
 PDF
PDF
Background
Aspirin was once the mainstay of stroke prevention in atrial fibrillation. However, the development of Vitamin K Antagonists (VKAs) and the evolution and availability of Direct Oral Anticoagulants (DOACs), has left aspirin (ASA) therapy by the wayside, based on the results of the BAFTA, ARISTOTLE, RE-LY and ROCKET-AF trials. Both ASA as monotherapy and ASA as dual-antiplatelet therapy are no longer recommended as first line stroke prevention in patients with CHA2DS2-VASc ≥ 2 [1,2]. Exceptions in the guidelines exist only in certain clinical settings, particularly in those with CHA2DS2-VASc score=1 [3]. Besides primary outcomes, including endpoints such as cardiovascular death and mortality, VKAs have additionally shown no increased risk of bleeding compared to ASA, especially among the moderate to high-risk sub-group of atrial fibrillation patients [4,5,6-9].
Regarding ASA use for cardiovascular benefit, ASA is ineffective at increasing disability-free survival or at decreasing mortality among healthy elderly adults without clear risk factors [10,11]. This calls into question the popular assumption that the benefits of ASA therapy for cardiovascular health of the general population outweigh negative side effects. Therefore, ASA use overall should be carefully assessed, particularly in patients with atrial fibrillation.
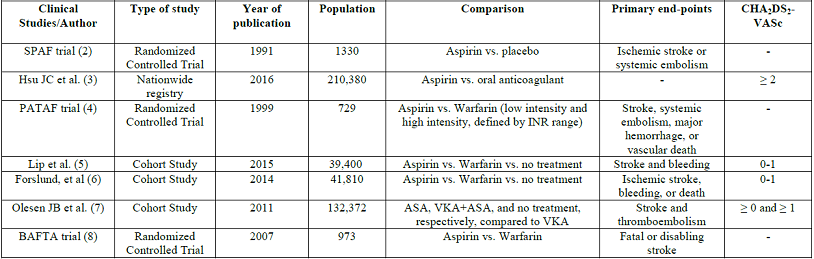
Interestingly, even more than a decade after the first generation of studies showing superiority of VKAs for stroke prevention in atrial fibrillation, ASA continues to be prescribed to patients with CHADS2 scores of greater than or equal to 2 despite overwhelming evidence against, based on the results of the PINNACLE trial, which involved 210,380 patients with high CHADS2 scores [12]. In fact, in 2012 the European Society of Cardiology recommended ASA for patients who refused anticoagulation, consistent with evidence at the time that ASA did have benefit over no therapy for this patient population [13]. Regarding specifically lower risk patients, the 2014 American College of Cardiology/American Heart Association guidelines recommend no antithrombotic therapy or treatment with an oral anticoagulant or aspirin for non-valvular atrial fibrillation with CHA2DS2-VASc=1 [2]. With a spotlight on ASA this year in the literature, it is appropriate to re-evaluate ASA as alternative therapy to VKA or DOAC for patients with atrial fibrillation. Specifically, evidence should be evaluated behind the benefit of ASA vs VKA or DOAC vs no therapy for patients with non-valvular atrial fibrillation and CHA2DS2-VASc=0 or 1 (Table 1).
The Evidence
The evidence for ASA for stroke prevention in patients with atrial fibrillation with low risk of stroke (CHADSVASC<2) stems from the Stroke Prevention in Atrial Fibrillation (SPAF) trial, published in 1991, which followed patients for a mean of 1.3 years and found a 42% reduction in ischemic stroke and embolism, as well as decreased mortality, with ASA compared to placebo. Nevertheless, the SPAF trial also looked at warfarin outcomes and found that warfarin had a superior reduction of primary events or death compared to aspirin, 58% (p=0.01) vs. 32% (p=0.02). The risk of significant bleeding was 1.5% vs. 1.4%, respectively [2]. Based on this early study, ASA appeared to be a safe and effective (albeit less so) alternative to VKAs.
Nevertheless, this study was performed in an era where CHADSVASC had not been described before, and generalization among different thrombotic risks and lack of standardized criteria was evident. Even though the SPAF trial gave a hope for aspirin, evidence has been slowly proving it differently. In 2000, the Primary Prevention of Arterial Thromboembolism in Nonrheumatic Atrial Fibrillation (PATAF) trial supported the popular opinion that ASA was an accessible and inexpensive therapy for those at low risk of stroke or embolism, with a decreased risk of bleeding compared to anticoagulation and a low drug-interaction profile. It should be noted, however, that the PATAF trial was a relatively small study of a uniform, elderly population in the Netherlands [14].
More recently, a meta-analysis published in 2007 supported these early
findings. Hart et al. concluded that ASA did reduce risk of stroke and embolism in
patients with atrial fibrillation by 20% compared to placebo, in addition to a
similar decrease in mortality. Nonetheless, warfarin was found to reduce stroke
by 60%. Of note, this meta-analysis included patients with both low and high CHA2DS2-VASc
values. Sub-group analysis was not performed, so conclusions for low vs high CHA2DS2-VASc
values were not assessed. Most studies included in this meta-analysis
specifically targeted primary prevention [15]. In 2011, a large study in
Denmark performed sub-group analyses of VKA vs ASA vs placebo by CHADS2
and CHA2DS2-VASc scores. The results showed no net
clinical benefit of ASA in patients with a low risk of stroke or embolism
(CHADS ≥ 0 or CHA2DS2-VASc ≥ 1).
This study also found that ASA did not decrease risk of bleeding compared to warfarin. Specifically, this study supported a neutral or positive net clinical effect of warfarin over ASA in low risk patients with atrial fibrillation, which contradicts the prior assumption that as risk decreased, the efficacy of ASA increased enough to become clinically indicated [16]. This study was the cornerstone for developing the most recent studies that advocate for anticoagulation over antiplatelet in CHA2DS2-VASc ≥ 1. Numerous other studies throughout the last several decades also support either similar bleeding risk or insignificant difference in bleeding risk between ASA and VKA or between ASA and DOACs [4,5,6-8].
A Swedish study in 2014 also evaluated the risk of stroke or embolism in atrial fibrillation. Their findings were consistent with a low support of ASA in low risk patients, finding that patients with CHA2DS2-VASc scores of 0-1 had a 1.0-1.2% one-year risk of ischemic stroke with ASA therapy compared to a 0.1-0.2% risk without any treatment, which suggests that ASA likely has no clinical benefit compared to no therapy for patients with low risk of stroke or embolism [17]. It should be noted that both the aforementioned Danish and this Swedish study were regional studies with presumably homogenous populations, thus lacking external validity in other populations and ethnicities.
A recent study published in 2015 by Lip, et al. compared ASA to warfarin therapy for primary prevention of stroke or embolism in those with CHA2DS2-VASc scores of 0 or 1 [18]. They included a total of 39,400 patients, of which 10,475 were treated with VKAs; 5,353 were treated with ASA; and 23,572 were left untreated. Primary endpoints, including stroke, bleeding and death, were evaluated by both an intention-to-treat and Continuous Treatment analyses. The authors found that for those with a low risk of stroke or embolism, defined as CHA2DS2-VASc=0 for males and CHA2DS2-VASc=1 for females, the risk of stroke, bleeding, and death was truly low, and there was therefore no net clinical benefit of treatment with either VKA or ASA.
In those with one additional risk factor (CHA2DS2-VASc=1 for male and CHA2DS2-VASc=2 for female), ASA did not significantly reduce risk of stroke and was significantly associated with increased risk for bleeding, i.e., regardless of sex, ASA therapy does not prevent stroke in those with CHA2DS2-VASc=1, and furthermore does not prevent stroke in women with CHA2DS2-VASc=2. However, in untreated patients with one additional risk factor (CHA2DS2-VASc=1 for male and CHA2DS2-VASc=2 for female), 1-year stroke risk increased by 3.01-fold, bleeding by 2.35-fold and death by 3.12-fold. The authors also found that for those with one additional risk factor (CHA2DS2-VASc=1 for male and CHA2DS2-VASc=2 for female), there were reductions in stroke and death with VKAs compared to no treatment and with VKAs compared to ASA, without a significant increase in bleeding with VKA vs ASA [18] .
Conclusion
In the last three decades, ASA therapy has repeatedly been found to be inferior to anticoagulation for preventing stroke in patients with non-valvular atrial fibrillation, even for those with low risk of embolism or stroke (CHA2DS2-VASc ≤ 1). Furthermore, ASA is not associated with decreased risk of bleeding compared to VKA. The net benefit of ASA therapy for these patients, therefore, does not have supporting evidence, and we conclude that patients with low CHA2DS2-VASc should not be offered ASA as a safer alternative to anticoagulation. Reasons to prescribe ASA in this patient population include availability, financial accessibility, and convenience, but these values are counterbalanced by similar bleeding risk to VKA and significantly decreased efficacy at preventing the primary outcome.
References
1. Ruff CT, Giugliano RP, Braunwald E, Hoffman BE, Deenadayalu N, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: A meta-analysis of randomised trials (2014) The Lancet 383: 955-962. https://doi.org/10.1016/S0140-6736(13)62343-0
2. January CT, Wann LS, Alpert JS, Calkins H, Cigarroa EJ, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: A report of the american college of cardiology/american heart association task force on practice guidelines and the heart rhythm society (2014) J Am Coll Cardiol 64: e1-e76. https://doi.org/10.1016/j.jacc.2014.03.022
3. Valgimigli M, Bueno H and Byrne RA. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS (2017) Eur J cardio-thoracic sur 53: 34-78. https://doi.org/10.1093/eurheartj/ehx638
4. Stroke prevention in atrial fibrillation study: Final results (1991) Circulation 84: 527-539. https://doi.org/10.1161/01.CIR.84.2.527
5. Mant J, Hobbs FR, Fletcher K, Roalfe A, Fitzmaurice A, et al. Warfarin versus aspirin for stroke prevention in an elderly community population with atrial fibrillation (the birmingham atrial fibrillation treatment of the aged study, BAFTA): A randomised controlled trial (2007) The Lancet 370: 493-503. https://doi.org/10.1016/S0140-6736(07)61233-1
6. Adjusted-dose warfarin versus low-intensity, fixed-dose warfarin plus aspirin for high-risk patients with atrial fibrillation: Stroke prevention in atrial fibrillation III randomised clinical trial (1996) The Lancet 348: 633-638. https://doi.org/10.1016/S0140-6736(96)03487-3
7. Albers GW, Dalen JE, Laupacis A, Manning WJ, Petersen P, et al. Antithrombotic therapy in atrial fibrillation (2001) Chest-Supplements 119: 194S-206S. https://doi.org/10.1378/chest.119.1_suppl.194S
8. Hart RG, Pearce LA and Aguilar MI. Meta-analysis: Antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation (2007) Ann Intern Med 146: 857-867. https://doi.org/10.1016/j.pcad.2015.07.003
9. Potpara TS and Lip GY. Oral anticoagulant therapy in atrial fibrillation patients at high stroke and bleeding risk (2015) Prog Cardiovasc Dis 58: 177-194. https://doi.org/10.1016/j.pcad.2015.07.003
10. McNeil JJ, Woods RL, Nelson MR, Reid CM, Kirpach B, et al. Effect of aspirin on disability-free survival in the healthy elderly (2018) N Engl J Med 379: 1499-1508.
11. McNeil JJ, Nelson MR, Woods RL, Lockery JE, Wolfe R, et al. Effect of aspirin on all-cause mortality in the healthy elderly (2018) N Engl J Med 379: 1519-1528.
12. Hsu JC, Maddox TM, Kennedy K, Katz FD, Marzec NL, et al. Aspirin instead of oral anticoagulant prescription in atrial fibrillation patients at risk for stroke (2016) J Am Coll Cardiol 67: 2913-2923. https://doi.org/10.1016/j.jacc.2016.03.581
13. Camm AJ, Lip GY, De Caterina R, Savelieva I, Atar D, et al. 2012 focused update of the ESC guidelines for the management of atrial fibrillation: An update of the 2010 ESC guidelines for the management of atrial fibrillation developed with the special contribution of the european heart rhythm association (2012) Eur Heart J 33: 2719-2747. https://doi.org/10.1093/eurheartj/eht291
14. Hellemons BS, Langenberg M, Lodder J, Schouten HJA, Van Ree JW, et al. Primary prevention of arterial thromboembolism in non-rheumatic atrial fibrillation in primary care: Randomised controlled trial comparing two intensities of coumarin with aspirin (1999) BMJ 319: 958-964. https://doi.org/10.1136/bmj.319.7215.958
15. Connolly S, Pogue J, Hart R, Pfeffer M, Hohnloser S, et al. Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the atrial fibrillation clopidogrel trial with irbesartan for prevention of vascular events (ACTIVE W): A randomised controlled trial (2006) Lancet 367: 1903-1912. https://doi.org/10.1016/S0140-6736(06)68845-4
16. Olesen JB, Lip GY, Lindhardsen J, Lane AD, Ahlehoff O, et al. Risks of thromboembolism and bleeding with thromboprophylaxis in patients with atrial fibrillation: A net clinical benefit analysis using a real world nationwide cohort study (2011) Thromb Haemost 106: 739-749. https://doi.org/10.1160/TH11-05-0364
17. Forslund T, Wettermark B, Wändell P, von Euler M, Hasselström J, et al. Risks for stroke and bleeding with warfarin or aspirin treatment in patients with atrial fibrillation at different CHA2DS2-VASc scores: Experience from the stockholm region (2014) Eur J Clin Pharmacol 70: 1477-1485. https://doi.org/10.1007/s00228-014-1739-1
18. Lip GY, Skjøth F, Rasmussen LH and Larsen TB. Oral anticoagulation, aspirin, or no therapy in patients with nonvalvular AF with 0 or 1 stroke risk factor based on the CHA2DS2-VASc score (2015) J Am Coll Cardiol 65: 1385-1394. https://doi.org/10.1016/j.jacc.2015.01.044
*Corresponding author:
Juan Simon Rico-Mesa, Department of Medicine, Division of Internal Medicine, University of Texas Health San Antonio, USA, E-mail: mesajs@uthscsa.edu
Citation:
Rico-Mesa SJ, Cornell S and Kanakia R. Current evidence for the use of aspirin in patients with atrial fibrillation and a CHA2DS2-VASc=1 (2019) Clinical Cardiol Cardiovascular Med 3: 7-9.
Keywords
Atrial fibrillation, Anticoagulation therapies, Cardiovascular health.
