Introduction
Dental caries is
one of the most common chronic illnesses in the whole world, affecting people
across all age gatherings and nations [1]. Carious teeth can be both prevented
and arrested by utilizing fluoride-based materials for example professional
applied varnishes [2]. Dental caries is the most continuous childhood chronic
disease worldwide [3]. Childhood caries the available quantity of one or more Decayed, Missing
or Filled Tooth Surfaces (DMFS) in any primary tooth in a
preschool-mature youngster has been associated by the American Dental
Association as an important feature of public health issue [4]. ECC initiates
with a white -spot lesion in the upper primary incisors along the margins of
the gingiva. If the lesions progress, cavities can progress that will lead to
destruction of the tooth.
Children with
experienced early childhood caries will lead to future destruction of primary
and permanent teeth, In fact some of the children with caries are suffering
from lack of eating, underweight because of the associated pain, which is also
related to iron deficiency. In the coming years, a decrease in general caries
indicators has been accounted for; in any case, an expansion in childhood
caries has been documented [5]. If childhood caries stands by untreated, oral health
lifestyle, body weight, growth, school attendance and school
participation can be affected [6]. Children caries treated under general
anesthesia have a higher inclination to develop dental caries in the permanent
dentition, because severe childhood caries experience is a
significant predictor for adult caries, methodologies to prevent and control
childhood caries are essential to improve general and oral health [7,8].
Clinical examinations
have been shown the effectiveness of SDF in childhood caries prevention and
arrest. Semiannual utilization of SDF at 38% concentration has been recommended.
SDF has been proposed for complex-to-treat carious lesions and patients with
high probability of caries, adding those with medical or behavioral
complications, those individuals who need numerous treatment visits, or those
without access to dental care [9].
Review of the Literature
Fluoride has
multiple ways of application and agents in preventive
dentistry which can be delivered as topical (as in, gels,
foams, silver fluoride and fluoride varnish) or systemic (as in community water
fluoridation) and self-administered such as (toothpastes and
mouthrinses) and we can ignore the fact that
fluoride transmission through topical or systematically and aim to delivering
it to the oral cavity, so that it can play a role in caries control [1]. The
key subject of the growing hysteria on fluorosis is the consumption of fluoride
from toothpaste by young children, resulting in the intake of extra fluoride.
While young children's use of fluoride toothpaste may be considered a risk
factor for dental fluorosis, the following shows the most common usage of
fluoride agents in the dental field for children
Silver Diamine Fluoride
Silver diamine
fluoride is a correlation with silver nitrate and fluoride that reduces the
progress of cariogenic bacteria to grow, inhibits degradation of collagen in
dentin, and hinders demineralization and stimulates remineralization of both
enamel and dentin. Japan used SDF for decades and in Argentina, China, and Brazil
and has been approved by the Food and Drug Administration (FDA) for tooth desensitization.
Concentration of the silver diamine fluoride is 10 to 38% to enhance dental
caries. It is a simple and inexpensive procedure and is called minimally
invasive dentistry and the way of application was lesion first located with
mirror and explorer only and SDF was applied with proper cotton isolation and
is suitable for younger and uncooperative patients [2].
SDF shown to be
89% from 49% to 138% more effective in arresting dental caries in primary teeth
than other active treatments. The main disadvantages in SDF is black staining
and when the patients that are allergic to silver [3]. Mechanism of action of
SDF that fluoride ions mainly works on tooth structure while silver ions acts
mainly on cariogenic bacteria. SDF reacts with hydroxyapatite in an alkaline
environment to form calcium fluoride and silver phosphate as major reaction
products. Calcium Fluoride (CaF2) provides adequate amount of
fluoride to form fluorapatite [Ca10(PO4)6F2]
which is less soluble and silver phosphate forms an insoluble layer to
facilitate the transform hydroxyapatite to fluorapatite (Figure 1 and Figure 2) [4].
Fluoride
Varnishes
Fluoride
varnishes were discovered and developed in the early 1960’s so that dentists
could practice topical application of fluoride in a way that provided more
prolonged tooth structure; enamel without consuming time in a dental visit,
Fluoride varnish is a concentrated topical fluoride with a resin or synthetic
base [5].

Figure1:Silver diamine fluoride 38%.

Figure2:Formula of hydroxyapatite and fluorapatite.
Recent commercial
formulations of fluoride varnish such as: Duraphat® (5% NaF-Sodium Fluoride),
Duraflor® (5% NaF) and Fluor Protector® (1%
DifluoroSilano), the ages of the children at base-line varied from 6 months to
8 years for studies of the primary teeth, application technique is very easy
and well tolerated and the time needed to apply the varnish depends on the
number of teeth available from 1 to 4 minutes per patient and the child can
directly close his mouth as varnish hardens as soon as there is contact with
saliva, teeth were dried with gauze, and varnish was brushed onto all surfaces
of the maxillary and mandibular anterior teeth, and the proximal and occlusal
surfaces of the posteriors and forms a film that cohere to tooth surfaces,
patient has to avoid eating for two hours after applying the varnish and not to
brush the same day to give time for the varnish to contact the enamel for
several hours [6].
Also in some
researches fluoride divided into two percentages which was either 2.26% or 0.1%.
Further research revealed that products identified with an identical brand name
(Fluor Protector, Ivoclar Vivadent, Am-herst N.J). A sustain of compositional
change in 1987 from 0.7% fluoride to 0.1% fluoride, the 0.7% fluoride product is
no longer available in the commercial field. Therefore, the data are subdivided
into 2.26% and 0.1% fluoride varnish categories. So, researchers approved that
fluoride varnish reduces the incidence of early childhood caries of up to six
years of age (Figure 3 and Figure 4)
[7].

Figure3:Application of fluoride varnish.

Figure4:Sodium fluoride paste.
GC Tooth Mousse Plus
GC tooth mousse
plus achieved a huge popularity in the commercial field, it works as caries prevention and
treating white lesion in the tooth structure. GC tooth mousse have tooth mousse
(MI paste) and tooth mousse plus (MI paste plus) which contains an ingredient
Casein Phosphopeptide-Amorphous Calcium Phosphate (CPP-ACP) and are marketed by
the GC corporation (Figure 5 and Figure 6)
[8].
Tooth Mousse Plus
contains 900 parts per million fluorides in a molar ratio with the calcium and
phosphate of 5 calcium, 3 phosphates and 1 fluoride which is reported by
Reynolds and co-workers as the ideal ratio for building fluorapatite. The
development of the GC products Tooth Mousse and Tooth Mousse Plus is to be
applauded as scientific innovation is critical in the quest to improve the oral health of
patients [9].

Figure 5: GC Tooth Mousse.
However, when the
dental team use and recommend products for patient care there must be sound
scientific evidence to support their treatment planning decisions and advice. CPP-ACP
in the form of Tooth Mousse and Tooth Mousse Plus are
widely recommended for the prevention of early dental caries [10]. The
manufacturer instructions recommend Tooth Mousse for patients of any age except
those with milk protein allergies but limit the indication of Tooth Mousse Plus
to patients over six years of age because of the fluoride content. These
products are much more expensive to use than fluoride products, so it is
important to examine the evidence supporting their general usage [11].

Figure 6: GC Tooth Mousse Plus.
To this end a
systematic review on the specific use of these two products “GC tooth mousse
and GC tooth mousse plus” for caries prevention and treatment has been
undertaken, in order to determine whether their efficacy warrants use in general dental
practice. The aim of the systematic review is to answer the
question. “Is there sufficient clinical evidence available to support the use
of Tooth Mousse and Tooth Mousse Plus over a routine oral care regimen for the
prevention and treatment of early dental caries?
Sodium Fluoride Gel
The usage of fluoride
gel for the recommended amount every year is possible and it helps in gradually
reducing tooth
decay. It can be self-applied or under supervision
depending on the preference of the individual. A review of trials found that
fluoride gel can reduce tooth decay in children. One in two children with high
levels of tooth decay would benefit from fluoride gel and
as a result would lead to lower levels of tooth decay [12].
However, because
fluoride gel is mostly applied and used in children, research is needed as
children tend to swallow the gel during application. Fluoride gels must be differentiated
from fluoride toothpaste, which are also available in the form of gels. The
amount of fluoride in the toothpaste is substantially less than the fluoride
gel and the fact that fluoride toothpaste contains abrasives means that
fluoride gel can be applied at relatively infrequent intervals [13].
Various methods
and concentrations and frequencies of gel applications have been tested, with
or without prior dental prophylaxis, and different fluoride compounds have been
used. Typically, Acidulated
Phosphate Fluoride (APF) gels in the concentration of
12,300 parts per million of Fluoride (ppm F) are professionally-applied twice a
year. The excessive ingestion of fluoride during topical application is not
recommended as it may cause toxic and harmful effects (Figure 7 and Figure 8) [14-16].

Figure 7: Sodium fluoride gel.

Figure8:Sodium fluoride gel.
Aims and Objectives
· To
compare the effect of SDF, fluoride varnish, fluoride gel and GC tooth mousse
plus on Streptococcus mutants
bacterial load in children.
· To
evaluate the effect of silver diamine fluoride, fluoride gel, fluoride varnish
and GC tooth mousse plus on caries.
· To
compare the effect of prevention of early childhood caries by using silver
diamine fluoride, fluoride gel, GC tooth mousse plus.
· The
objective of this paper is to signify the types of fluoride efficacy on early
childhood caries and the effect on the streptococcus mutants.
Materials and Methods
Duration: 6
months
Study
design:
literature review
Inclusion
criteria:
2010-December 2018, databases which were searched: MEDLINE via Ovid, Web of
science, Embase , Cochrane Library , LILACS and Dental specialties: pediatrics,
oral preventive.
Exclusion
criteria:
Foreigner languages, editorials, letter to the editor, experimental studies
with animals and short communications were excluded from this review.
Data
collection procedure: Searching the databases using the
keywords: sodium diamine fluoride, GC tooth mousse, fluoride varnish, fluoride
gel, early childhood caries and caries.
Ethical
consideration: Ethical approval was obtained from RAK Research
Ethics Committee and favorable ethical opinion was obtained from The Ministry
of Health and Prevention Research Ethics Committee; under reference number
(RAKMHSU-REC-50-2019-U-D) (Appendix-1).
Results
Study process:
the databases (MEDLINE via Ovid, Web of science, Embase, Cochrane Library and
LILACS) were searched; a total number of 40 articles were identified for an
inclusion. Only 16 articles were included in the research according to
inclusion criteria and 5 articles were excluded according to the exclusion
criteria. As shown in the flow (Figure 9).
Discussion
This topic was
selected to differentiate between the agents of fluoride: silver diamine
fluoride, fluoride varnish, silver fluoride and GC tooth mousse plus as
antibacterial agent and mainly to check if the silver diamine fluoride has heterogenous
or homogenous effect comparing to the other agents. But with upcoming
generations preventive dentistry is getting improved with new knowledge and
different agents.
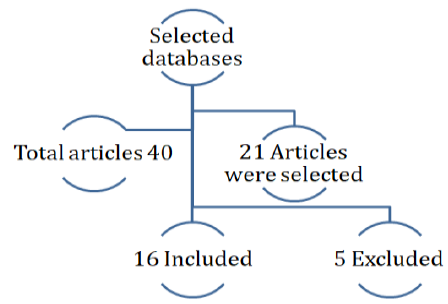
Figure9:Flow diagram 1 of the method of data collection that shows the databases that were searched of a total 40 articles and 23 of them were selected and 16 articles included whereas 5 of them were excluded.
Discussion
of the materials and methods: Articles after 2000 were used for
the research because of the new silver diamine fluoride agent used at this
time. Databases such as MEDLINE via Ovid-Web of science-Embase-Cochrane
Library-LILACS were used as they contain all the medical articles which were
very helpful for the research.
Discussion
of the results: 2 studies assessed un-clear and need further
research of SDF. 5 studies assessed that 12% of SDF has no effect but 38% has
an effect with dentin and enamel with black staining as an disadvantage.1 study
showed that SDF is safe and effective compared to fluoride varnish, 2 studies
showed that tooth mousse is recommended for early child caries without
mentioning SDF and 3 studies found that it decreases the growth of S.Mutants and aids in the
remineralization of both enamel and dentin
structure.
The articles
discussed in the following research studied the effect of silver diamine
fluoride although there were 5 of the articles in the study had no conclusive
results due to the lack of enough evidence, (Oliveira, 2018) and in another
article the results needed further investigations to spot the difference
between different materials. In studying the different materials such as silica
tetrafluoride, fluoride gel, sodium fluoride and SDF they have found that they
all help in the remineralization of early enamel caries. As for the fluoride
gel the result showed arresting the effect on dentine [14].
The study in Table 1 explains that fluoride varnish
was shown to reduce the intensity of primary tooth caries in children of six
years of age and younger [4]. It is shown in table 1 of the included articles
that different concentrations of SDF gave different results, the more you apply
SDF in about 38% it will give an effective result but it would have black
staining with no further complications, but in giving SDF in lower
concentration 12% the study have shown that it has no effect whatsoever on childhood
caries [5]. SDF as an agent was proven to be the most effective, safe, and
efficient in comparison to Fluoride varnish and is considered as a non-invasive
method and found that it decreases the growth of s. mutants and it renders the
remineralization of dentin and enamel structure which protects and inhibits the
collagenase and the destruction of dentin collagen [6,7]. According to our
study, In another study showed that tooth mousse plus is recommended for early
dental caries and it is critical in the quest to improve the oral health of the
patients, one of the main reasons people use tooth mousse plus is to restore
mineral balance in the oral environment, And a different study says that
fluoride varnish applied at every child care visits can reduce early childhood
caries (Table 2) [8,9].
Conclusion
To end this
study, silver diamine
fluoride is effective and safe to use as silver fluoride, GC
tooth mousse and fluoride varnish to prevent childhood caries, which saves time
with increased accuracy and patient satisfaction due to its drawbacks, is
contraindicated for patients with sliver allergy and who have oral ulcerations,
periodontal
issues and deep caries. And over time, a faint black mark in
the tooth itself may cause discoloration.
Table 1: Results of included articles. (Refer PDF)
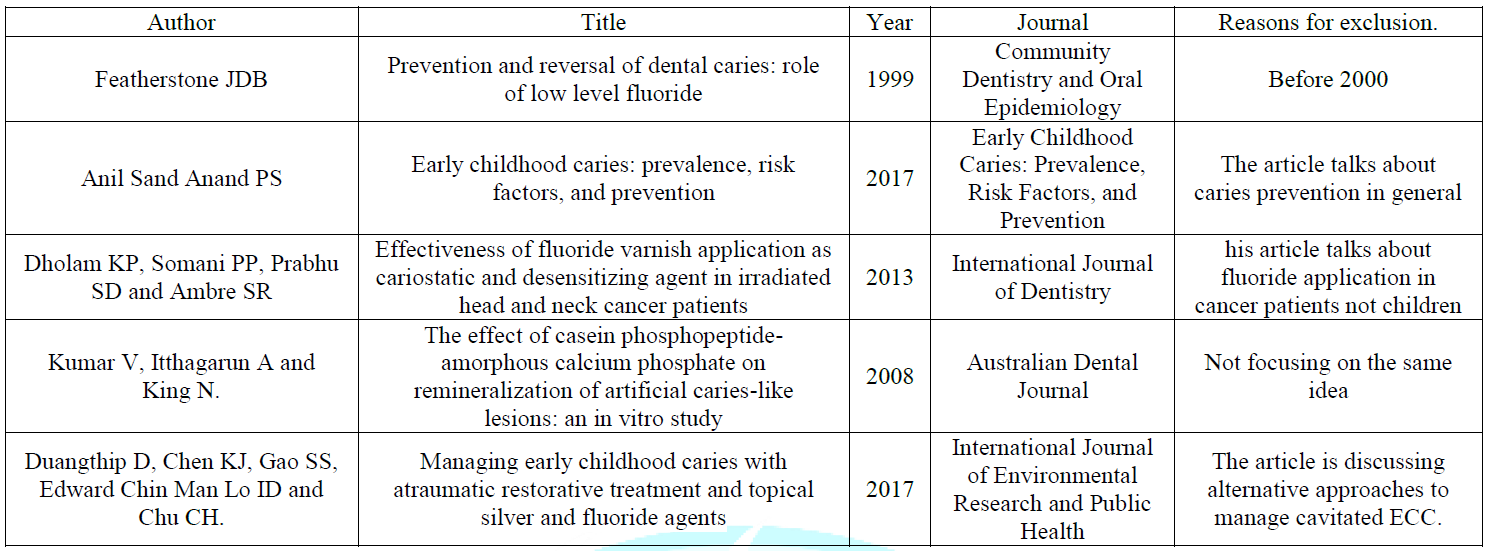
Table 2: Articles that were excluded.


