
 PDF
PDF
Strengths and Limitations of this study
- Convenient purposive sampling procedures were followed making data collection a bit easier for the research team.
- Scheduling the FGDs to fit nurses’ work schedules, workloads and distance from home was difficult, and although PI and assistant conducted three FGDs, two came out well but the third was disrupted by noise from construction work in a last-minute change of venue, affecting the data quality.
- The nurses also complained about the number of pages to be read, and a lot of distractions from their clients.
- Problems also arose in trying to coordinate focus group
meetings with changes of shift and we also recognized researcher impact on
study participants.
Introduction
Caring for older people is a humbling experience, regarded as unselfish and loving assistance given to another [1]. It is about responsibility and watching over the other and can be carried out by a lay person [2]. Assumptions are that nursing practice focuses on what matters for nurses caring for the elderly, thus listening attentively to what the elderly say about themselves and their lives, gives cues on what is meaningful for them and how their quality of life, peace of mind, body and soul is [3]. The challenges of caring for older individuals can be a scary task for health care providers because it requires multi-specialty expertise with the focus of meeting the individual’s psychological, cultural, spiritualty and physiologic needs [4]. Policies in Western societies have been geared towards enhancing facilities as a home domain for residents through regulation of sheltered accommodation and nursing care facilities for older persons to increase their autonomy [5]. From a caring perspective, there is an emphasis on the staff and the organization respecting the older person’s integrity and personal boundaries, both relational and corporeal [6]. Well-being in older peoples’ everyday life is dependent on respect for their integrity and dignity which is very important [7].
Background
Overview
of Assisted Living Facilities
Demand for home-based care is rapidly increasing as baby
boomers are ageing and advanced medical technologies are extending the life
expectancy of disabled and chronic patients, with an estimate that by 2050,
27million people will need some type of long-term care [8]. The National Home
Health Aide Survey (NHHAS) also estimated that almost 1.46million older people
were receiving care in 2007 and 7.2 million had received care and were
discharged in 2000 [9]. And over 14,000 agencies were in the business of
recruiting and training caregivers for serving clients. Assisted living is any
residential setting not licensed as a nursing home but provides or arranges
personal care and routine nursing in a homelike residential setting [10]. It is
regulated according to its state or region, which also reflects different philosophies
about who should be served in these residential long-term care settings and the
relationship envisaged between assisted living and nursing homes [11]. These facilities
are living arrangements that provide personal care and health services for people
who may need assistance with activities of daily living but wish to live
independently. The level of care provided is not as extensive as that which may
be provided in nursing homes [12]. Assisting living is not an alternative to a
nursing home, but an intermediate level of long-term care. One facility may
look like a modern high-rise apartment building; another might look like a
quiet suburban town home community. Others may resemble a resort hotel or a
country club, but there are some generalizations [13].
The homelike nature of the settings also varies a great deal
among and within state, with some assisted living settings providing
single-occupancy apartments and others providing shared accommodations in
board-and-care settings with two or more persons per room [14]. Apartment-style
assisted living, by design, offers privacy and the opportunity for autonomy. It
also exposes residents to risks of everyday life associated with cooking and
bathing and tends to afford staff less opportunity for protective surveillance.
Whether the service is provided by internal staff, outside home care agencies,
or a combination of these, assisted living tends to be more lightly staffed
than nursing homes [14].
Care
in an Assisted Living Facility
Nurse Practitioners (NPs) provide direct patient care and it
involves cognitive assessment, reviews, ordering and /or reviewing tests and
medication, and liaising with family members [15]. Referrals by NPs include
referrals to geriatricians, to general practitioners, to allied health
professionals (e.g. physiotherapists, dieticians), and to social service (e.g.
home care and dementia support program) [16]. The role of a registered nurse in
the residential aged care facility is multifaceted and includes miscellaneous
forms of caring, managing the individual impact of ageing, the opportunities of
clients and their respective regarding care needs [17].
They are required to provide leadership and guidance in care
directives, which includes training learning and development of other
subordinate staff and team members, and assisting clients make informed
decisions, particularly in relation to treatment choice, palliative pathways
and end-of-life issues [18]. It is also noted that RNs are the clinical leaders
in aged care in effective management of staff retention within their service
[19]. Among the various staff types in a geriatric center are contract staff
and aids including certified nursing assistants, home health aides, personal
care aides or assistants, and medication technicians or aides.
Social workers include licensed social workers, graduates
with a bachelor or master degree in social work in adult day service centers
and residential care communities, and medical social workers [20]. The normal
working hours per day in nursing homes and residential care settings for adult
day services, home health agencies and hospices have been reported as averaging
8 hours per day in three 24-hours section shifts [21], with a
worker-to-caregiver ratio of 3:26 [22]. Nurse practitioners spend considerably
more time with the elderly than do general practitioners attached to these
facilities. They are more accessible, able to initiate more timely care, visit
elderly people in their homes and thereby increase access to care for those who
are not mobile or not able to drive themselves for services [23].
NPs undertake more comprehensive assessments of older
persons than registered nurses; this means that there is better quality of
clinical information to be used by the broader healthcare team in ordering
diagnostic tests or initiating appropriate medicines, and timelier treatment
schedule for acute facility and can circumvent complications of the condition
[23]. From an economic perspective, nurse practitioners in Australian aged care
save dollars for government funders through their timely and accurate care
interventions.
Economic efficiencies were gained through reductions in:
unnecessary transfers to acute health facilities, ambulance costs, hospital bed
days, and thus hospital cost [24].
Health
Care System
In Ghana, most health care is provided by the government and is largely administered by the Ministry of Health and Ghana Health Services. The healthcare system has five levels of providers: health posts or level A, health centers and clinics-level B, district hospitals Level C, regional hospitals or level D and tertiary hospitals Level E. Currently, the country has 170 of health facilities operated by the Ghana Health Service; 71 by missions; 281 by private facilities; and 8 by the Ashanti quasi-government [25]. Apart from allocations from tax revenue, the Ghanaian health system is financed by direct out-of-pocket (OOP) payments (accounting for nearly half of all health care expenditure) and health insurance (composing of premiums and government payroll deductions). These user fees and direct payments disproportionately affect the poor and the aged. The aged support their health care through personal income, family support and National Health Insurance Scheme (NHIS). Family support, Livelihood Empowerment against Poverty (LEAP) grants and rents on property owned by these aged are the major sources of funds available to them [26].
Traditional
Caring System in Ghana
The total population of Ghanaians is 31.1million and that
for the aged is 1.301,000 constituting 4.6% of the total population. The
population of male to female aged is 598,000 to 703,000. Majority of the aged
are household heads or spouse of heads in the households in which they reside
[27]. The aged living accommodation is complex. They live in a dwelling either
owned by them, a household member or rented; but majority are resident in
houses owned by a relative. Ownership of houses is low among the aged,
considering that the aged are expected to have their own houses to command some
respect. Traditionally, aged care is the responsibility of family members and
care is provided within the extended family home, but in recent times, elderly
care is now being provided by the government or charitable organizations. The
reasons for this change include decreasing family size, increasing life
expectancy, increasing number of the aged to the decreasing number of the
dependent family members, the geographical dispersion of these family members,
the tendency for women to be educated and work outside the home [28].
Many elderly people are gradually losing functioning ability
and require additional assistance in their homes. Family members or any person
providing care for the aged are considered to be caregivers, however, in the
Ghanaian formal system caregivers are healthcare providers who are health
professionals such as doctors, nurses who are not nurse practitioners but
registered nurses, and midwives with scientific knowledge about the diagnosis
or treatment of diseases afflicting people and who had worked in the medical
field for at least a year [26]. Ghana has no organization for the aged apart
from facilities for community-based rehabilitation so the study explored how
various stakeholders including nurses would appreciate the establishment and their
willingness to work in assisted living facilities before lobbying government to
establish them.
Aim: The aim of the study is to explore
Ghanaian nurses’ perception on assisted living facilities and their willingness
to work in these facilities.
Materials and Methods
Design
and Setting
A sequential mixed-method study design was employed for the
study. This study is a sub-study of a bigger study that developed a model for
the care of the aged in the Cape Coast metropolitan area; so therefore, a
report from one of the populations used for the bigger study. The researcher
sought to elaborate on or expand on the findings of one method with another.
The study began with a qualitative investigation for exploratory purposes,
followed by a quantitative approach with a large sample so that there could be
generalization of results to the population [29]. Therefore, a focused group
discussion was used to collect data followed by administration of
questionnaires. The questionnaire was designed to answer questions that were
missed during the qualitative phase. The study was carried out in the Cape
Coast Metropolitan Assembly, one of the 17 districts of the Central Region of
south Ghana. This metropolis is further divided into 25 sub-metros for
effective administrative purposes. Of the 25 sub-metros, 10 were randomly
selected using SPSS version 20 software, and an adjoining community was used to
test study instruments. These 10 sub-metros were further classified into three
different zones: urban (elite residential communities), peri-urban (either
urban or rural, but densely populated) and rural (lacking almost all social
amenities).
Subsequently, the zones were demarcated as zones A, B, and C. All the government health facilities in the Central region are in the metropolis. Four health facilities were used for the study, considering one teaching hospital, a metropolitan hospital, a quasi-hospital, and a psychiatric hospital, in which all the categories of nurses are located. Looking at the individual strength of these health facilities, a proportional-to-size approach was used in allocating estimated sampling populations from which participants were recruited. It was concluded by the principal investigator (PI) and research team that the Regional Hospital, which was a referral center for all major and complex cases, would be allocated 40% of the estimated sample size, because of the number of nurses present there.
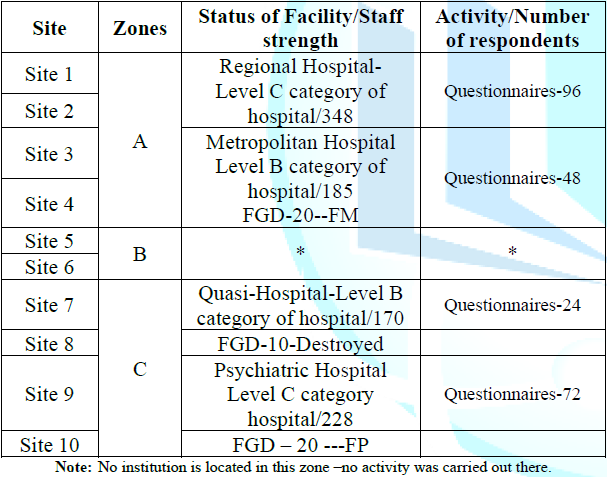
Table 1: Research sites and activities.
This was followed by 30% for the psychiatric hospital which
served the middle belt of the country and one of the three government
psychiatric hospitals in Ghana. The district hospital and the University
hospital, which is a quasi-hospital, followed with 20% and 10% respectively.
Sampling
and Data Collection Techniques
A total of 248 nurses was originally proposed for the study
so 248 questionnaires were sent out, but only 240 questionnaires were collected
because these were the respondents willing to give the needed time and
information due to their busy schedules. Forty participants were recruited to
participate in the three focus group discussions (FGDs). Two groups were made
up of 15 participants each and the 3rd groups were 10 registered nurses. The
inclusion criterion was all categories and ranks of nurses, but excluding
midwives on the grounds that these were in a specialized branch of nursing that
did not have much contact with the aged. All the groups had a combination of
all the category of registered nurses and the discussions ended at a point
where saturation was reached; a point the PI and the assistant were not getting
any new information. Hence, PI in the selection of the study participants did
not consider the ranks of the population in the facilities. The nurses were
selected using convenience sampling technique because of their availability at
the study site. These methods were appropriate because the nurses were very
busy with clients and their residents are scattered in the communities. Getting
them after work was very difficult so the FDGs were held during their duty
shift. The PI and the research assistant collected all the qualitative data. An
unsaturated interview guide was used to conduct discussions.
The four main questions for all the groups were as follows;
(a) what was the welfare of the aged in regard to activities of daily living on
a scale of 0 to 10? (b) How did the aged prepare for their current situation?
(c) Should the government establish assisted living facility? (d) Would nurses
be willing to accept responsibility in caring for the aged in an assisted
living facility? The questionnaire included both structured and semi-structured
questions, which were divided into five sections: Section A -personal information;
Section B-preparedness of the aged for their ageing; Section C-current care
practices looking at activities of daily living; Section D-care that needed to
be added to what the aged currently received: Section E-willingness of nurses to
accept responsibility in caring for the aged in an assisted living facility.
An introductory letter and a gatekeeper from University of
KwaZulu-Natal and the Dodowa Research center was sent to the individual
facility’s research officers and one field worker each was assigned to assist
in data collection. Appointments were scheduled for commencement of data
collection for both the focus group discussions and the questionnaires. The
facility research officers (FROs) sensitized the nurses in preparation for the
focus group discussions and a period of seven days was allocated to organized
participants for the discussions. After each discussion, a week was scheduled
for those who had attended the discussion to meet with other nurses for
responding to the questionnaires so that key informants sent the message to
other parts of the facility through grapevine communication about the impending
data collection.
The age range of target population was 20 to 58 years. Strengths Weaknesses Opportunities Threats (SWOT) analysis was used to explain the reason for the research to participants which was mainly on what assisted living facility was and how it is managed since there was none in Ghana. So, the SWOT analysis was on assisted living, types and how it was funded. Five field workers and a research assistant were recruited, based on their knowledge and experience of the topic under study and were given three days of training. Data collection began in October 2016 and ended in January 2017. Although three FGDs were scheduled, difficulties due to nurses’ workloads and distance of the from the facilities could not allow for 3 but 2 FGDs, the 3rd discussion was marred with a lot of background noise from a construction work near the place the discussion was held so that discussion was discarded followed by the collection of the quantitative data. Each of the discussions lasted between 40 minutes and one hour. A total of 240 questionnaires were completely answered out of 248 giving a 97% of questionnaire return rate.
A quota system was used where each health facility was given
a number of questionnaires to answer through their research officers with the
help of the field workers considering the total population of the facility. Any
nurse met at the data collection point (convenient and purposive sampling) was
included and taken through the questionnaire. Those who were busy were given a
day or two to complete and return the form, with follow-ups from field workers.
Participants and respondents were assured of confidentially and anonymity
before each procedure began by giving them consent forms to sign, and those who
were not ready to be part of the study were given the opportunity to withdraw.
Data
Management and Analysis
The recorded FGDs were transcribed verbatim from the native
language into English by the PI and the trained research assistant. The
transcripts were checked for accuracy and quality and cleaned for anonymity by
the PI. When no discrepancies were identified, the files were coded for
analysis. The methods of analysis were interpretive descriptive analysis to
gain insight into the perception and willingness of nurses to work in caring
for the aged in an assisted living facility [30]. In an initial step, the
content of the data files was read to identify the major distinctive themes
that provided meaningful constructs and illuminated the concept under study.
Three key elements of interpretative descriptive analysis
were followed: detection (which involved identification), assigning the
substantive content and displaying dimensions of the topics under study. Six
major themes and three sub-themes emerged: trends of ageing, preparedness of
the aged for ageing, government plans for the aged, caring and caregivers,
assisted care (sub-themes: cultural ideologies, inception and funding), and
acceptance of responsibility. Quantitative data was analysed alongside and
presented in tabular presentation at the end of the themes that needed
augmentation.
Strengths
and Limitations of this study
- Convenient purposive sampling procedures were followed making data collection a bit easier for the research team.
- Arrangement for the FGDs to fit nurses’ work schedules,
workloads and distance from home was difficult, and although PI and assistant
conducted three FGDs, two came out well but the third was disrupted by noise
from construction work in a last-minute change of venue, affecting the data.
- The nurses also complained about the number of pages to be read, and there were a lot of distractions from their clients.
- Problems also arose in trying to coordinate focus group meetings with changes of shift and we also recognized researcher impact on the study participants.
Results
Participant Characteristics
The nurses showed mixed feelings
about the intent of the study, but were willing to give researchers the needed
information. Of the 40 participants recruited for the 3 FGDs, all had
successfully completed their basic nursing education; six had also completed
their baccalaureate, and four had master degrees. They were all Christians and
married. Three were females and 37 males; ages ranged from 25 to 44 years. Some
had children while others did not. The demographic characteristics from data
collected from the questionnaire blended with the characteristics of those in
the FGDs.
Data collected from the participants
was first edited, coded and analyzed using Statistical Package for Social
Sciences (SPSS) version 20. The editing process was done to check
inconsistencies from participants, whether all items had been responded to and
took care of outliers in the data by removing them from the data set. Data was
analysed and presented in a descriptive presentation of frequencies and cross
tabulation. About 48.8% of eligible respondents in the quantitative study were
in the 20-29 years age group, and just 2.9% were in the 50-59 years age group.
Majority of those who had time for questionnaires were female, single and
Christians. More than half (53.8%) had a diploma qualification as their highest
level of educational attainment, and they were either general or psychiatry
nurses with the rank of staff nurse.
Trends in Ageing
Ageing and death is inevitable, when participants were asked if they had noticed that the population of the aged had increased in their communities, they thought it was due to the aged being pushed into the hospitals because of festive occasions and because community members did not want the aged to be in their way. Some knew about this trend in research reports form dissemination of results to the hospital; others had not because they spent most of their time in the hospitals and scarcely interacted with the community. Another participant agreed that the aged were increasing in number possible because of public health strategies or health promotion activities. All the participants echoed the point made by one contributor that, Yes…we have seen that because the aged are being pushed into the hospitals on festive occasions.
Source: Fieldwork, 2017.
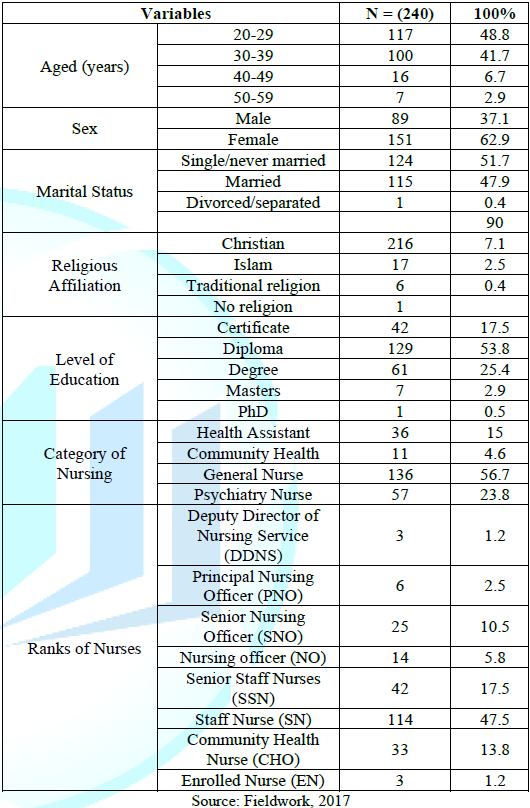
Table 2: Quantitative data on demographic characteristics of nurses.
We the young guys when we invite our
friends to our homes, we do not want them to see our frail parents so we hide
them FM4. From information in a
report disseminated to the hospital, a participant added that we have noticed
that the longevity of Ghanaians has increased through a survey. Ghanaians are
growing older and our population is now between 25-30million FB1. Another participant added that, I
can also say that due to good and proper medical care, the young ones are
growing hence the increment in population FM3.
Table 1-3 shows awareness of the increasing number of aged in our communities.
About 66.6% said ‘Yes’ to the question and 33.4% said ‘No’. The table also
shows the responses on whether the aged were kept in the hospitals on festive
occasions and about 67.9% responded ‘Yes’.
Preparedness for Ageing
When participants were asked how the community planned for their future, they all responded that people planned through ensuring a certain amount of security by taking good care of their children for reciprocation of care in the future. Our society plan through their kids…they try to take care of their kids very well or any family member living with them, so that in their old age they can also rely on them for care. FM6 Others said they knew people who planned by building houses so that they could retire and come back home to their loved ones before dying.
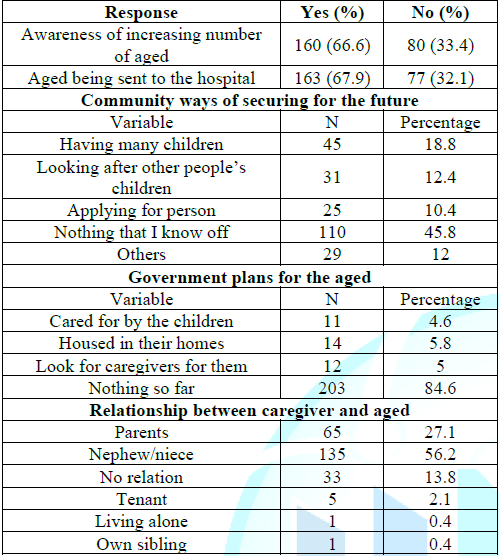
Table 3: Quantitative data on nurses’ awareness of issues of the aged.
Other participants said that those
who plan do it without the knowledge of their family while others do not plan
at all: What I see is, people think of residence, where they will spend the
rest of their lives when they are old…a place to live after pension. Some do it
secretly without their family’s knowledge…others too plan their lives secretly
by saving toward their funeral and buying of caskets FM8. Another participant added that, for those who travel to seek
greener pastures…they make sure they build houses so that when they come back…they
will get a place to stay…because they believe that it is good to die around
your loved ones FM6.
One participant thought only the
educated plan for their future, some of our people invest into businesses so
that when they go home, they can be getting dividend from their investments and
these are the educated ones. Apart from these nothing FM3. Tables 1-3 again shows perceived community ways of securing
the future. 45.8% had no idea how the community members plan for their ageing,
followed by 24.4% who said others look after people’s children so that care
will be reciprocated in future and18.8% said some people have their children as
their future security.
Government Plans for the Aged
Participants were asked what
government does for the aged; they all seemed to know about the national health
insurance scheme (NHIS), the pension scheme, LEAP, and the EBAN because the
programme are ongoing and they had a fair idea of them: the NHIS…it is a policy
that is free for people 65 years and over, they enjoy free premium by the
policy’ FM2, ‘to me this (pension)
plan is limited to the literate i.e. those who have ever had formal classroom
education. It is based on their active years’ contribution they are given
something (money) until they die’; FM4.
Those who had heard of LEAP were not sure how it really worked: ‘they are given
some money (LEAP) especially for the poor to cater for themselves’ FM4; ‘the
only programme l knows of is the LEAP but I do not know how it works; I heard
they go and register for it’ FP1. One
participant thought only the disabled were eligible for the plan and he was
corrected. I thought that programme was for disables FM7.
There was general agreement that
‘the aged have been added’, and one participant commented that, ‘For my area,
the LEAP is only for widows who are old…or who are above 65 years and more but
for the male aged I have not heard anything’, FM6. Another added that he had heard of the EBAN:’ ‘I also have
heard that the aged are given priority whenever they go to the health
facilities for attention or the EBAN for the state owned or metropolitan buses’
FM6. Table 1-3 indicates responses
on government planning for the aged, a majority (84.6%) said that government
had no plan so far; 5.8% said the government plan was for the aged to be housed
in their own homes and 4.6% said the government plan was for aged to be cared
for by children irrespective of the environment.
Caring and Caregivers
When asked if they knew about the
care and caregivers of the aged in their communities; all the participants
agreed that there are some caregivers in their communities, and although these
caregivers think they are doing a great job in caring but care to the nurses
was not good enough. Some suggested that the root of the problem of poor caring
practices was that the extended family system was breaking down and everybody
was now busy, so the aged were left unattended. One participant said he had
often seen old people in the company of young grandchildren about eight years
old looking for directions to destinations and ending up in different parts of
the town.
These was report that; ‘Caring is
not good because we are moving to the nuclear family system that is why we are
facing these challenges. In the nuclear family setting, the aged are left alone
at home so they need more caregivers. But with the extended family system their
children leave their kids with their grandmothers so they tend to enjoy the
interaction of these grandchildren. Meanwhile, in our setting because of our
extended family system there was always someone who is self-employed and ready
to care for the aged’ FP1.
Another participant added that ‘In
our communities, women are more and they suffer the neglect than men so the
government in its own wisdom targeted the women for the LEAP’ FM6. Another described how a friend’s
grandmother was poorly treated by his own mother, People do neglect the aged and
they leave them to their fate … because at their age they are branded as
witches and then neglected. Just yesterday, a friend called me and complained
about how his mother was maltreating his grandma she hardly cooks for her, so
when he questioned the old lady on how she feeds she said she sleeps on empty
stomach when there is no food she eats when there is food and stays when there
is nothing and I think it is very much appalling’ FM2.
Caring is traditionally done by
females in the indigenous African home; participants were quick to add that it was
appropriate for the female child to look after the aged in the community even
through caring could also be done by a male child. Indicative comments were: ‘Caring
is the responsibility of the daughter’ FM4.
‘From where I come from, the aged stays with either the first born or the last
born irrespective of the sex’ FM6. In
my community, it is the responsibility of the last born to care for their aged
but if the aged has a daughter then the daughter will leave wherever she is and
go and care for her parents … she must come and stay by running a routine
between her aged parents and her nuclear family FM3.
Another participant reported that
grandchildren were made to stay with their grandparents and he was an example, I
stay with my grandmother; because of the low educational status of the
community, they do not plan for ageing. What they do is that they rely on their
husbands if they are alive then it is the responsibility of their husbands to
take care of their household and everybody.…So, when there is a girl child in
the family…they will let the girl come and stay with her grandparents and help
with the little things that they may need. When I was home, I did the house
chores because my sister had left for school … but now another girl is there
now’. FM7. Table 3 shows the relationship between caregivers and the aged they
take care off. A majority (56.2%) was close family members of the second
generation, and 13.8% of caregivers were not blood relations of the aged in
their care. One aged person was reported to be living alone and another with a
sibling.
Assisted Living
Assisted living illustrates the
shift from caring as a humanitarian service to a business venture in the
broader health care arena in the 1970s where it has become a consumer-driven
industry that offers a wide range of options, levels of care, and diversity of
services [31]. When asked what they thought about assisted living, participants
asked what kind of nursing care entailed in the assisted living facilities. The
PI took the opportunity to explain the concept of assisted living to them using
the SWOT approach.
As participants deliberated among
themselves and the PI gave them more time to discuss their fears and
uncertainties. There were expressions of disapproval as to why people would want
to give up their cultural role of caring for their own to be replaced by
something, they had no idea off. Other participants felt that government should
assign nurses to take care of the aged in their homes so that they could also
attend to their spiritual needs. Another group was happy because they knew
people who were looking for such places for their aged. There were also
participants who were convinced that day-care would work but felt that there
should first be a suitable policy for the programme before its inception.
Cultural Ideologies
Those who oppose the idea of
assisted living thought that government should come out with a policy on care
for the aged that would be binding on every household in the country. I have my
reservations about this assisted living….You see, a lot of people will be
running away from their responsibilities.….I suggest that there should be a
policy or law before this programme comes off…so that everybody would be made
to take care of their aged … and penalties accorded if those rules are breached
or flouted; …if people neglect their parents, grandparents and it made known to
authorities…these culprits would be punished…people who do not want to look
after their aged could dump them there FM7.
I am not in support with this idea
because when we were young, they took care of us.…We were defecating and
urinating on them and doing all sort of things on them so it is now time for us
to also care for them. Now, that it is time for reciprocation of care we are
trying to dodge our responsibility; leaving it for someone else to do.…As my
brother rightly said people will shed their responsibility to other people.…My
suggestion is if education will be effective on how to take care of the aged. I
think it will be good FM8.
Programme Inception
There were various comments on the
possible inception of the programme by participants: ‘I saw this nursing in a
foreign movie once and it was very fine. Due to our cultural beliefs, the old
ones believe there is a spirit of the environment so they would not like to
leave their environment. But if government too can do that for us it will be
fine. Nurses can take nursing to their door step so that it will be like door
to door nursing care. Caring for the spiritual needs of the aged is also very
important so if they can train nurses, it will be very fine. Every month or
twice a month a nurse can go and visit the aged at home and demonstrate family
involvement in their care’ FM6. ‘Left
to me, government must train more community health officers (CHOs) to handle
the aged just like they are handling the children. The old people also believe
that they are the custodians of the land … so if you ask her to go and stay
somewhere it will not be proper. The uneducated would want their parents to
stay in the house. Meanwhile the young ones cannot say they will not work to look
after their aged parents so the government can train nurses solely for this
programme to go around the homes to help with caring for the aged’ FM5. ‘In Ghana now, we are becoming
enlightened so there should be education for people to be aware of these
innovations.
It should be an in and out of the
facilities and home setting. We must push this thing forward; there will be ups
and downs of the programme while it is taking root. When it takes off…I believe
all these challenges we are bringing up will be taken care off so long as we
pay attention to them’ FP8. ‘The day
care will be proper; our communities have been structured such that every
community in Ghana has a community or social centre so the chief should agree to
let his people to be trained…so that they take off the aged at the community
centre…day-care type will be more feasible.
The day care will work; … it will be
a place where they will have a lot of fun then they come home in the evening. This
will work in Ghana’ FP3. ‘I also
think the church can help…because in my church they are trying to use the
social centre to be doing something creative for the aged. So, that the aged
who can walk will come and play indoor games when they are bored at home then go
back at the end of the day. Some of the tithes we pay at church is used to do
this activity’ FP1.
Funding
Participants offered time to
comments on how the programme should be funded: ‘As part of our pension scheme, we
must be advised so that the same thing to be done on our aged facilities … we
have complaints from the community about people neglecting their aged’ FP5. ‘Government can do it through
private partnership so that it will be regulated like the health insurance
system. This could be one aspect of the health sector, to make life complete’ FP4. ‘Government should go into
partnership with private entrepreneurs so that they can handle this programme
as a business entity’ FP3.
Ehmm! We are being advised to secure
other means of pension plans as workers in our active life: … So, if we are
saying that government should take up responsibility it can also take up that
part of setting up policies to care for the aged. Just like it did for the
3tier system of the existing pension plan so that such funds could easily be
accessed. More so, the emphasis should be on social support. We are worried
about people in the communities complaining on neglecting their aged parents
but I also want to say that anybody who is sensitive enough to identify that
their aged parents need care in such a home or secured services in a home or
looking for someone to cater for their aged is supportive enough Ahhaaa!!! So,
if we should promote this practice rather than undermine it from the scratch,
we could go a long way’ FP8.
As for Ghanaians, we will agree to
pay for the something then we start and just to let it hang… an example is the
mental hospital saga. People will bring their wards with promises … but when
they go home that is all. They do not honor their promises and it becomes a
burden for the government. We do not want such things to repeat itself because
people would be dodging their responsibilities and start blaming the government
when things go wrong, however there should be another way of reaching out to
the aged through government’s point of view. They should be in their own home
environment for government to reach out to them through LEAP’ FM6.
Acceptance of Responsibility
Questions that were missed from the
FGD question guide for participants were captured in the questionnaire for
respondents. Question on willingness to work in an assisted living facility was
captured and answered by 240 respondents. Table 1-4 also displays the response
of respondents to the establishment, and working in an aged-care facility or an
assisted living facility, and willingness to work in an aged care facility or
an assisted living facility. In the analysis, the variable score showed a
statistically significant p-value of 0.043, showing there is an association
between respondents agreeing to the establishment of assisted living and
readiness to work in an assisted living facility. 97.9% agreed to accept
responsibility to work when deployed, while 2.1% were not in favor of the idea.
In the descriptive statistics, there was statistically significance association between having knowledge of government policy and source of this knowledge with a p-value of 0.000. The Table indicated acquisition of information on the policy for the aged and how this information was acquired. A significant number of participants (39.2%) had no idea of any policy on aged care. Even though some claimed to be getting information about the aged, in most cases, from two or more sources. Less than a quarter of the participants said that, ‘Yes’, they knew about this policy from TV and radio.
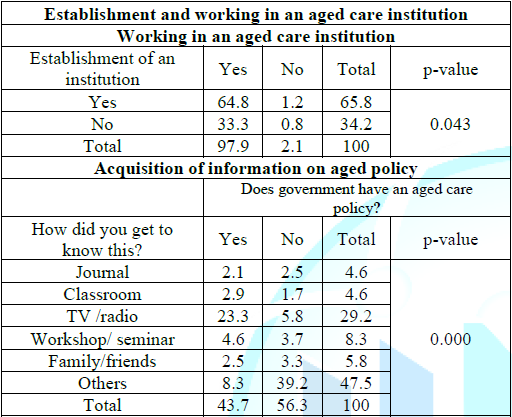
Table 4: Quantitative data on nurses interest in aged issues.
Discussion
This study set out to explore the
perception of establishing and willingness of skilled nurses to work in an aged
care or assisted living facility in Ghana. More than 90% agreed to the
inception of the programme and to accepting responsibility to work in that
environment. Although participants in the focus group were skeptical about
feasibility of the programme, since family members had an obligation to take
care of their own even when resources might be scarce. They nonetheless agreed
that care for the aged was not good, due to the breakdown of the extended
family system and its replacement by nuclear families. The nurses also
acknowledged that health promotion strategies had increased the longevity of
Ghanaians.
Appreciation was expressed for a
documentary on changing family structures, showing that as people live longer
and have fewer children, family structures are transformed, leaving older
people with fewer options for care [32]. Population ageing is a phenomenon that
resulted from declines in fertility as well as increase in longevity: two
trends that are usually associated with social and economic development [33]. Participants
did not know how community members plan for their ageing. Some said that caring
for one’s children and other people’s children was used as a guarantee for the
future in the form of reciprocated care when one becomes frail. According to
Karlberg cited an Akan proverb to illustrate this: “If someone looks after you
to grow your teeth, you must also look after him to lose his” [34]. This system
has been a security for people without children, however, in a modernized
society this system is difficult to maintain. Ultimately the system fails if
these children move away to find work [35]. In a study in central Ghana, found
that growing doubt around family solidarity meant that loyalty being shifted
from lineage to conjugal family, and that the middle-class, urbanized Akan
families had begun to keep non-nuclear relatives at bay, avoiding claims by the
abusua on their income and possessions. Lack of awareness of government plans
could be due to the nurses being fully preoccupied with workplace commitments
than to get involved in community issues or communications on policy
implementation from other sectors.
All respondents knew about the NHIS,
which had a direct bearing on their job descriptions, as suggested by the Abuja
Declaration which called for African heads of state to allocate at least 15% of
annual government budgets to the health sector. In addition, it was expected
that this financial support would increase substantially over the decades [36].
Assisted living will is a new caring practice in the Ghanaian health sector if
accepted in the country, with study participants finding the concept difficult
to understand until it was explained to them. As word got around about the
concept in the course of the sequential data collection in the study, almost
all participants (98%) showed interest in the establishment of aged care
facilities and in working in such facilities or accepting deployment to one by
their employers.
In terms of the technology acceptance model (as applied in the field of information technology and computing), which uses a simplified interpretation of beliefs that affect technology acceptance [37], there are two kinds of belief: perceived ease of use referring to the belief that using a particular system would be free of physical and mental effort, and perceived usefulness. Perceived usefulness is the degree to which an individual believes that using a particular system would enhance his or her job performance. These distinctions had been applied to the adoption of technology in workplaces, including health care facilities [38], in studies focusing on physicians [39], nurses [40], and other clinicians [41] as adopters of the new technology or programme. Similar distinctions may help to explain the dilemma faced by nurses in this study as to ease of use of assisted living facilities, coupled with goal-driven concerns about whether output in their nursing care for the aged will enhance quality of care and improve the status of situation in the community. The concept of funding was rightly suggested as needing to be of the social security type, where the individual contributes to his/her ageing in line with government-controlled policy. It was also agreed by participants that all programme controlled by policies, well managed and sustained.
Conclusion
The purpose of this study was to
explore the perception of establishment and the willingness of nurses to accept
responsibility for working in an assisted living facility in Ghana. Issues that
emerged were the existence of poor caring practices that would favours the
introduction of assisted living, and the importance for study participants of
perceived usefulness of people in the community, but also thought it would be
worthwhile to try the assisted living concept because lives were at stake. There
was also valuable input from respondents about the need for formulated policy
to control the programme and using entrepreneurship to set it going. Study
participants confirmed that there are some individuals in the communities who
have no caregivers, and that for those who do, the care was not what they would
consider adequate.
This suggests that this programme,
through its multidisciplinary approach to nurses, caregivers and clients, may
be meeting needs in the metropolis.
Ethical Approval
The study was approved by the Humanities and Social Sciences Research Ethics Committee of the University of KwaZulu-Natal (HSS/0608/016D) in South Africa and the Dodowa Health Research Centre (IRB Ghana Health Services) of Ghana (DHRCIRB/06/06/16). Voluntary participation was accorded with written and signed consent.
Patient and Public involvement statement: Patients and the public used for
the study were not involved in the conceptualization of the study, its design
and dissemination.
Acknowledgements
I thank the health facilities that granted permission to conduct this research, the research assistant, the field workers and the research officers from the health facilities for their emersed support in data collection. Field work was supported by the bursary from the College of Health Sciences, University of KwaZulu-Natal.
References
1) Eriksson K. Evidence to see or not to see (2010) Nurs Sci Q 23: 275-279. https://doi.org/10.1177/0894318410380271
2) Skogsberg IA and Lindahl B. Empirical studies Personal care assistants’ experiences of caring for people on home mechanical ventilation (2017) Scand J Caring Sci 31: 27-36. https://doi.org/10.1111/scs.12326
3) Bernick L. Caring for Older Adults: Practice Guided by Watson’s Caring-Healing Model (2004) Nursing Science Q 17: 128-134. https://doi.org/10.1177/0894318404263374
4) Goldstein C, Anapolsky E, Park J, Immordino M and Ukoha N. Research Guiding Practice Related to Cultural Issues at End of Life Care (2004) Geriatric Nursing 25: 58-59. https://doi.org/10.1016/j.gerinurse.2003.12.007
5) Clancy A and Mahler M. Nursing staffs’ attentiveness to older adults falling in residential care-an interview study (2016) J Clinical Nursing 25: 1405-1415. https://doi.org/10.1111/jocn.13240
6) Rostgaard T and Szebehely M. Changing policies, changing patterns of care; Danish and Swedish home care at the crossroads (2012) Eur J Ageing 9: 101-109. https://doi.org/10.1007/s10433-011-0209-1
7) Galvin K and Todres L. Caring and Well-Being: A Lifeworld Approach (2013) Routledge, Taylor & Francis Group, London.
8) Department of Health and Human Services. The Future Supply of Long-Term Care Workers in Relations to the Aging Baby Boom Generation: Report to Congress (2003) Washington, DC.
9) Kim K and Antonopoulos R. Unpaid and Paid Care: The Effects of Child Care and Elder Care on the Standard of Living (2011) Levy Economics Institute, USA. https://doi.org/10.2139/ssrn.1946377
10) Department of Health and Human Services. National Study of Assisted Living for the Frail Elderly: Literature Review Update (1996) Lewin-VHI Inc, USA.
11) Mollica RL. State Assisted Living Policy (2000) Portland, ME: National Academy for State Health Policy.
12) Genworth 2014 Cost of Care Survey; Executive Summary (2014) Genworth Financial Inc, USA.
13) https://www.senioradvisor.com/
14) Frytak JR, Kane RA, Finch MD, Kane RL and Griffin MR. Assisted Living and Nursing Facility Outcome Trajectories (2000) HSR: Health Services Research 36:91-111.
15) Bentley M, Minstrell M, Bucher H, Spoule L, Robinson A, et al. Aged care nurse practitioners working in general practice (2015) J clinical nursing 24: 3745-3747. https://doi.org/10.1111/jocn.13066
16) Schadewaldt V, McInnes E, Hiller J and Gardner A. Views and experiences of nurse practitioners and medical practitioners in primary care-an integrative review (2013) BMC family practice 14: 132. https://doi.org/10.1186/1471-2296-14-132
17) Drew D. Experiences of registered nurses as managers and leaders in residential aged care facilities: a systematic review (2011) Int J Evidence-Based Healthcare 4: 388-402. https://doi.org/10.1111/j.1744-1609.2011.00239.x
18) Caruana E. Comprehensive systematic review of evidence on developing and sustaining nursing leadership that fosters a healthy work environment in health care (2008) J Adv Nurs 62: 653-654. https://doi.org/10.1111/j.1365-2648.2008.04667.x
19) Fussell B, McInerney F and Patterson E. Experiences of graduate registered nurses in aged care: a case study (2009) Contemp Nurse 33: 210-223. https://doi.org/10.5172/conu.2009.33.2.210
20) Kojetin HL, Sengupta M, Lee PE and Valverde R. Long-term care services in the United States: 2013 overview (2013) National Center for Health Statistics. Vital Health Stat 3 37:1-107.
21) National Association for Home Care and Hospice, Hospital and Healthcare Compensation Service. Homecare salary and benefits report 2009-2010. In: National Association for Home Care and Hospice, Hospital and Healthcare Compensation Service. Basic statistics about home care.
22) The MetLife national study of adult day services: Providing support to individuals and their family caregivers (2010) MetLife Mature Market Institute.
23) Australian Government Department of Health Ageing and Aged Care. Nurse Practitioner-Aged Care Models of Practice Initiative.
24) Davey R, Clark S, Goss J, Parker R, Hungerford C and Gibson D. National Evaluation of the Nurse Practitioner-Aged Care Models of Practice Initiative: Summary of Findings (2015) Centre for Research and Action in Public Health. UC Health Research Institute, Canberra.
25) Akazili J, Gyapong J and McIntyre D. Who pays for health care in Ghana? (2011) Int J Equity Health. https://doi.org/10.1186/1475-9276-10-26
26) Duah AW, Peprah C and Peprah P. “Let’s talk about money: How do poor older people finance their health care in rural Ghana? A qualitative study (2019) Int J for equity in Health 18. https://doi.org/10.1186/s12939-019-0927-0
27) Duah AW, Peprah C and Peprah P. Factors influencing the use of public and private health care facilities among poor older people in rural Ghana (2019) J Public Health 28:53-63. https://doi.org/10.1007/s10389-018-01010-y.
28) Aboh IK and Ncama BP. Critical Review of the Plight of the Ghanaian Aged (2017) IOSR Journal of Nursing and Health Science 6: 1-4. https://doi.org/10.9790/1959-0602070104
29) Creswell JW. Research Design Qualitative, Quantitative,and Mixed Methods Approaches (2nd Ed) (2003) SAGE Publications.
30) Dwyer T, Creswell A, Rossi D and Holzberger D. Evaluation of an aged care nurse practitioner service: quality of care within residential aged care facility hospital avoidance service (2017) BMC Health Services Research 17. https://doi.org/10.1186/s12913-017-1977-x
31) Lockhart C. Commentary: Is assisted living in the United States well served by regulations requiring the reporting of detailed operational data that are then posted on the Internet? (2009) J Aging and Social Policy 21: 243-245.
https://doi.org/10.1080/08959420902955792
32) Dobriansky PJ, Suzman RM and Hodes RJ. Why Population Aging Matters: A Global Perspective (2007) National Institute on Aging National Institutes of Health U.S. Department of Health and Human services, U.S. Department of State.
33) Population Facts. Population ageing and sustainable development (2015) United Nations Department of Economic and Social Affairs, Population Division.
34) Karlberg T. Elderly People in Ghana” About Roles and Life Situation from their own Perspective (2008) Orebro Theological Seminary, Field Study Course.
35) Geest SDV. Respect and reciprocity: Care of elderly people in rural Ghana (2002) J Cross-Cultural Gerontology 17: 3-31.
36) Carrin G, Doetinchem O, Kirigia J, Mathauer I and Musango L. Social health insurance: how feasible is its expansion in the African region? (2008) Dev ISSues 10
37) Consumer Health Informatics Research resource (CHIRr), Technology Acceptance Model (Perceived Usefulness and Perceived Ease of Use).
38) Holden RJ and Karsh BT. The Technology Acceptance Model: Its past and its future in health care (2010) J Biomedical Informatics 43: 159-172. https://doi.org/10.1016/j.jbi.2009.07.002
39) Paré G, Sicotte C and Jacques H. The effects of creating psychological ownership on physicians’ acceptance of clinical information systems (2006) J American Medical Informatics Association 13: 197-205. https://doi.org/10.1197/jamia.m1930
40) Tung FC, Chang SC and Chou CM. An extension of trust and TAM model with IDT in the adoption of the electronic logistics information system in HIS in the medical industry (2008) Int J Med Inform 77: 324-335. https://doi.org/10.1016/j.ijmedinf.2007.06.006
41) Schaper LK and Pervan GP. ICT and OTs: A model of information and communication technology acceptance and utilization by occupational therapists (2007) Int J medical informatics 76: 212-221. https://doi.org/10.1016/j.ijmedinf.2006.05.028.
Corresponding author
Irene
Korkoi Aboh, School of Nursing and Midwifery, University of Cape Coast, Ghana, E-mail:
iaboh@ucc.edu.gh
Citation
Aboh KI. Perception of nurses on the establishment, and their willingness to work in assisted living facilities in Ghana (2020) Edelweiss Appli Sci Tech 4: 56-64.
Keywords
Aged, Assisted living/care, Care, Nurse and Willingness to work.
