due to the location of the study was a DHA health center where majority of the patients-cohort is formed by UAE nationals and very few non-nationals, that automatically justifies an overall higher prevalence of these conditions amongst them.
It is noteworthy that occurrence of diabetes was noticed in 3.6% of the study participants, which is much lower than the corresponding value outlined in the USA, UK and Australia being 9.4% 9, 6.6% and 6% respectively, as reported by their national statistics [8,9,10]. Further, in the present study, 20% of the participating Emiratis were found to be pre-diabetic, which is slightly higher than reported by Dubai Diabetes Survey conducted by DHA in 2017 (18.6%) [4]. In contrast, the rate of diabetic Emiratis in this study is only 5.1% which is clearly much lower than the Dubai survey (19%). The prevalence of pre-diabetes in the present study (18%) was slightly lower than that reported by S Maples et al. (19.2 %) and higher than that reported by National Health and Nutrition Examination Survey (NHANES) (17.31%) [11,12]. At the same time the diabetes percentage in the present study (3.6%) was observed to be higher than reported by S Maples et al. (1.2%) and NHANES (1.64%). Al Amiri et al. reported the prevalence of prediabetes, among overweight and obese Emirati children and adolescents in Sharjah as 5.4% and 0.87%, respectively, based on Oral Glucose Tolerance Tests (OGTT), which are much lower than the present study [13].
Unlike certain other studies, the present study revealed significant gender differences in the FINDRISC scores as well as HbA1c values with P=0.054 and P=0.008 respectively, these findings contrast the ones obtained by S Maples et al, and W.H. Herman et al, where no significant gender differences were noticed in the pre-diabetes and diabetes prevalence. Identical to the findings from the NHANES and S Maples et al, age was seen to be significantly associated with the presence of diabetes and pre-diabetes in the present study (P=0.00) [11,12,14].
The findings of this study were consistent with the Wijnand J Teeuw et al, where statistically significant association was found between the HbA1c levels and the periodontal status, and significantly greater number of subjects were spotted with deep pockets (more than 6 mm) in the pre-diabetic and diabetic groups as compared to the subjects with normal HbA1c levels (Table And Figure 8). The present study also indicates a highly significant association between the periodontal condition and risk for diabetes and the diabetic stage the p value being P=0.000, which is inconsistent with certain other studies such as Oelisoa Mireille et al. who found no significant association between fasting glucose and bleeding on probing [15,16].
There has been abundant evidence to support that the presence and severity of periodontal disease is highly associated with the diabetic stage and its complications. Severe periodontitis has been found to be associated with poor glycemic control after a 5-year period and subjects with Clinical Attachment Loss (CAL) of at least 6 mm had over six times the risk of poor glycemic control compared to those without it [17]. Additionally, an increase in mean CAL has been associated with an increase in HbA1c. Next, a significant increase in Impaired Glucose Tolerance (IGT) with mean Periodontal Probing Depth (PPD), with each additional millimeter mean PPD corresponding to 0.13% increase in HbA1c has been observed after 10-year follow-up [18]. Later, all studies in subjects with types 1 and 2 diabetes found that those with periodontal disease, especially severe disease, and edentulism, had higher risk for diabetes-related complications than participants without or with mild periodontal disease [19]. Lastly, severity of periodontal disease expressed by clinical attachment loss at follow-up was significantly associated with development of diabetes over ten years in a study [18]. However, due to their design and nature, cross-sectional studies are limited to only provide information about associations and are thus not able to an establish a causal relationship.
Limitations of the Study
· The small sample size of this study defers the extrapolation of the results to whole of Dubai population.
· No information around smoking (duration and frequency) has been recorded, since smoking is a known risk factor for periodontitis and plays a significant role in aggravating the complications caused due to diabetes, it would have been beneficial to do so.
Recommendations
· In light of the findings of this research, the routine application of the FINDRISC tool in the dental setting for the purpose of risk assessment and screening for diabetes and Pre-diabetes is highly recommended.
· It will be more beneficial if information about smoking is also recorded along with other risk factors, since it is a well-known risk factor for periodontal disease and at the same time aggravates the complications caused due to diabetes.
· Non-dental health care providers should be well informed about these results and made aware of the two-way relationship of diabetes and periodontal health to be able to collaborate with them for the purpose of early detection and prevention of the diabetes. The two primary goals of management of Pre-diabetes are lifestyle management to prevent the progression to type 2 diabetes and management of common Pre-diabetes comorbidities, both of which requires the effective contribution of the abovementioned stakeholders [20].
· The confirmation of the blood glucose by other standardized measurements such as OGTT and fasting blood glucose levels along with their clinical correlation would be ideal before initiating any discrete treatment for the diabetic patients, due to the reported overestimation of the blood glucose levels by the HbA1c [21,22].
Conclusions
The Diabetes Risk Score has proven to be very useful in identifying high-risk subjects and exhibits worrying high proportion of Pre-diabetes and diabetes among Dubai population. Filling in the Diabetes Risk Score may encourage a person who gets a high value to have his/her blood glucose measured and also to improve their lifestyle regardless their glucose levels. Additionally, many individuals with a high Diabetes Risk Score may have unrecognized, asymptomatic diabetes and, therefore, may require blood glucose testing for diagnosis, other clinical assessments, and therapy.
This study emphasizes that periodontal disease adversely affects glucose levels and promotes development of Pre-diabetes and diabetes and vice-versa. The results obtained here would affect the patients and families, health care providers, insurance companies, policy-makers and societies in general, due to the high prevalence of both periodontal disease and diabetes in Dubai afflicting immense physical, mental, social and economic consequences. Controlling and managing periodontal disease could be a new aspect to eventually include in the standards for diabetes care. It undoubtedly requires a shift in paradigm for management and prevention of diabetes and its complications. Dental setting could be successful platform to carry out the screening and risk stratification of diabetic patients, those could further be referred to the relevant medical provider for subsequent treatment and follow up.
Acknowledgments
The authors would like to thank Dr. Ghayath Aboud, Dr. Vijitha Saleem, Dr. Sameh Sulaiman and Dr. Darwish Al Sadik for their valuable input in the data collection process.
References
1. Prediabetes: Your Chance to Prevent Type 2 Diabetes
2. World Health Organization-Diabetes country profiles (2016) United Arab Emirates
3. Ogurtsova K, da Rocha JD, Huang FY, Linnenkamp U, Guariguata L, et al. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040 (2017) Diabetes Res Clin Practice 128: 40-45. https://doi.org/10.1016/j.diabres.2017.03.024
4. 2nd Phase of Dubai Diabetes Survey Results Revealed (2017) Dubai
5. Maurice vandersmissen JG and Godderis L. Evaluation of the Finnish Diabetes Risk Score (FINDRISC) for diabetes screening in occupational health care (2015) Int J Occupational Med Environmental Healt 28: 587-591. https://doi.org/10.13075/ijomeh.1896.00407
6. Lindström J and Tuomilehto J. The diabetes risk score: a practical tool to predict type 2 diabetes risk (2003) Diabetes Care 26: 725-731. https://doi.org/10.2337/diacare.26.3.725
7. Point-of-care prediabetes identification, American Medical Association
9. Diabetes and a lot of facts and stats, United Kingdom
10. Diabetes snapshot (2019) Australian institute of health and welfare
11. Maples S, Aldasouqi S, Little R, Baughman H, Joshi M, et al. Detection of Undiagnosed Prediabetes and Diabetes in Dental Patients: A Proposal of a Dental-Office-Friendly Diabetes Screening Tool (2016) J Diabetes Mellitus 6: 25-37. https://doi.org/10.4236/jdm.2016.61004
12. Estrich CG, Araujo MWB and Lipman RD. Prediabetes and Diabetes Screening in Dental Care Settings: NHANES 2013 to 2016 (2019) JDR Clin Trans Res 4: 76-85. https://doi.org/10.1177/2380084418798818
13. Al Amiri E, Abdullatif M, Abdulle A, Al Bitar N, Afandi EZ, et al. The prevalence, risk factors, and screening measure for prediabetes and diabetes among Emirati overweight/obese children and adolescents (2015) BMC Pub Healt 15: 1298. https://doi.org/10.1186/s12889-015-2649-6
14. Herman HW, Taylor GW, Jacobson JJ, Burke R and Brown MB. Screening for prediabetes and type 2 diab etes in dental offices (2015) J Pub Healt Dentistry 75: 175-182. https://doi.org/10.1111/jphd.12082
15. Teeuw WJ, Kosho MXF, Poland DCW, Gerdes VEA and Loos BG. Periodontitis as a possible early sign of diabetes mellitus (2017) BMJ Open Diabetes Res Care 5: e000326. https://doi.org/doi:10.1136/bmjdrc-2016-000326
16. Andriankaja MO and Joshipura K. Potential association between prediabetic conditions and gingival and/or periodontal inflammation (2014) J Diabetes Invest 5: 108-114. https://doi.org/10.1111/jdi.12122
17. Borgnakke WS, Ylostalo PV, Taylor GW and Genco RJ. Effect of periodontal disease on diabetes: systematic review of epidemiologic observational evidence (2013) J Clin Periodontol 40: S135-S152. https://doi.org/10.1111/jcpe.12080
18. Saito T, Shimazaki Y, Kiyohara Y, Kubo IK, Iida MM, et al. The severity of periodontal disease is associated with the development of glucose intolerance in non-diabetics: the Hisayama study (2004) J Dental Res 83: 485-490. https://doi.org/10.1177/154405910408300610
19. Shultis WA, Weil EJ, Looker HC, Curtis JM, Shlossman M, et al. Effect of Periodontitis on overt nephropathy and end-stage renal disease in type 2 diabetes (2007) Diabetes Care 30: 306-311. https://doi.org/10.2337/dc06-1184
20. Management of Prediabetes, American association of clinical endocrinologists
21. When is hemoglobin A1C inaccurate in assessing glycemic control?
22. Radin SM. Pitfalls in Hemoglobin A1c Measurement: When Results may be Misleading (2013) J Gen Intern Med 29: 388-394. https://doi.org/10.1007/s11606-013-2595-x
*Corresponding author
Shiamaa AlMashhadani, Specialist Senior Registrar Dental Public Health specialist, Dubai Health Authority, United Arab Emirates, Tel: 00971551038706, E-mail: ssalmashhadani@dha.gov.ae
Citation
AlMesmar H, Saleh N, AlMashhadani S and Farghali K. The detection of pre-diabetic patients in the dental setting (2019) Dental Res Manag 3: 56-63
Keywords
Oral health, Pre-Diabetes, Diabetic, FINDRISC, HbA1c, Periodontal, Screening, Oral-Systemic.
