Introduction
In
all these cases was found the limited movement of the right hip. In some
children we found an additional causes connected with the bigger or smaller
disorders in brain. There were children with Minimal Brain
Dysfunctions (MBD)
and they had: a. primary extension
contracture of the trunk, b. anterior
tilt of the pelvis and c. laxity of
the joints.
Biomechanical
etiology
The
cause of etiology of scoliosis was secret over many years [1-41]. In years
1984-2007 was found that the primary cause in etiology of scoliosis-is the
asymmetry of hip movements-limited movements of right hip. In Karski T. [9] was
described a specific model of
hip movements-three
groups of asymmetries-leading to four types of scoliosis. Next important cause
in development of scoliosis is function: gait and standing on the right leg (Figure 1a, Figure 1b and Figure1c). In
figures 2 and 3 is presented the test of adduction and anatomy of shortened
soft tissue (Figure 2, 3).
The
asymmetry of movements of the hips is one of the symptoms of Syndrome of
Contracture (SofC) according to Prof. Hans Mau-Tübingen, Germany (in German Siebenersyndrom)
[18]. Since 2006 we talk in Lublin about the Syndrome of
Contracture and Deformities (SofCD) because we add
the varus deformity of the shanks in newborns and babies as the eighth
deformity.
Figure 1a: Range of adduction of the hips and type
of scoliosis. Causative influence: standing and gait. Deformity S1st
epg.
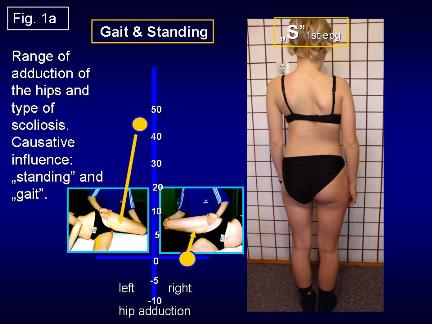
Figure 1b: Range of adduction of the hips and type
of scoliosis. Causative influence: standing. Deformity C 2nd/A epg
and S 2nd/B epg.
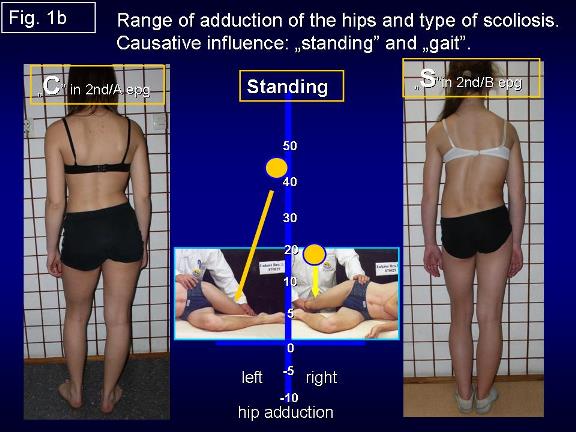
Figure 1c: Range of adduction of the hips and type
of scoliosis. Causative influence: gait. Deformity I 3rd epg.
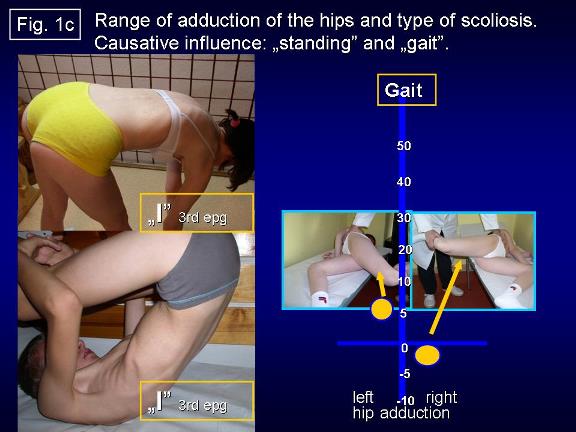
Figure 2: In 2006 was described „the model of hips
movement and type of scoliosis. On the pictures the test to discover the
difference of dduction of hips. Measurement of adduction in straight position
of joints. In this case limited movement of right hip typical for „S scoliosis
in the 1st epg group.
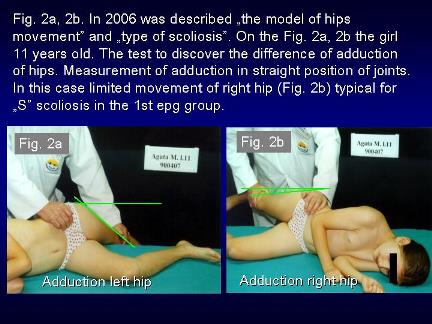
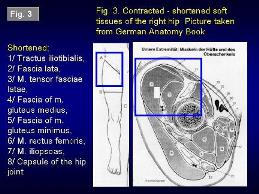
Figure 3: Contracted - shortened soft tissues of
the right hip. Picture taken from German Anatomy Book. Shortened: Tractus
iliotibialis, Fascia lata, M. tensor fasciae latae, Fascia of m. gluteus
medius, Fascia of m. gluteus minimus, M. rectus femoris, M. iliopsoas, Capsule
of the hip joint.
This
varus deformity, in certain conditions-may lead to Blount disease in older
children [18,20-23]. In development of scoliosis the additional secondary
influences can come from Central Nerve System (CNS) in children with MBD and
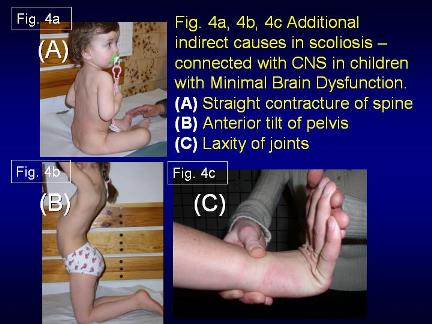
examples are presented in (Figure 4a,
Figure 4b, and Figure 4c).
Classification
Three groups and
four types of scoliosis (Figure 1a, Figure 1b and Figure 1c):
(1)
Scoliosis S 1st Etiopathological
Group (epg)-3D.
Double curve. Stiff spine. Rib hump on the right side of the thorax. Specific
model of hips movements. Connection with gait and permanent standing at ease on
the right leg. Beginning of deformity in 2-3 years of life. Clinical symptoms
appears of the age of 5-6 years.
Figure: 4a-c Additional indirect causes-connected
with CNS in children with MBD. (A) Straight contracture of spine. (B) Anterior
tilt of pelvis. (C) Laxity of joints.
(2a)
Scoliosis C 2nd/A epg-1D or 2D. One curve-lumbar left convex. Spine flexible.
Specific model of hips movements. Connection with permanent standing „at ease
on the right leg. Beginning of deformity at the age of 2-3. Clinical symptoms
appear at the age of 8-10.
(2b)
Scoliosis S 2nd/B epg-2D or 3D. Two curves-lumbar left convex and thoracic
right convex. Specific model of hips movements. Connection with permanent
standing at ease on right leg and additionally with laxity of joints or/and
harmful in previous incorrect therapy/exercises. Beginning of deformity at the
age of 2-3. Clinical symptoms appear of the age of 10-12 years. In the 2nd/A
and 2nd/B types of scoliosis - the spine is flexible.
(3)
Scoliosis I 3rd epg-2D or 3D. Specific model of hip movements. Deformity has
the form of a stiff spine. No curves or small ones. The cause is gait only.
Such spine deformity was until 2004
never included and classified as scoliosis. Beginning of deformity at the age
of 2-3. Clinical symptoms are stiffness of the spine in children and in adults permanent pain. Why stiffness?
In situations of maximal limited adduction, internal rotation and very often
also extension of the right hip-appears compensatory movement in the pelvis and
in the spine with every step during gait. This rotation movement in inter-vertebral
joints
is bigger than normal and has the character of distortion and in result causes
fibrosis and stiffness.
Previous therapy
The
various extensions exercises to receive strong muscles were and are only wrong
and improper. They cause iatrogenic
deformity
of the spine-bigger curves, bigger rib hump and more stiff spine. The children
after such therapy very often need surgery. The bad results after improper
therapy were explained as the natural history of scoliosis (Figure 5a, Figure 5b, Figure 5c and Figure 6).
Figure 5a-c: Example of wrong and harmful exercises.
After such therapy-iatrogenic deformity, big curves, big rib hump and maximal
stiff spine.
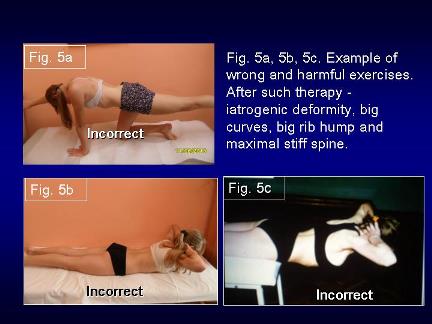
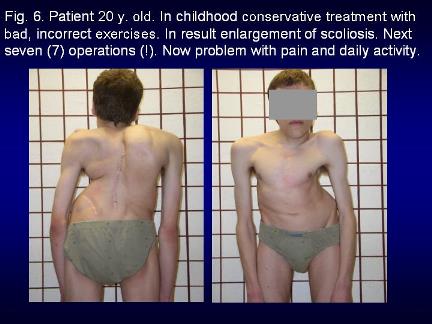
Figure 6: Patient 20 y. old. In childhood conservative
treatment with bad, incorrect exercises. In result enlargement of scoliosis.
Next seven (7) operations (!). Now problem with daily activity. Pain.
New, proper
therapy
Only
stretching exercises giving symmetry of movements and next symmetry of growth
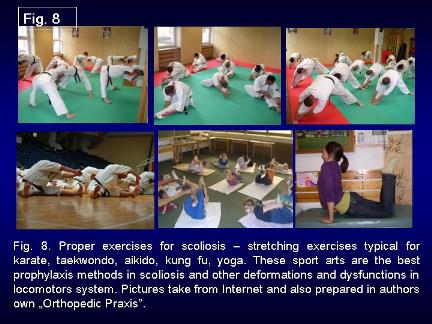
and the development of the pelvis and the spine are proper Figures: 7, 8. The
best are stretching exercises like karate, taekwondo, aikido, kung fu and
others (Figure 7 and Figure 8).
Figure 7: Proper therapy for scoliosis. In program
stretching exercise to receive full range of movement of hips, position of
pelvis and movement of spine. Important standing at ease on the left leg in
every day situation.

Figure 8: Proper therapy for scoliosis in
Sanatorium for Children-under the name-of Dr Janusz Korczak-in Krasnobród.
Cooperation with Pediatric Orthopedic and Rehabilitation Department in Lublin
from 1977. In program only stretching exercises-to receive full range of
movement of hips, position of pelvis and full movement of spine. Important
standing at ease only on the left leg in every day situation.
Very
important are flexion-rotation
exercises
for spine. Such treatment gives good results (Figure 9a, Figure 9b, Figure 9c, Figure 9d, Figure 10a, Figure 10b).
In this part of the paper it is my ethical obligation to inform-that-flexion
exercises for the spine in scoliosis in Poland many years ago (1960-1980) were
introduced by Prof. Malawski S [27]. But at this time the biomechanical
influence going from the hips, pelvis and the factors: standing at ease on the
right leg and gait was not discovered.
Figure 9a-c: Stretching exercises to receive full
movement of right hip, to receive better range of movement and axis of spine. Figure 9d: Result after three years of
treatment.

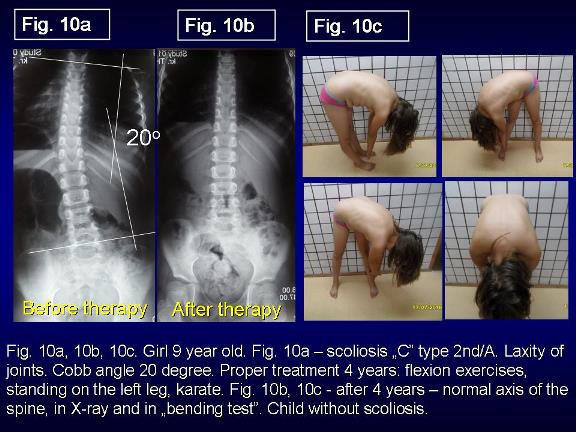
Figure 10a-c: Girl 9 year old. Fig. 10a-scoliosis
C type 2nd/A. Laxity of joints. Cobb angle 20 degree. Proper treatment 4 years:
flexion exercises, standing on the left leg, karate. Figure 10b, 10c: After 4 years-normal axis of the spine, in X-ray
and in bending test. Child without scoliosis.
The possibility
of causal prophylaxis
To
find the danger of scoliosis we should use not only old but also the new tests:
·
We
should define the manner of the standing at ease-left: right leg.
·
Use
the test of adduction of both hips.
·
Adams-Meyer
test-other words-bending test for scoliosis.
·
Lublin
test-side bending test for scoliosis.
·
Elly-Duncan
test to discover the anterior tilt of pelvis and hiperlordosis of lumbar spine-due
to flexion contracture of hips [8].
·
Kneeing
test-to discover the anterior tilt of pelvis
and hiperlordosis of lumbar spine.
Rules of
prophylactic recommendations against scoliosis:
·
Standing
at ease only on the left leg.
·
Sitting
relax-never straight up.
·
Sleeping
in embryo position.
·
Active
participation in sport in school and additionally in clubs-the best are karate,
kung fu, taekwondo, aikido, yoga.
·
Physiotherapy/Kinesio-therapy to obtain full,
symmetrical movement of both hips and movement of the spine-flexion, deviation,
rotation. Especially important is to recover the full adduction and internal
rotation movement of the right hip.
Discussion and my
remarks
Information
to these problems is presented on the Website www.ortopedia.karski.lublin.pl from 2006 [41].
In Poland, in 1995-2009 I have given many lectures about the problem of
scoliosis-at Polish Orthopedics and Traumatology Congresses in Lodź, Szczecin,
Poznan, but till now the explanation of etiology and the rules of new therapy
is not understood nor accepted. Why-because the conviction that the scoliosis is
idiopathic
is so deeply incrusted in the minds of many doctors, professors-that nobody
searches for new knowledge.
My
lectures have also been presented abroad in The International
Research Society of Spinal Deformities (IRSSD) Meetings in
Athens (2002), Genth (Belgium 2006), Liverpool (UK-2008) and in Poznan (Poland
2012) as well in Kolobrzeg (Poland 2009) during Scoliosis Course Meeting of
SICOT and in Czech Republic during SICOT Meeting in 2011 and twice at the Society on
Scoliosis Orthopedic and Rehabilitation Treatment (SOSORT) Congresses in
Athens and in Wiesbaden and remain till now without any response. Only
Professor Martha Hawes [32] and Professor Jan Stokes [35,36] from the USA, as
well Professor John Sevastik [37,38] and Dr. Helen Normelly [33] from Sweden,
Professor Stefan Malawski [27,28] and Professor Kazimierz Rąpała [34,40] from
Poland, as well Professor Harald Thom [39] from Germany-understood my
explanation of the biomechanical etiology of the so-called idiopathic
scoliosis.
In
the article there is all the information about etiology, classification, new
therapy, but-the most important-the rules of causal
prophylaxis of scoliosis. The conviction that can be other etiology of
idiopathic scoliosis-for example presented in articles of Milan Roth (Czech
Republic) or divagations of Prof. Mikhail Dudin from St. Petersburg- Russia (my
friend, we had many personal discussions) not give the answer to all questions
about properties of scoliosis. Only biomechanical etiology answers all
questions and because of this we speak so-called idiopathic scoliosis. The
biomechanical etiology is confirmed over many years by some group of scientist
but not known in all counties in the world. Children of the world are waiting
for prophylaxis. I hope that from Illinois, USA, the knowledge will spread to
other countries, including Poland.
Conclusions
The biomechanical etiologies of the so-called idiopathic scoliosis explain all
questions connected with this spine deformity. Development of scoliosis and the
types of spine deformity are connected with pathological model of hips
movements-limited movements of right hip and the function- standing at ease on
the right leg and gait [9]. Restricted range of movements in the right hip is
one of the symptoms of the Syndrome of Contractures and Deformities according
Prof. Hans Mau and Lublin observations [18].
Every
type of the scoliosis starts to develop at the age of 2-3. If start to be
scoliosis-the development is slowly, over years, long time secret for parents
and doctors if they do not use the new tests. The infantile scoliosis in not
the So-Called Idiopathic Scoliosis. The causal prophylaxis of scoliosis is
possible and should be introduced in every country. Start for prophylaxis in
age of 4-6 years.
The
rules of prophylaxis for all children are:
·
Standing
at ease on the left leg.
·
Sitting
in a relaxed position.
·
Sleeping
in an embryo position.
·
Active
participation in sports in school and at home every day.
·
Especially
beneficial sports are: karate, taekwondo, aikido, kung fu and other similar.
The
special message to all doctors, to all nurses-tray to understand the new
knowledge and proof/check their truest. Never say-no in the first moment. Even anecdotal
cause-standing at ease on the right leg-words of my friends-from Europes
Country-is in the first place-real and true. Please remember-standing at ease
on the right leg is true cause in etiology of the so-called idiopathic
scoliosis.
Acknowledgement
I
would like to express my many thanks to David Poynton and Honorata Menet for
correction of the article.
References
1.
Burwell
G, Dangerfield PH, Lowe T and Margulies. Etiology of adolescent idiopathic
scoliosis: current trends and relevance to new treatment approaches (2000) J
Spine 14: 324
2.
Dangerfield
PH, Dorgan JC, Scutt D, Gikas G and Taylor JF. Stature in Adolescent Idiopathic
Scoliosis (AIS) (1995) 14 Meeting EPOS, Belgium, pp- 210.
3.
Green
NE and Griffin PP. Hip dysplasia associated with abduction contracture of the
contralateral hip (1982) J Bone & Joint Surgery 64: 1273-1281. https://doi.org/10.2106/00004623-198264090-00002
4.
Tylman
D. Patomechanika bocznych skrzywień kręgosłupa, Wydawnictwo Severus (1995)
Wydawnictwo Severus, Poland.
5.
Heikkilä
E. Congenital dislocation of the hip in Finland. An epidemiologic analysis of 1035
cases (1984) Acta Orthop Scandinavica 55: 125-129. https://doi.org/10.3109/17453678408992322
6.
Hensinger
RN. Congenital dislocation of the hip (1979) Clinical Symp 31: 270
7.
Howorth
B. The etiology of the congenital dislocation of the hip (1977) Clin Orthop 29:
164-179.
8.
Karski
T. Etiology of the so-called idiopathic scoliosis. Biomechanical explanation of
spine deformity. Two 272 groups of development of scoliosis. New rehabilitation
treatment. Possibility of prophylactics, Studies in 273 Technology and
Informatics (2002) Res into Spinal Deform 91: 37-46.
9.
Karski
T, Kalakucki J and Karski J. Syndrome of contractures (according to Mau) with
the abduction contracture of the right hip as causative factor for development
of the so-called idiopathic scoliosis (2006) Stud Health Techno Inform 123:
34-39
10.
Karski
T. Explanation of biomechanical etiology of the so-called idiopathic scoliosis
(1995-2007). New clinical and radiological classification (2010) Locomotor
System 17: 26-42.
11.
Karski
T. Biomechanical etiology of the so-called idiopathic scoliosis
(1995-2007)-connection with 279 syndrome of contractures-fundamental
information for pediatricians in program of early prophylactics/280 (2011) J
China Medical Science 8: 278-281.
12.
Karski
T. Biomechanic factors in the etiology of idiopathic dinominated scoliosis. New
282 classification. New clinical tests and new conservative treatment and
prophylaxis (2010) Physiotherapy 39: 85-152
13.
Karski
T. Biomechanical Etiology of the So-called Idiopathic Scoliosis (1995-2007).
New Classification: 285 Three Groups, Four Sub-types. Connection with Syndrome
of Contractures (2010) Pan Arab J Orth Trauma 14: 286-287.
14.
Karski
T. Biomechanical Etiology of the So-called Idiopathic Scoliosis (1995 - 2007).
Three Groups Four Types in the New Classification (2013) J Nov Physiother S2:
289-290. https://doi.org/10.4172/2165-7025.s2-006
15.
Jacek
K and Karski T. So-Called Idiopathic Scoliosis. Diagnosis. Tests examples of
children incorrect 291 treated. New therapy by stretching exercises and results
(2013) J Nov Physiother 3: 292-293.
16.
Karski
T. Biomechanical Aetiology of the So-Called Idiopathic Scoliosis. New Classification
(1995-2007) in Connection with Model of Hips Movements (2014) Global Journal of
Medical Research H: Orthopedic and Musculoskeletal System 14.
17.
Karski
T. Biomechanical etiology of the so-called idiopathic scoliosis (1995-2007)
connection with „syndrome of contractures-fundamental information for
pediatricians in program of early prophylactics (2014) Surgical Science 5:
33-38.
18.
Karski
T and Jacek k. Syndrome of Contractures and Deformities according to Prof. Hans
Mau as Primary Cause of Hip, Neck, Shank and Spine Deformities in Babies, Youth
and Adults (2015) Ameri Rese J Med Surgery 1: 26-35.
19.
Karski
T and Jacek K. Biomechanical etiology of the so-called Idiopathic Scoliosis
(1995-2007). Causative role of „gait and „permanent standing at ease pn the
right leg. New classification. Principles of new therapy and causal prophylaxis
(2015) Canad Open Med Sci Med J 1: 1-16.
20.
Karski J, Karski
T, Pyrc J and Kulka M. Deformations of the feet, knees, hips, pelvis in
children and adults with minimal brain dysfunction Causes treatment Prophylaxis
locomotor system, Movement System (2016) 23: 1-134
21.
Karski
T. Physiotherapy-Correct, or Incorrect, Based on Wrong Principles of Treatment.
Example for Spine, Hip, Knee, Shank and Feet (2017) Ortho Rese Online J 1: 3-6.
https://doi.org/10.31031/OPROJ.2017.01.000502
22.
Karski
T, Karski J, Karska K, Karska K and Menet H. pediatric prophylaxis program of
motor system deformations and illnesses in children. problems of spine, hips,
knees and feet (2018) EC Paediatrics 7.7: 704-714.
23.
Karski
T, Karski J, Karska K, Karska K and Menet H. Prophylactic rules for newborns,
babies, children and adults in problems of hip, knee, shank, feet and spine
(2018) Ortho Res Online J 2:110-112. https://doi.org/10.31031/OPROJ.2018.02.000530
24.
Karski
T and Karski J. Low back pain-problem neurological and orthopedic symptoms.
Causes of treatment back pain-neurology-orthopedic problems clinic, causes,
therapy and prophylaxis advances in practical Neurology (2016) Czelej
Publishing House 4: 9-16.
25.
Karski
J and Karski T. Imperfect hips as a problem at an older age. early and late
prophylactic management before arthrosis (2016) Jacobs J Physiotherapy
Exercises 1: 15.
26.
Karski
T. Biomechanical aetiology of the so-called adolescent idiopathic scoliosis
(AIS). lublin classification (1995-2007). Causative influences connected with gait
and standing at ease on the right leg (2018) J Orthopedics Bone Res 1: 1-10.
27.
Malawski
S. Własne zasady leczenia skolioz niskostopniowych w świetle współczesnych
poglądów na etiologię i patogenezę powstawania skolioz (1994) Chir Narz Ruchu i
ortop Pol 59:189-197.
28.
Stefan
M. confirmation of Biomechanical etiology of the so-called idiopathic scoliosis
(1995).
29.
Mau
H. Etiopathogenesis of scoliosis, hip dysplasia and torticollis of infancy
(1979) J Ortho 5: 601-605.
30.
Mau
H. Atiopatogenesis of scoliosis, orthopedic library (1982) Enke Verlag Stuttgar
33: 296-297.
31.
Hans
M. confirmation of Biomechanical etiology of the so-called idiopathic scoliosis
(1998)
32.
Martha
H. confirmation of Biomechanical etiology of the so-called idiopathic scoliosis
(2002)
33.
Normelly
H. Asymmetric rib growth as an aetiological factor in idiopathic scoliosis in
adolescent girls (1985) United Kingdom, 1-103.
34.
Rąpała
K. in Tylman D. Patomechanika bocznych skrzywień kręgosłupa, Wydawnictwo Severus,
Warszawa, 1995, Seiten 167.
35.
Stokes
IAF. Studies in technology and informatics (1999) Res into Spinal Deform 59:
1-385.
36. Stokes
J. confirmation of Biomechanical etiology of the so-called idiopathic scoliosis
(2006)
37.
Sevastik
J and Diab K. Studies in technology and informatics (1997) Res into Spinal
Deform 37: 300-301.
38.
John
S. confirmation of Biomechanical etiology of the so-called idiopathic scoliosis
(2008)
39.
Harald
T. confirmation of Biomechanical etiology of the so-called idiopathic scoliosis
(1995)
40.
Tylman
D. Automechanika lateral curvatures of the spines (1995) Wydawnictwo Severus,
Poland.
41.
www.ortopedia.karski.lublin.pl
*Corresponding author
Tomasz
Karski, Department of Pediatric Orthopedic and Rehabilitation, Vincent Pol
University, Poland, Tel: +48 604 933 234, E-mail: tmkarski@gmail.com
Citation
Karski T.
Biomechanical etiology of the so-called idiopathic scoliosis (Adolescent
Idiopathic Scoliosis [AIS]). New classification rules of therapy and
prophylaxis (2019) Nursing and Health Care 4: 81-85.



