
 PDF
PDF
Introduction
Ideal health is the ultimate goal of mankind throughout all ages. Proper nutrition contributes in expression of proper genetic heritage. Consequently, severity of age related degenerative disease might be influenced by nutrition. As the age advances several medical problems and diseases occurs, which have an underlying cause as nutritional aspects and along with that patients socioeconomic status and the dietary habits have a profound influence on their dietary selection [1]. Hence, a dental professional must also be aware of these potential detrimental effects of dental treatment and provide counteractive dietary guidance. The aim of this review is to summarize the earlier investigations on the association between food intake and dental status in geriatric patients [2].
Review of the Literature
Oral health is a prerequisite for a good chewing function, which may have an impact on food choice and nutritional well-being [3]. A variety of oral conditions can lead to an inadequate nutritional status, including tooth loss, pain and discomfort associated with caries, periodontal disease and ill-fitted dentures [4]. The absence of teeth in particular can affect the digestive capacity and nutritional status of the individual. Furthermore, the selection of food can be impaired due to the reduced masticatory capacity of the individual, leading to a restricted intake of fiber and protein-containing foods [5]. The presence of natural teeth and well-fit dentures has been linked to an increased variety of foods and nutrient intake, which will contribute to the consumption of a diet rich in fiber [6]. Maintaining an adequate nutritional status is important because an inadequate health status can lead to either underweight, which increases the risk of infections and mortality [7].
Healthy teeth are essential for effective chewing and swallowing and therefore for good nutrition intake. The relationship between oral health and nutritional health in the elderly is complex and controversial, and current understanding of it is limited [8]. Nutritional status also acts as a determination factor for physical performance with aging [9,10]. Nutritional status has been reported to deteriorate with aging, partly due to the loss of muscle mass and declined food intake [11]. Food avoidance and food modification are two self-management strategies [12]. Those who have impaired oral health may avoid foods that are difficult to eat or modify the ways that foods are prepared or eaten. Each can serve a different purpose. Without regard for the impact on the nutritional quality of the diet, avoidance can minimize the effects of chewing difficulties and tooth pain, and other oral health problems [13]. Modifying foods may serve to maintain certain foods in the diet that one perceives as beneficial or pleasant, and overcome difficulties with the inability to chew food properly [16].
The aim of this study is to evaluate the relationship between oral health status and nutritional status of non-institutionalized elderly individuals. The effect of aging on the oral health status, the effect of the oral health status on nutritional intake and the correlation of oral health status and malnutrition in the elderly will be evaluated. We hypothesize that there is a correlation between the oral status and the nutritional intake in elderly people (Figure 1).
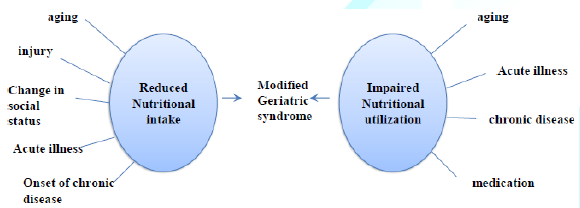
Figure 1: A frame work of the review of literature.
Materials and Method
This is a Cross sectional research of geriatric outpatients who visited RAKCODS Dental Clinic. The duration of this research was six months. The study plan had been approved by the Ethics Committee of the University (RAK.REC.REF 24-2016-UG).
Patients Groups: 40 geriatric patients (20 males and 20 females) were participated in this research. All the participants were signed on Consent form (Questionnaire Provided as Supplementary). For illiterate or low-reading level subjects, consent was obtained through their legal representatives. Excluded from the study were those individuals that were not in good enough physical and/or mental condition to participate in the collection of data, for example: those confined to wheelchairs, amputees, or those with problems of understanding that would prevent the measurements used in the study from being taken. The sample was divided into two groups, the Young Senior Group (YSG), with age not exceeding 70 years, and the Elderly Senior Group (ESG), aged over 70 years.
The cut-off point for the definition of elderly recommended by the World Health Organization (WHO) (1989).
The Data collecting procedure will be in the following process:
· History taking,
· Questionnaires, to collect information on socioeconomic status, eating habits, physical activity and health habits,
· Clinical examination and radiographic analysis. The oral health status was assessed using the index for Decayed, Missing and Filled Teeth (DMFT). The evaluation of oral health status included the identification of decayed, missing, and filled teeth, and the presence of prostheses. The oral examination was conducted in daylight according to biosecurity standards and the findings reported in an odontogram as recommended by the WHO (1997).
The data were analyzed using chi test statistics to assess the different factors affecting the oral status of the participated groups. For comparison and analysis of results the cut-off values used were those obtained from the Oral Health Survey of 2003 for the elderly age group (65 to 74 years) carried out in the Southeast region of Brazil. The mean DMFT for this region was 28.61 ± 6.44 which meant that dental health was satisfactory, this being defined when DMFT ≤ 22.17, with dental health status considered poor when DMFT>22.17. By transforming the DMFT index in Decayed (D), Missing (M) and Filled (F) the cut-off point was the average found in the Southeast where oral health status had satisfactory values of D>0.60, M>27.05 and F=0.91, and oral health status was poor with D>0.60, M>27.05 and F>0.91.
The Kappa test was used to lend a greater reliability to the data collected, and the value of k was =0.9129, with a p-value below 0.01%. The importance of this test is that it shows that the value of K was significantly different from zero and this association is classified as excellent. Other data on the oral health status were obtained with direct questions about intake of types of food and perception of the quality of dental prostheses.
The data obtained were presented in descriptive form as mean, standard deviation and percentage. For comparison of continuous variables between the two groups, we used Students t-test for independent samples or the Mann-Whitney test. To examine the correlations between continuous variables we used Pearsons correlation test or Spearmans. For the correlations between variables, we used Fischers exact test.
Results
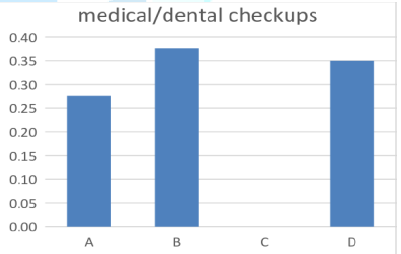
Figure 2: Results according to the medical and dental checkups.
The question was Do you maintain regular visits with your physician and dentist?
A. Yes, I maintain regular visits with my physician and dentist.
B. No, I only maintain regular visit with my physician.
C. No, I only maintain regular visit with my dentist.
D. No, I dont maintain regular visit with either.
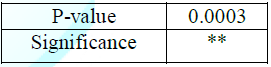
70% from the patients have chooses answer B (0.38%) and D (0.35%) but the significance is in answer C to not able to maintain regular visits with the dentist (0.50%). So, P-value was C significant answers (0.0003) (Figure 2 and Table 1).
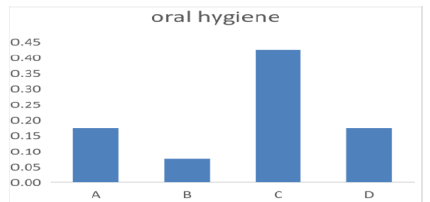
Figure 3: Results according to oral hygiene.

The question was Do you brush and floss your teeth or use mouth wash?
A. Yes, I brush and floss daily and use mouth wash.
B. Yes, I brush my teeth and floss but i dont use mouthwash.
C. Yes, I only brush my teeth but not daily.
D. No, I dont do anything to my teeth.
Majority answered C (0.47%), and according to the oral hygiene scale majority had fair scale (P-Value 0.0008) (Figure 3 and Table 2).
They increase in prevalence of cardiovascular disease and endocrine disease, out of 40 samples 19% had endocrine and 14% had cardiovascular conditions. There is a minor significant in neurological disease and its prevalence in geriatric population, only 2% of the population had neurologic conditions (Figure 4 and Table 3).
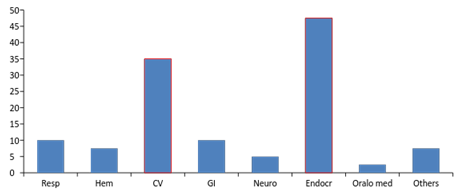
Figure 4: Results according to systemic disease.

Table 3: P-value of the significances according to the systemic disease.
Majority of samples had missing teeth and tooth decay regardless of gender, while none of the samples had any tooth aches which showed a significance, and minor significance in patients with grinding teeth habit and tooth ulcer (Figure 5 and Table 4).
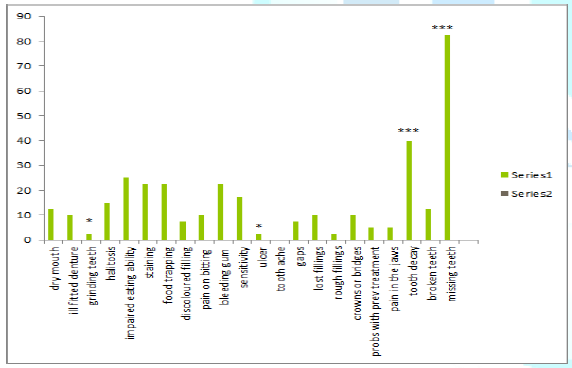
Figure 5: Results according to oral diseases.

Table 4: P-value of the significances according to the oral conditions.
There is increase in prevalence and significance with patients taking galvax and metformin and aspirin in the geriatric population (Figure 6 and Table 5).
According to the graph (no significance has been found) (Figure 7). 97.5% of the geriatric sample includes carbohydrates and caffeine and dairy and protein in their diet, nevertheless 52% include sugar and 75% include sodium in their diet, which reveals change in diet according to the systemic diseases.
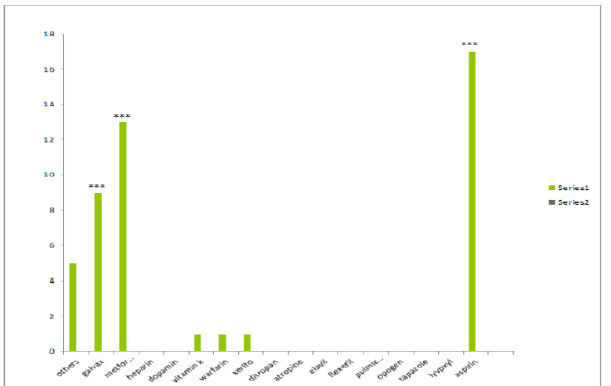
Figure 6: Results according to the choice of medications.
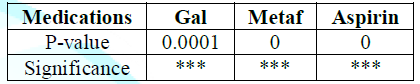
Table 5: P-value of significance according to the medications.
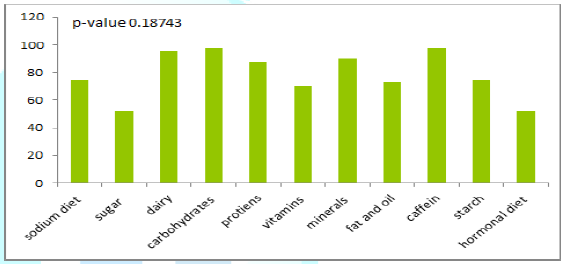
Figure 7: Results according to diet selection.
Discussion
The purpose of this study is to determine if there are associations between nutritional intake and the oral health status in geriatric population. There is an abundant scientific evidence to support the involvement of oral health in general health. Some authors have described the role of oral health is in nutrition, and indirectly in the control of different acute and chronic diseases. In the present study, we found that changes in diet can influence the oral health and vice versa. Reflecting in the nutritional status of the individual Review of the study has shown that patients who have marked loss of teeth may be prone to a decrease in the intake of foods with a heavy consistency, which are a major source of vitamins, minerals, fiber and protein. However, it is important to note that there are several factors other than oral health status that influence food choice, such as personal preferences, available food sources and dietary habits, as well as psychosocial and economic factors [2].
From a theoretical viewpoint, given that oral health is a modifiable risk factor, its improvement would reduce the risk of mastication and swallowing problems and the nutritional deficiencies they can cause. Deficient mastication is related to tooth loss, a lack of saliva, mastication force, and malocclusion problems. Some local studies have indicated that individuals with mastication problems avoid fresh fruits and vegetables, well-done meat, and even bread, preferring soft, easily chewable food that can often raise sugar and fat consumption to levels above recommendations, increasing their risk of cardiovascular diseases and metabolic syndrome. Masticatory function in elderly depends on two major factors, which are the number of natural antagonist teeth and the quantity and quality of saliva. Subsequent potential nutritional consequences are generally considered according to two different viewpoints. The first viewpoint considers a healthy oral aging taking place without any important oral disorders such as tooth loss or critical saliva deficiency. For this segment of population, aging is associated with a decrease in maximal bite force and changes in Masticatory muscle tissue. However, these alterations have little impact on Masticatory performance as these persons still produce a food bolus suitable for swallowing and only minor adaptations are needed to compensate the physiological changes.
The second viewpoint considers the impact of oral functioning on digestion or nutritional status in the elderly. In addition, denture wearers fail to adapt to changes in food texture such as hardness. A recent review of the evidence for nutritional exposures in the etiology of periodontitis suggests that, in some cases, inadequate levels of vitamin D and calcium may contribute to periodontal disease and that nutritional intervention may be of some benefit [15]. According to this survey it has shown that majority add dairy and protein in their diet which showed uncommon periodontal disease in the sample taken.
In a recent study, severe tooth loss in older adults was found to be a key indicator of a compromised dietary quality [16]. And an impaired oral health often leads elderly to modify their diet to adjust it to their limited oral functional capacities. These changes are mostly not adequate to maintain good overall health since soft foods are often foods rich in fat and contain additives [17].
Conclusions
In summary, the oral health status of the geriatric population is generally deficient, with an elevated prevalence of caries, periodontal disease, and tooth loss. These are responsible for mastication difficulties, chronic disease destabilization, and impairment of oral quality of life, with direct effects on the individuals general quality of life and well-being. Surveillance and improvement of the oral health of the elderly should be a key objective of the multidisciplinary team responsible for their care, including dentists, dental hygienists, geriatricians, and caregivers.
According to the systemic disease patients regardless of age group and gender showed that majority had cardiovascular and endocrine diseases which lead them to use medications such as galvex and metformin and aspirin and eventually change their diet accordingly, by reducing their sugar and sodium intake. The major significant oral conditions in this study were missing teeth and decayed teeth while minor significance showed in tooth ache and ulcer in the geriatric population.
Increase carbohydrate intake nevertheless decrease in sugar and sodium intake in their diet specifically showed unhealthy diet selection in regards of their limitation in diet selection, which as mentioned earlier choice of diet preference may be because of several factors such as socio economic status and educational factors. According to the number of elderly participants in this pilot study, it may be concluded that the DMFT index was satisfactory in 60.7% of the patients. Tooth loss was the biggest concern of the elderly in accordance with the high percentage of ill-fitting dentures (45.5%) and prostheses that make it difficult to chew (51.5%).
Recommendations
The main recommendation is to modify the consistency of the diet, eliminating certain foods and reducing the possibility of nutritional defects. Balanced diet as nutritional recommendations for Oral Healthcare team as the general assessment that tooth loss in elderly people who need nursing care is likely to have a larger impact on nutrition than that in healthy elderly people
References
1. Gil-Montoya JA, Ferreira de Mello AL, Barrios R, Gonzalez-Moles MA and Bravo M. Oral health in the elderly patient and its impact on general well-being: a nonsystematic review (2015) Clin Interv Aging 10: 461-467. https://doi.org/10.2147/cia.s54630
2. Rodrigues Junior HL, Scelza MFZ, Boaventura GT, Custódio SM, Moreira EAM, et al. Relation between oral health and nutritional condition in the elderly (2012) J Appl Oral Sci 20: 38-44.
https://doi.org/10.1590/s1678-77572012000100008
3. Rauen MS, Moreira EA, Calvo MC and Lobo AS. Oral condition and its relationship to nutritional status in the institutionalized elderly population (2006) J Am Diet Assoc 106: 1112-1114. https://doi.org/10.1016/j.jada.2006.04.015
4. Touger-Decker R and Mobley CC. Position of the American Dietetic Association: oral health and nutrition (2007) J Am Diet Assoc 107: 1418-1428. https://doi.org/10.1016/j.jada.2007.06.003
5. Sheiham A and Steele J. Does the condition of the mouth and teeth affect the ability to eat certain foods, nutrient and dietary intake and nutritional status amongst older people (2001) Public Health Nutr 4: 797-803. https://doi.org/10.1079/phn2000116
6. Marshall TA, Warren JJ, Hand JS, Xie XJ and Stumbo PJ. Oral health, nutrient intake and dietary quality in the very old (2002) J Am Dent Assoc 133: 1369-1379.
https://doi.org/10.14219/jada.archive.2002.0052
7. World Health Organisation (1995) Tech Rep Ser 854:1-452.
8. Muirhead VE, Marcenes W and Wright D. Do health provider-patient relationships matter? Exploring dentist-patient relationships and oral health-related quality of life in older people (2014) Age Ageing 43: 399-405. https://doi.org/10.1093/ageing/aft183
9. Alipanah N, Varadhan R, Sun K, Ferrucci L, Fried LP, et al. Low serum carotenoids are associated with a decline in walking speed in older women (2009) J Nutr Health Aging 13: 170-175. https://doi.org/10.1007/s12603-009-0053-6
10. Houston DK, Stevens J, Cai J and Haines PS. Dairy, fruit, and vegetable intakes and functional limitations and disability in a biracial cohort: the Atherosclerosis Risk in Communities Study (2005) Am J Clin Nutr 81: 515-522.
https://doi.org/10.1093/ajcn.81.2.515
11. Volkert D. Malnutrition in the elderly-prevalence, causes, and corrective strategies (2002) Clin Nutr 21: 110-112. https://doi.org/10.1016/s0261-5614(02)80014-0
12. Quandt SA, Chen H, Bell RA, Savoca MR, Anderson AM, et al. Food avoidance and food modification practices of older rural adults: association with oral health status and implications for service provision (2010) Gerontologist 50: 100-111.
13. Chavers LS, Gilbert GH and Shelton BJ. Two-year incidence of oral disadvantage, a measure of oral health-related quality of life (2003) Community Dent Oral Epidemiol 31: 21-29. https://doi.org/10.1034/j.1600-0528.2003.00031.x
14. Anastassiadou V and Heath MR. Food choices and eating difficulty among elderly edentate patients in Greece (2002) Gerodontology 19: 17-24. https://doi.org/10.1111/j.1741-2358.2002.00017.x
15. Van der Velden U, Kuzmanova D and Chapple ILC. Micro nutritional approaches to periodontal therapy (2011) J Clin Periodontal 38: 142-158.
https://doi.org/10.1111/j.1600-051x.2010.01663.x
16. Savoca MR, Arcury TA, Leng X, Chen H, Bell RA, et al. Severe tooth loss in older adults as a key indicator of compromised dietary quality (2010) Public Health Nutr 13: 466-474. https://doi.org/10.1017/s1368980009991236
17. Rémond D, Shahar DR, Gille D, Paula P, Kachal J, et al. Understanding the gastrointestinal tract of the elderly to develop dietary solutions that prevent malnutrition (2015) Oncotarget 6: 13858-13898. https://doi.org/10.18632/oncotarget.4030
*Corresponding author
Hala Zakaria, Associate Professor, RAK College of Dental Sciences, RAK Medical and Health Sciences University, United Arab Emirates, E-mail: hala.zakaria@rakmhsu.ac.ae
Citation
Zakaria H, Duarte C, Falah H and Abdulwahab M. Assessment of correlation between nutrition and oral status of elderly (2020) Dental Res Manag 4: 4-7.
Keywords
Diet, Geriatrics, Nutritional analysis, Dental status may influence food intake.
