Introduction
The kidney is a fundamental organ
required by the body to play out a few imperative capacities including the
support of homeostasis, direction of the extracellular environment, for
example, detoxification, and discharge of dangerous metabolites and medications
(Ferguson et al., 2008). The kidneys are a couple of bean molded organs
situated in the back of the abdomen area. Every kidney is around 4 or 5 inches
long - about the extent of a clench hand (WebMD, 2014).The bean-molded kidneys
have an external arched side and an internal curved side called the renal hilus
.A thin connective tissue called the renal capsule encompasses and keeps up the
kidneys shape and ensures the inward tissues. Inside the renal capsule is the
external layer called the renal cortex, deep to this layer is the renal
medulla. Each pinnacle of the renal pyramid is associated with a minor calyx,
an empty gathering tube for urine (New Health Adviser, 2014).
In people, the kidneys are found
high in the stomach pit, one on every side of the spine, and lie in a
retroperitoneal position at a marginally diagonal point (Boron, 2004). An
ordinary human kidney contains 800,000 to 1.5 million nephrons (Guyton and
Hall, 2006). The kidney is habitually an objective organ for metal harmfulness
since it concentrates huge numbers of these components amid discharge and has
countless procedures which are exceedingly touchy to metal-actuated irritation
(SpingerLink, 2002).
Nephron is the essential
auxiliary and utilitarian unit of the kidney. Its central capacity is to manage
the centralization of water and solvent substances like sodium salts by sifting
the blood, reabsorbing what is required and discharging the rest as urine. A
nephron takes out squanders from the body, directs blood volume and pulse, controls
levels of electrolytes and metabolites, and manages blood pH (Maton et al.,
1993).
Nephrotoxicity is a
kidney-particular toxicity in which discharge does not go easily inferable from
dangerous chemicals or medications (Finn and Porter, 2003). Chemotherapy or
anticancer drug has been of constrained use because of nephrotoxicity (Kohli et
al., 2000). The normal ecological contaminations lead and cadmium are each
known to instigate ceaseless renal sickness and the atomic components of such
poisonous occasions are being illuminated. Nephrotoxicity of these metals is
because of the way that urinary disposal is a primary course of discharge, and
the proximal tubules are particularly delicate because of their high
reabsorptive action. Renal obsessive impacts of these metals shift with the
substance type of the metal, the dosage, and whether the introduction is
intense or unending in nature. The few separated investigations of consolidated
metal exposures show that these neurotic impacts might be changed because of
obscure co-operations of these metals inside the kidney (Madden and Fowler,
2000).
The mammalian kidney is a
fundamentally and practically complex organ that assumes a vital part in
control and direction of homeostasis with different reabsorptive, secretory,
metabolic and endocrine capacities. Inability to play out these capacities is
showed in reabsorptive and secretory imperfections along the nephron, which in
instances of restricted glitches result in a little molecular weight
proteinuria, in more extreme cases display additionally polyuria, glucosuria,
aminoaciduria, phosphaturia, and expanded discharge of electrolytes, and also a
lifted blood urea nitrogen and creatinine, while in most serious structures, a
summed up harm to the kidney capacities shows as the Fanconi disorder (
Bergeron et al., 2000).
Diagnosis
Nephrotoxicity can be analyzed
through a straightforward blood test. Assessment of nephrotoxicity through
blood tests incorporates the estimations of blood urea nitrogen (BUN), grouping
of serum creatinine, glomerular filtration rate and creatinine freedom. In any
case, these appraisals of nephrotoxicity are just conceivable when a lions
share of kidney capacity is harmed (Kirtane et al.,2005).
Biomarkers assign the
biomolecules demonstrating the relationship between exogenous dangerous
substances and maladies. For the most part, biomarkers empower us to decide
early harm to wellbeing created by introduction to exogenous lethal substances,
and give an understanding into the component of the onset of these toxicants to
antagonistically influence certain gatherings or people (Finn and Porter,
2003). The ID of biomarkers that can be resolved from blood or urine came about
because of introduction to a nephrotoxicant is a promising methodology (Shao et
al., 2011). Particularly, urine is viewed as appealing and proficient example
since it is non-intrusive and simple to be gotten in impressive sums (Wu et
al., 2010).
Factors
Various components, for example,
dietary status, associative introduction to a few follow components, nearness
of high-fondness metal-restricting proteins, or other intracellular terminals
for metal sequestration and cell sort are altogether known to assume real parts
in deciding both the nature and degree of metal-or metalloid-instigated
nephrotoxicity (Sabolic, 2006).
Metals
Cadmium and lead are two of the
most common and two of the most nephrotoxic metals known to man (Gonick, 2008).
These are known to be thought by the kidney and to deliver a range of
organelle/biochemical wounds to the nephron by various components (Fowler et
al., 2002).
Cadmium
Exposure
Sources And Absorption: Nephrotoxicity brought about by
cadmium has been depicted in settings of modern presentation and ecological
contamination. Cadmium, a metal customarily got as a by-result of zinc
refining, is utilized modernly in plating of steel, colors, plastics,
compounds, and nickel-cadmium batteries, and in atomic and electronic building
(Friberg, 1984). Since the biologic half-existence of cadmium is long (more
than 30 year), delayed low-level introduction prompts to extreme collection in
specific tissues, particularly the kidney (Gonick ,1978). Absorption of lead
relies upon the physical and substance condition of the metal, and is impacted
by age, physiological status, healthful status and hereditary elements (WHO,
1995). Natural cadmium introduction happens in occupants living in vicinity to
modern contamination (EFSA, 2010). Furthermore in overwhelming smokers (FAO
2011), as tobacco smoke yields high cadmium focuses (IPCS, 2007).
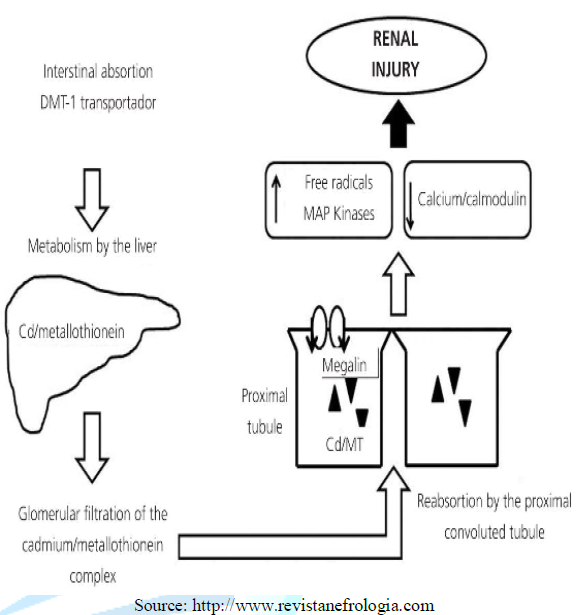
In circulating blood, it binds to
albumin and is transported to the liver, where it binds to glutathione (GSH)
and metallothionein-1 (MT-1). The Cd-MT-1 complex is secreted in bile and subsequently
reabsorbed into the blood by means of enterohepatic circulation. Cd-MT-1 is a
low molecular weight complex (< 7kDa) which is easily filtered by the
glomerulus and is entirely reabsorbed in the S1 segment of the PCT (proximal
convulated tubule) by endocytosis in a process mediated by the proteins megalin
and cubilin (Klassen etal., 2004). The ZIP-8 transporter is also located in PCT
cells, and it is able to transport Cd and other divalent metals through the
apical membrane of these cells; however, the role it plays in Cd toxicity is
unknown (Edward and Prozialeck, 2009). Inside the intracellular medium
of PCT cells, the Cd-MT-1 complex is put away and separated by lysosomes. Free
Cd is then transported to the cytoplasm by lysosomal DMT-1(divalent metal
transporter) (Liu et al., 2001). Activation of protein kinase C builds
articulation of DMT-1, in this manner expanding tubular danger by Cd (Olivi,
2001). Free Cd amasses in mitochondria, obstructing the respiratory chain at
complex III. This outcomes in mitochondrial brokenness and the development of
free radicals, which initiates caspase proteins and the apoptosis procedure.
Free Cd likewise ties to protein sulfhydryl gatherings and influences the
structure and capacity of the proteins. It has been shown that Cd meddles with
enzymatic exercises of the calcium-calmodulin complex, hinders Na+-K+-ATPase
action, and animates movement by MAP (mitogen activated protein) kinases. In
paracellular tight intersections, it influences the dispersion of paracellular
tight intersection proteins and abatements transepithelial resistance (Hirano
et al., 2005). Just 10% of sifted Cd is
reabsorbed into distal finishes of the nephron, and it is conceivable that the
Cd s hypercalciuric impact is the aftereffect of hindrance of calcium direct
action in the distal tubule. (Barbier et al., 2004). Another nephrotoxicity
instrument is the one interceded by the development of against MT antibodies;
introduction to Cd builds MT generation in the liver and kidneys, which
constitutes a defensive reaction to farthest point its lethality. In any case,
once the MTs ability for Cd stockpiling has been surpassed, free Cd can
initiate the arrangement of antibodies against MT, which are likewise lethal to
PCT cells (Klaassen et al., 2009).
To view Figure 1, Click below
Figure 1: Physiopathological mechanisms of cadmium-induced kidney injury DM T-1: divalent metal transporter 1; M T: metallothionein.
Individuals with beginning renal
harm are more helpless to the nephrotoxic impacts of Cd (Hotz et al., 1999). In
patients with diabetic nephropathy, urinary discharge of CD is
straightforwardly identified with expanded urinary discharge of
beta-2-microglobulin and albuminuria (Nordberg et al., 2006). Determining Cd
levels in the bloodstream is used to diagnose acute exposure, whilst urinary
excretion of Cd is used to assess Cd body burden and is useful for evaluating
chronic exposure (Bernard, 2008). Cadmium .because of its long half life, initiates
the amalgamation of a protein called metallothionein by the liver, which goes
about as cadmium scavenger. Low metallothionein levels, press lack, more
established age, female sexual orientation, smoking history, and place of
living arrangement (vicinity to mechanical cadmium sources) are hazard
components for creep mium toxicity (Klassen et al ., 2004). Clinically, cadmium
nephro-poisonous quality presents with elements of proximal tubular brokenness,
for example, glucosuria, ami-noaciduria, and low atomic weight professional
proteinuria. These indications of poisonous quality may happen at much lower
levels of urinary cadmium focuses than those recog-nized as poisonous by the
World Health Organization. Other renal signs incorporate hypercalciuria and
renal stones (Olivi et al., 2001).
Treatment
Treatment for chronic or acute
cadmium nephrotoxicity ought to be preventive. Once there is obvious renal
ailment, the individual ought to be expelled from all further presentation to
cadmium. British against lewisite (BAL) ought not be controlled in light of the
fact that there is confirmation that the cadmium-BAL complex is more poisonous
to the kidney than cadmium alone (Blanusa et al., 2000). At present there is
constrained involvement with the utilization of chelating specialists, for
example, calcium disodium ethylenediaminetetraacetic acid (calcium EDTA), in
treating acute or perpetual cadmium harming in people (Waters et al., 2005).
Lead
Exposure
Sources And Absorption
The primary courses of systemic
introduction are transcendently by means of ingestion or inward breath.
Presentation to inorganic lead happens basically through ingestion of
sustenance and drinking water, despite the fact that introduction by means of
soil and tidy, air, and chippe leaded paint essentially adds to
the general presentation (WHO, 1995). Modern parts that vigorously add to the
arrival of lead incorporate metal mining, coal mining and electrical offices
Non-modern sources are air-borne lead from leaded fuel vapor and toxic paints
(EFSA, 2010). Soil and family tidy are essential wellsprings of lead
introduction for babies and youthful youngsters, because of hand to mouth
exercises (WHO, 2011). Word related presentation to lead
and inorganic lead mixes may happen in an assortment of occupations, including
lead purifying and refining, steel welding or cutting operations, battery
assembling or reusing, radiator repair shops, development and different
occupations including fire binding of lead solder. The US National Institute for
Occupational Safety and Health (NIOSH) recognized more than 100 occupations in
which laborers might be presented to inorganic lead mixes (ATSDR, 2007). Absorption of lead relies on upon
the physical and substance condition of the metal, and is affected by age,
physiological status, nutritious status and hereditary components (WHO, 1995).
Lead in entire blood has a short half-life (35 days).Thus the utilization of
blood lead estimations are confined to observing simultaneous lead
presentation. For appraisal of more remote lead introduction, different
techniques must be utilized (Abudhaise, 1995).
Lead
Induced Nephrotoxicity Mechanism
Pb attached low atomic weight
proteins (<1% of the aggregate) is sifted unreservedly at the glomerulus and
is reabsorbed by PCT cells by endocytosis. Inside the cell, Pb causes
mitochondrial harm, development of free radicals, intracellular consumption of
GSH and apoptosis (Wang et al., 2009). Pb likewise influences enzymatic
responses in which calcium assumes a part, and the calcium-detecting receptor
can likewise be initiated by Pb, which proposes that there might be different
instruments for lead nephrotoxicity (Handlogten et al., 2000)
Pb prompts initiation of
translation atomic element kappa B, enactment of the intrarenal
renin-angiotensin framework and fascination of macrophages, which creates a
fiery procedure in the renal interstitium that might be included in the
improvement of tubulointerstitial harm and high blood pressure (Bravo et al.,
2007 ). In endothelial cells, it has been demonstrated that expanded
development of free radicals instigated by Pb diminishes nitric oxide
generation and the declaration of the protein
guanylate cyclase. These impacts clarify how hypertension can create
accordingly movement of NADP(H) oxidase by expanding generation of hydrogen
superoxide and hydrogen peroxide, in this way influencing oxidative anxiety and
the intracellular redox potential (Bannon et al., 2003).
Nephrotoxicity connected with
lead may have acute and chronic indications. Intense lethality causes
coordinate proximal tubular damage, likely coming about because of
intranuclear, cytoplasmic, and mitochondrial consideration bodies made out of a
lead–protein complex (Moreno et al., 2009). Intense poisonous quality most
normally shows with a Fanconi sort syndrome, including glucosuria,
aminoaciduria, and phosphate squandering, conceivably created by mitochondrial
brokenness. Incessant lead introduction may bring about hypertension, gout, and
interstitial nephritis and fibrosis. The incessant nephrotoxicity of lead
traditionally shows as diminished assessed glomerular filtration rate (eGFR),
with insignificant proteinuria and insipid urine residue. Drawn out exposures,
regardless of the possibility that low level, may bring about CKD (chronic
cadmium disease) by creating interstitial nephritis, hypertension and
hyperuricemia (Lai et al., 2008).

Figure 2: Physiopathological mechanisms of lead-induced kidney injury cGM P: cyclic guanosine monophosphate; NF-κβ: nuclear factor kappa B.
Treatment
Intense lead inebriation without
renal inclusion or lead nephropathy customarily is treated with EDTA chelation.
Inspite of the fact that sodium EDTA has been demonstrated to have dangerous
inclinations as a result of its calcium chelation properties, calcium EDTA in
suitable measurements is helpful and generally innocuous. Progressed renal
ailment identified with lead inebriation (GFR under half of ordinary) must be
dealt with warily, on the grounds that EDTA is sifted by the glomerulus, much
as inulin may be. In such occasions, the measurement and implantation rate of
EDTA ought to be diminished in extent to the serum creatinine height. Lead
nephropathy ought to be dealt with vivaciously, be that as it may, in light of
the fact that treatment may balance out or enhance renal capacity (Gonick,
2008).
Conclusion
Kidneys are the consequential
organs present in our body whose basic function is to filter waste from blood.
Nephrotoxicity by various exogenous substances specially metals like cadmium
and lead are well known because of their common prevalence in surrounding
environment. Both cadmium and lead are the most common nephrotoxic metals which
alter the normal kidney functions and make kidney susceptible to various
abnormalities which can be chronic and acute. Common outcomes of nephrotoxicity
are hypertension, hyperuricemia and decreased glomerular filtration rate. Their
abundant availability in the surrounding environment enhances the chance of
exposure to these metals and accumulation in body tissues. Chelation therapy is
playing role in its treatment but most effective of all the treatments to avoid
or limit exposure to lead and cadmium.
References
1.
Ferguson MA, Vaidya VS and Bonventre
JV. Biomarkers of nephrotoxic acute kidney injury (2008) Toxicology 245:
182-193. https://doi.org/10.1016/j.tox.2007.12.024
2.
WebMD (2014) The kidneys:
structure and function and dysfunction.
3.
New Health Adviser (2014) kidney
structure and function.
4.
Boron WF. Medical Physiology: A
Cellular and Molecular Approach (2004) Elsevier 122-123.
5.
Guyton AC and Hall JE. Textbook
of Medical Physiology (2006) Elsevier Saunders, USA 240-310.
6.
Springer Link (2002) Mechanism of
Metal induced nephrotoxicity.
7.
Maton A, Hopkins J, McLaughlin
WC, Johnson S, Warner QM, et al. Human Biology and Health (1993) Englewood
Cliffs 345-347.
8.
Finn W and Porter G. Urinary
biomarkers and nephrotoxicity Clinical Nephrotoxins (2003) Kluwer Academic
Publishers 621-655. https://doi.org/10.1007/1-4020-2586-6_33
9.
Kohli HS, Bhaskaran MC,
Muthukumar T, Thennarasu K, Sud KJ, et al. Treatment-related acute renal
failure in the elderly: A hospital-based prospective study (2002) Nephrol Dialysis
Transplant 15: 212-217. https://doi.org/10.1093/ndt/15.2.212
10.
Madden EF, Fowler BA. Mechanism
of nephrotoxicity from metal combinations: A review (2000) Drug Chemical
Toxicol 23: 1-2. https://doi.org/10.1081/DCT-100100098
11.
Bergeron M, Goodyear PR, Gougoux
A and Lapointe JY. Pathophysiology of renal hyperaminoacidurias and glucosuria
(2000) The Kidney, Physiology and Pathophysiology 2: 2211-2233.
12.
Kirtane AJ, Leder DM, Waikar SS,
Chertow GM, Ray KK, et al. Serum blood urea nitrogen as an independent marker
of subsequent mortality among patients with acute coronary syndromes and normal
to mildly reduced glomerular filtration rates (2005) J Am College of Cardiol
45: 1781-1786. https://doi.org/10.1016/j.jacc.2005.02.068
13.
Shao C, Li M, Li X, Wei L, Zhu L,
et al. A tool for biomarker discovery in the urinary proteome: A manually
curated human and animal urine protein biomarker database (2011) Molecular Cell
Proteomics 109: 75-79. https://doi.org/10.1074/mcp.M111.010975
14.
Wu Y, Yang L, Su T, Wang C, Liu
G, et al. Pathological significance of a panel of urinary biomarkers in
patients with drug-induced tubulointerstitial nephritis (2010) Clinical J Am
Society Nephrol 5: 1954-1959. https://doi.org/10.2215/CJN.02370310
15.
Sabolic I. Common Mechanism in nephropathy
induced by Toxic Metals (2006) Nephron Physiology 104: 107-114. https://doi.org/10.1159/000095539
16. Gonick
HC. Nephrotoxicity of cadmium and lead (2008) Ind J Medical Res 128: 335-352.
17.
Friberg L. Cadmium and the kidney
(1984) Environment Health Perspective 54: 1-11.
18.
Gonick HC. Trace metals and the
kidney (1978) Miner Electrolyte Metabolism 1: 107-120.
19. International
Programme on Chemical Safety (IPCS), Inorganic lead.Environmental Health
Criteria. World Health Organisation, Geneva, 1995.
20.
EFSA (European Food Safety
Authority) Panel on Contaminants in the Food Chain (CONTAM), Scientific Opinion
on Lead in Food (2010) EFSA J 8: 1570-2010.
21.
Joint FAO/WHO Expert Committee on
Food Additives (JECFA), WHO Food Additives Series: 64. Safety Evaulation of
Certain Food Additives and Contaminants. Prepared by the Seventy-third meeting
of the Joint FAO/WHO Expert Committee on Food Additives (JECFA) 2010.
22.
International Programme on
Chemical Safety (IPCS). Evaluation-Monograph on Lead (2007) Inorganic.
23.
Klassen RB, Crenshaw K, Kozyraki
R, Verroust PJ, Tio L, et al. Megalin mediates renal uptake of heavy metal
methallothionein complexes (2004) Am J Physiol-Renal Physiol 287: 393-403. https://doi.org/10.1152/ajprenal.00233.2003
24.
Edwards JR, Prozialeck. Cadmium
diabetes and chronic kidney disease (2009) Toxicol Appl Pharmacol 238: 289-293.
https://doi.org/10.1016/j.taap.2009.03.007
25.
Liu Y, Liu J and Klaassen CD.
Metallothionein-null and wild type mice show similar cadmium absorption and
tissue distribution following oral cadmium administration (2001) Toxicol Appl
Pharmacol 175: 253-259. https://doi.org/10.1006/taap.2001.9244
26.
Olivi L, Sisk J and Bressler J.
Involvement of DM T1 in uptake of Cd in MDCK cells: role of protein kinase C
(2001) Am J Physiol- Cell Physiol 281. https://doi.org/10.1152/ajpcell.2001.281.3.C793
27.
Hirano S, Sun X, DeGuzman C,
Ransom R, MacLeish K, et al. Signaling mediates cadmium-induced contract ion of
mesangial cells and renal glomeruli (2005) Am J Physiol-Renal Physiol 288:
1133-1143. https://doi.org/10.1152/ajprenal.00210.2004
28.
Barbier O, Jacquillet M, Tauc M,
Poujeol P and Cougnon M. Acute study of interaction among cadmium, calcium, and
zinc transport along the rat nephron in vivo (2004) Am J Physiol-Renal Physiol
287: 1067-1075. https://doi.org/10.1152/ajprenal.00120.2004
29.
Klaassen CD, Liu J and Diwan BA.
Metallothionein protection of cadmium toxicity (2009) Toxicol Appl Pharmacol
238: 215-220. https://dx.doi.org/10.1016%2Fj.taap.2009.03.026
30.
Hotz P, Buchet JP, Bernard A,
Lison D and Lauwerys R. Renal effects of low -level environment al cadmium
exposure: 5-year follow -up of a subcohort from the Cadmibel study (1999) The
Lancet 354: 1508-1513.
31.
Nordberg G, Chen L, Lei L, Jin T
and Nordberg M. Plasma metallothionein antibody, urinary cadmium, and renal
dysfunction in a Chinese type 2 diabetic population (2016) Diabetes Care 29:
2682-2687. https://doi.org/10.2337/dc06-1003
32.
Bernard A. Cadmium and its
adverse effects on human health (2008) Ind J Medical Res 128: 557-564.
33.
Blanusa M, Kostial K, Restek SN,
Piasek M, Jones, MM, et al. Mobilization of cadmium by meso and
racemic-2,3-dimrcaptosuccinic acid (DMSA) in rats (2000) Pharmacol Toxicol 87:
179-181. http://dx.doi.org/10.1034/j.1600-0773.2000.d01-70.x
34. Waters
RS, Bryden NA, Patterson KY, Veillon C and Anderson RA. EDTA chelation effects
on urinary losses of cadmium, calcium, chromium, cobalt, copper, lead,
magnesium, and zinc (2001) Biological Trace Element R 63: 207-221. https://doi.org/10.1385/BTER:83:3:207
35.
World Health Organization (WHO),
Lead in Drinking-water (2011) Background document for development of WHO
Guidelines for Drinking-water Quality.
36.
Agency for Toxic Substances and
Disease Registry (ATSDR), Toxicological Profile for Lead 2007, US Department of
Health and Human Services, Atlanta, US.
37. Abudhaise
BA, Alzoubi MA, Rabi AZ and Alwash RM. Lead exposure in indoor firing ranges:
environmental impact and health risk to the range users (1996) Int J
Occupational Med Environmental Health 9: 323-329.
38.
Wang L, Wang H, Hu M, Cao J and Chen
D. Oxidative stress and apoptotic changes in primary cultures of rat proximal
tubular cells exposed to lead (2009) Archive
Toxicol 83: 417-427. https://doi.org/10.1007/s00204-009-0425-z
39.Handlogten M, Shiraishi N, Awata
H, Huang C and Tyler MR. Extracellular Ca2-sensing receptor is a promiscuous
divalent cat ion sensor that responds to lead (2000) Am J Physiology Renal
Physiology 279: 1083-1091. https://doi.org/10.1152/ajprenal.2000.279.6.F1083
40.
Bravo Y, Quiroz Y, Ferrebuz A and
Vaziri N. Mycophenol at emofetil administration reduces renal inflammation,
oxidative stress and arterial pressure in rats with lead-induced hypertension
(2007) Ame J Physiology Renal Physiology 293: 616-623. https://doi.org/10.1152/ajprenal.00507.2006
41.
Bannon DI, Abounader R, Lees PS
and Bressler JP. Effect of DM T1 knockdown on iron, cadmium, and lead uptake in
Caco-2 cells (2003) Am J Physiol- Cell Physiol 284: 44-50. https://doi.org/10.1152/ajpcell.00184.2002
*Corresponding author:
Hafiza
Samar Fatima, College of Earth and Environmental Science, Punjab University,
Lahore, Pakistan Email: hafizasamar6@gmail.com
Citation:
Fatima
HS. Role of Cadmium and Lead in Nephrotoxicity (2018) Edelweiss Appli Sci Tech 2:
74-78




{kind=link}