Introduction
Epistemology
is the branch of philosophy that addresses cognitive sciences, the history of science
and cultural studies. It investigates the origin, methods, nature, and limits
of knowledge. It seeks to determine what we know, how we know it and is used to
determine truth or falsehood as we seek to acquire knowledge of our world.
Swarming in patient care made an initial impact in nursing when The University
of Kentucky Healthcare in Lexington, UK created a standardized approach to
investigate Root Cause Analysis (RCA) in 2009. Since then, swarming in nursing
is described in different ways. For instance, RCAs were referred to as
Swarming. Another description of swarming was of a tool, which was designed to
recognize inefficiencies in staff communication. Another example described
Swarming as a swift evaluation of the patient by the healthcare team and the
final description of SWARM was described as a type of gathering to discuss the
events of a fall. Nevertheless, limited sources described events of swarming directly
in nursing and the ones that did were difficult to access and not open source.
To fill this gap, we presented a review of the various examples of swarming and
recommended a novel approach of how swarming may be utilized in Intensive Care
Units (ICUs) [1,2].
Aim
We
reviewed the research literature and examined the epistemology of swarming in
patient care. The admission process of patients into ICUs can be busy to
utterly chaotic at times. To the untrained eye, staff may be observed milling
around in a small space trying to stabilize and provide care to patients. In
order to provide some semblance of structure, to prevent duplication of tasks
and to ensure required tasks for standard of care are completed, we recommended
an innovative approach to assist the nursing staff when admitting critical
patients into ICUs.Method
Electronic
databases CINAHL, MEDLINE, EMBASE, PsycINFO, ProQuest, PubMed and the Internet
were searched using the terms “swarming” and “nursing”. Although the
recommendations are not a formal guideline, the AGREE checklist was used to
develop this manuscript. No restrictions of published dates were placed. The
target populations were patients and articles that discussed the use of
swarming in patient care were selected. All articles that included swarming of
insects were excluded. There were limited articles available on the use of
swarming in patient care. Three articles were published by the Joint
Commission, another by America’s Essential Hospitals, and the next was as a
letter to the editor of the Annals of Emergency Nursing. A systematic review
was conducted on these works and the examples outlined below.
First Example
of SWARM
RCA
is a universal approach used to investigate undesirable vulnerabilities in
health care systems. From this research, RCAs were colloquially termed
Swarming. The authors described five key steps to a SWARM. The process usually
begins with an unwanted patient event; staff SWARMs to the site to determine
cause or immediate corrective actions; an incident report is completed by the
front-line worker; department heads review and evaluate the report as soon as
possible; and then a meeting is set up for staff to determine what happened,
why it happened and how to prevent the event from happening again see Figure 1. A meeting is then conducted
in a neutral blame-free environment, introducing the process, the plan, purpose
and the legal protections for staff who speak up. Everyone in the room is
introduced, the facts of the incident are reviewed, discussion of the incident
with any contributing factors and finally, proposed action plan, assignment of
individuals to take ownership for additional investigations and implementation
of a plan of action [2].
Second Example of
SWARM
Williams
et al., [3] used a quality improvement process to recognize, evaluate and
encourage open dialogue with front-line workers to improve problem solving in a
Pediatric ICU (PICU). The authors created a tool to empower caregivers to share
information about problems or perceived problems and to quickly develop
solutions in order to eliminate errors, process improvement and to develop a
system of high reliability. The SWARM tool was designed to identify
communication and inefficiencies in performance to develop an infrastructure of
high reliability when managing problems. The approach to a problem specific
SWARM begins by consulting upstream and downstream stakeholders in order to
understand the scope of a problem. There is the use of an electronic tracking
system to list the problems in categories, as well as possible solutions. Then,
there is a process to disseminate learning opportunities to the involved
caregivers on the specific units [3].
Third Example of
SWARM
In
a letter to the Editor of the Annals of Emergency Department (ED), Perniciaro
and Liu described the redesign process of a Pediatric ED with upwards of 80,000
visits per year. The authors described Swarming as the instant evaluation of
the patient together with the nurse, resident, and senior ED physician.
Historically, in the ED a patient was initially assessed by the nurse, and then
a medical assessment was performed by the physician.
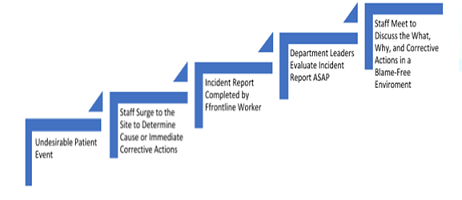
Figure 1: The Process of Swarming.
However,
in their new model, patients were sorted quickly into tracks, placed in beds
without the usual triage process, physicians were placed into zones, and
patients were moved into treatments-in-progress and discharge areas. By
eliminating the traditional serial workflow, efficiency was garnered via
concurrent assessment of patients and education of residents. Using this
process, this ED saw a drastic reduction in wait times and residents were able
to model the senior medical staff. The authors asserted to have given birth to
the concept of "swarming," and concluded that Swarming as a new
process seem promising, but has several disadvantages including its efficacy
and individual variability [4].
Fourth
Example of SWARM
Motuel
et al., [5] described a patient safety incident that occurred in a UK hospital.
SWARM was described as a type of post incident huddle that was performed soon
after the event in order to make improvements. SWARM was compared to RCAs as a
superior tool because it stressed a blame-free culture with a focus on
addressing the underlying issues. This example builds upon the standard
approach and seminal work of Li et al, on how to investigate safety events that
affect patients [2].
Reasons for ICU
Admissions
The
Society for Critical Care Medicine reported on the vital statistics of patients
who end up in ICUs in the U.S. Nearly six million patients are admitted per
year, needing invasive monitoring, airway support, and stabilization of life
threatening conditions, management of illness or injuries, restoration of
homeostasis, or care for the dying patient in a collaborative and
interdisciplinary environment. About 20% of acute Care patients are admitted to
ICUs, with approximately 58% of ED patients resulting in ICU admissions. The
most common ICU admissions are septicemia, percutaneous cardiovascular
procedures, cerebral/myocardial infarction, and respiratory system diagnosis
with up to 30% of patients requiring ventilatory support. The admission process
of this patient population into ICUs can be busy to downright chaotic [6].
Swarming in ICU
Admissions
Critically
ill patients are often transported from EDs, Operating Rooms, other areas
within a hospital system, or from Critical Care Transport. Generally, the
receiving staff for a patient in the ICU include a Registered Nurse (RN), a
respiratory therapist, and an Intensivist (physician who specializes in
critical care medicine). In order to have the best outcomes, several actions
are often performed simultaneously. During this period, an “all hands-on deck”
approach is used where all available staff SWARM into the room to help. Nurses
may be observed performing tasks like hooking the patient up to a cardiac
monitor or trying to start peripheral intravenous lines. There
is usually no structure to these practices. Some would agree this is the
culture of the ICU where nurses show up, lend a hand, and then return to their
assigned patients. As the helpers are busy attempting to stabilize the patient,
the primary RN should ensure the medications and equipment are verified for
activation and correct settings. Some of the tasks needed once the patient
arrives into the ICU suite are for the primary RN to receive a bedside report
from the healthcare team, often using the framework called SBAR (Situation,
Background, Assessment, Recommendation). Timely tasks include logging into the
Electronic Health Record to start and or pend the admission note. Other
simultaneous tasks are listed in the admission to ICU tasks checklist (Table 1) [7].
The
assumption is the primary RN will be familiar with the healthcare team located
in the ICU and feel comfortable with them to designate some of these tasks.
Like processes used in the ED by Perniciaro and Liu to optimize clinical
efficiencies, swarming could be used in ICUs to prevent duplication of tasks.
We recommend the primary RN assign tasks to staff who show up to help. The
checklist may be taped on the entrance door into the ICU and staff who complete
a task may check the right-hand side of the checklist to express completion.
Once the team returns to their designated areas, the primary RN will need to
verify, but not have to spend a long time completing the tasks alone. This
checklist may also be a good tool to communicate with oncoming staff at the
change of shift. The checklist may be updated as needed by the nursing staff to
fit their ICUs and to include tasks specific to their workflow [4].
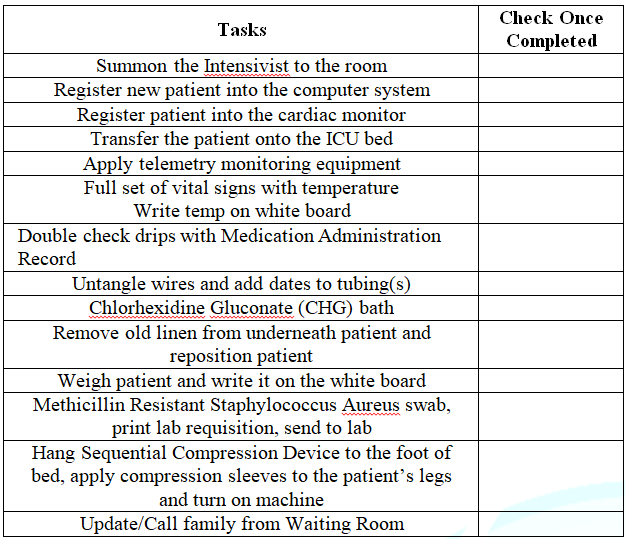
Table 1: Admission to ICU Tasks Checklist.
Limitations
A
standard definition of Swarming does not exist. Besides the benchmark study by
Li et al., there is limited research on the use of Swarming in healthcare and
no mention of its use in any ICUs. Swarming ICU patients would rely on the
number of available staff to help to stabilize patients. When staff SWARM to a
patient during the ICU admission process, the environment can seem chaotic, but
quick assignment of roles before patient arrival or on arrival to the ICU may
guide staff to be more efficient. The goal is to reduce the number of tasks for
the primary RN to perform, freeing up time for continual assessment of the
critically ill patient [2,5].
Conclusion
The
epistemology of Swarming in patient care revealed that it is a colloquial term
created by a British hospital system in 2009 to describe RCAs. We described
four examples of Swarming found in the nursing literature. Each example was
unique and described measures to improve patient safety, and or ways to improve
efficiencies in workflow through communication and performance. When the
Swarming process was used in the ED, it helped to improve delays and prevented
frustrations from patients answering repetitive questions. Similarly, Swarming
a patient during the admission process in ICUs may improve communication
amongst staff and help the primary RN to perform continual assessments in the
stabilization of critical patients. No best practice exists on how to SWARM
admitted patients into ICUs, but this process is performed by nurses daily and
lacked a name until now. We believe the use of our checklist could enhance the
ICU admission process and be used as a tool to streamline tasks, thus avoiding
duplication and supporting the primary RN.
References
1. Bourgeois
N. (2011). An epistemology of leadership perspective.
2. Li J, Boulanger B, Norton J, Yates A and Swartz. Swarming
to improve patient care: A novel approach to root cause analysis (2015) Joint
Commission J Qual Pati Saf 41: 494-501.
https://doi.org/10.1016/S1553-7250(15)41065-7
3. Williams EA, Nikolai D, Ladwig L, Miller C and
Fredeboelling, E. Development of swarm as a model for high reliability, rapid
problem solving, and institutional learning. Joint Commission (2015) J Qual
Pati Saf 41: 508-13. https://doi.org/10.1016/j.evalprogplan.2008.08.009
4. Perniciaro J and Liu D. Swarming: A new model
to optimize efficiency and education in an academic emergency department (2017)
Annals Emerg Med 70: 435-436. http://dx.doi.org/10.1016/j.annemergmed.2017.05.012
5. Motuel L, Dodds S, Jones S, Reid J and Dix A.
Swarm: A quick and efficient response to patient safety incidents (2017)
Nursing Times 113: 36-38.
6. Society of
Critical Care Medicine (2019) Critical care statistics.
7. Liverpool
Hospital (2017 February). ICU guideline: Clinical guidelines, receiving a
patient into ICU.
*Corresponding author
Aretha D Miller, Nursing Department, Aspen
University, Denver, USA, E-mail: aretha.miller@aspen.edu
Citation
Miller
DA and Stephenson C. The epistemology of swarming in patient care: an
innovative approach to admitting patients into intensive care units (2021)
Nursing and Health Care 5: 41-43.



