During
pregnancy, the pregnant mother undergoes significant anatomical and
physiological changes in order to nurture and accommodate the developing fetus.
These changes begin after conception and affect every organ system in the body.
There are many hematological changes during pregnancy including the blood
volume, the red blood cells and the WBCs. Maternal blood volume increases
during pregnancy, and this involves an increase in plasma volume as well as in
red cell and white cell volumes. The plasma volume increases by 40% to 50%,
whereas the red cell volume goes up by only15% to 20%, which causes a situation
that is described as “physiological anemia of pregnancy”. Despite this
hemodilution, there is usually no change in Mean Corpuscular Volume (MCV) or Mean
Corpuscular Hemoglobin Concentration (MCHC). However, several hormones such as
angiotensin, aldosterone, atrial natriuretic peptide, oestrogen and progesterone
may be involved in this interesting phenomenon. The red cell mass increases by
an increase in maternal erythropoietin production. [1-4].
The
drop in hemoglobin is by 1-2 g/dl by the late second trimester and stabilizes
thereafter in the third trimester, when there is a reduction in maternal plasma
volume due to an increase in levels of atrial natriuretic peptide. Women who
take iron supplements have less pronounced changes in hemoglobin, as they
increase their red cell mass in a more proportionate manner than those not on
iron supplements. The red blood cell indices change little in pregnancy.
However, there is a small increase in Mean Corpuscular Volume (MCV), of an
average of 4 fl in an iron-replete woman, which reaches a maximum at 30-35
weeks gestation and does not suggest any deficiency of vitamins B12 and folate.
Increased production of RBCs to meet the demands of pregnancy, reasonably explains
why there is an increased MCV (due to a higher proportion of young RBCs which
are larger in size). Hemoglobin concentration <9.5 g/dl in association with
a mean corpuscular volume <84 fl probably indicates co-existent iron
deficiency or some other pathology [5]. The normal reference range for Hb
during pregnancy has not been established and this limits the diagnosis of
anemia in pregnancy. The World Health Organization has suggested that anemia is
present in pregnancy when Hb concentration is <11 g/dl. A pilot study in
Sudan on hemoglobin level in relation to the PCV as an indicator of plasma
volume hemodilution has suggested that lower Hb values should be considered for
anemia diagnosis in Pregnancy. In this study the normal hemoglobin levels were studied
in different trimesters [6].
Methods
A
cross sectional study was performed on 300 pregnant women presented to
Port-Sudan obstetrical Hospital for antenatal care from the period July 2019 to
April 2020. This was a questionnaire was used for collecting data of study. Blood
(4.5 mL) was collected from each participant cubital vein using the stander
vacutainer blood collection system. The pregnant women were requested to sit
upright on the chair, a tourniquet was applied 5-8 Cm above the venipuncture,
the site was swabbed with alcohol. A full blood count was performed using
Hematological analyzer (Sysmex XP 300). 50µl was taken from each labeled tube
to the Sysmex container and mixed manually or with a mixer to be ready for the
machine to perform the counts. The instrument automatically count RBCs, Hb, and
PCV. The reagents used on this device were Rinse and Diluent. The principle of
the device depends on electricity e.g. Red cell distribution width RDW-SD and
RDW-CV, depend on the average size of RBCs or MCV, also TWBCs count and
deferential depend on volumetric study Each cell is measured by forward-scatter
laser light. Electrical system they displace their volume in a conductive
fluid, which causes a change in electrical resistance as each cell passes
through the aperture. This change is proportional to the cell volume.
Results
Hemoglobin: The mean Hb
value of pregnant women was 11.3±1.4 g/dl, with a range of 7.8-18.7 g/ dl. the
Number of pregnant women of Hb less than 11 g/dl in this study was 103 (38%)
who were considered anemic according to WHO criteria Table 1 shows the mean Hb, RBCs and PCV in studied pregnant women.
Hb was lower during the 3rd trimester (T3) (10.3±1.2g/dl) compared
with the 1st (11.6±1.6g/dl) and 2nd trimesters (11.4±1.4g/dl),
P = 0.008.
RBCs counts: The mean of RBCs
count was 4.1x106 /mm3 with a range of 2.26-4.1x106/mm3. RBCs count were lower
during 2nd P = < 0.001 and 3rd trimester (3.9±0.45
x106 /mm3 (P= 0.007) table 1.
PCV: The mean PCV was
33.35 % with a range of 22.8-54.4 %. The PCV was lower in the 2nd
(33.7±3.4%) and 3rd trimesters (32.1±3.3%) compared with the 1st
(34.17±4.3%) P =0.000 table 1. Hb, RBCS and PCV reference values for Sudanese
female in Khartoum were showed in table
2. There
are significant differences between Hb, PCV, and RBCs count of pregnant women
and adult non pregnant Sudanese women (P= 0.000). (Figure 1,2,3).
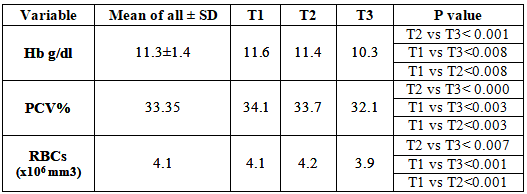
Table1: The mean of Hb, PCV, RBCs count during pregnancy (T=trimester).
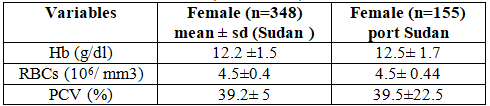
Table 2: Hb, RBCS, and PCV values for Sudanese female.
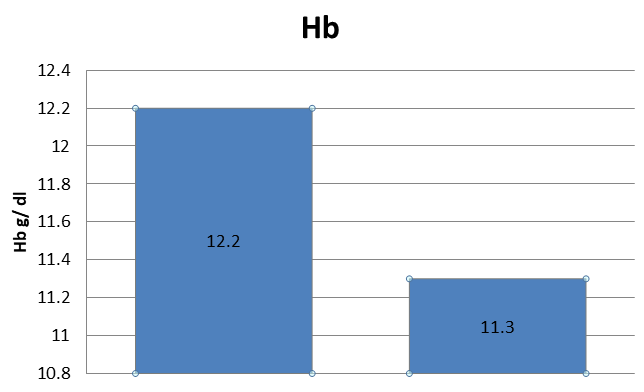
Figure 1: Comparison of Hb, of non-pregnant normal Sudanese females values with the pregnant women.
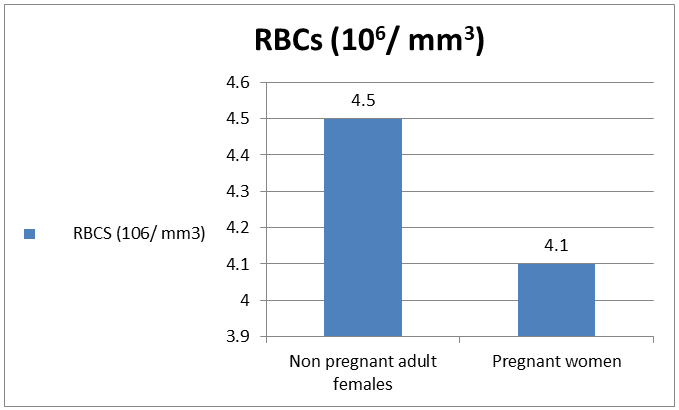
Figure 2: Comparison of RBCs of pregnant women with the normal Sudanese females.
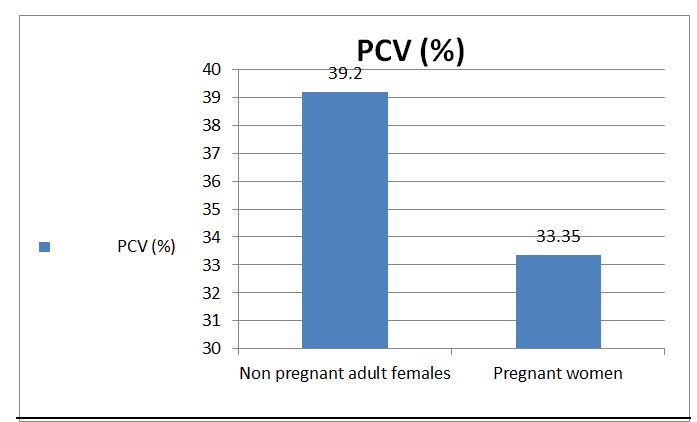
Figure 3: The difference in PCV between pregnant women and normal Sudanese females.
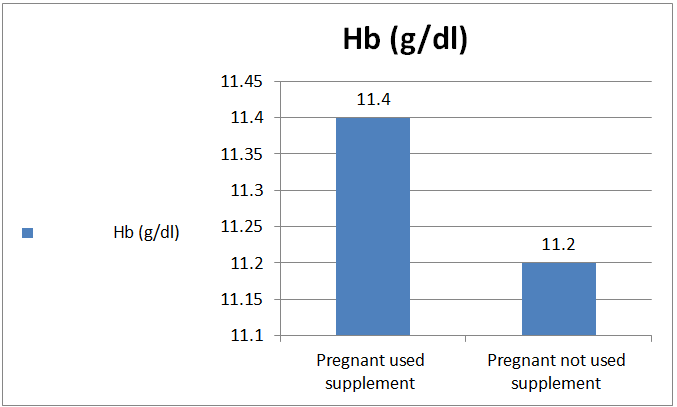
There are (143) women who used iron and folic
acid supplement in this study and there were (126) women not used this supplement,
There was no significant difference in Hb level between pregnant ladies not
using supplement (11.2 g/dl) and those who used them during pregnancy (11.4
g/dl), (P=.32) ( figure 4).
Hb level and tobacco
use
Seven
pregnant women used tobacco in this study four of them used shisha (average
between one to two times/day for period of one to six years) (mean Hb were
11.7) and only one was smoker (one time/day) for six years (Hb was 12.4), while
two females were snuffers (mean Hb were 10.1). Accordingly, there was no
significant effect of tobacco use during pregnancy on Hb level P= 0.188).
Discussion
Hemoglobin and
anemia during pregnancy
The
cut off level of hemoglobin for diagnosing anemia in pregnancy was taken in
most studies as less than 11g/dl according to the WHO recommendation. This
level is less than that diagnosing anemia in non-pregnant ladies (12g/dl) as
with pregnancy there is hemodilution [2]. The cut off level for anemia in
Sudanese non pregnant females could be even lower than 11g/dl as the normal
Sudanese level was found to be lower than the international one [7]. This cut
off level for anemia in pregnancy in Sudan was used in many studies [8-17]. Ishag
Adam carried out several studies on anemia during pregnancy in Sudan. For
example in Eastern Sudan He found that 26% of the group of his study were
anemic (Hb <9.5 g/ dl) and 3.2% were severely anemic (Hb = 5.6 g/ dl) [8].
In this study 38% of the pregnant ladies were anemic according to the WHO
criteria. Ishag Adam also has classified anemia during pregnancy in Sudan as
mild to moderate (Hb 7-10.9 g/dl) and severe with Hb <7 g/dl [17].
Anemia,
iron supplementation and susceptibility to falciparum malaria in Khartoum was investigated
also by Ishag Adam and he found that sever malaria was a leading cause of
anemia. 788 out of 885 pregnant women used iron supplement and folic acid in
Khartoum state [2]. There was no association between iron deficiency anemia and
helicobacter pylori among pregnant women in Khartoum [13]. Aisha defined mean
HbA1c during pregnancy as 4.37 %, (4.7% in 1st, and 3.98 % during 3rd
trimester). A pilot study on the relation of PCV as an indicator of hemodilution
in pregnancy suggested that the cut off level of anemia in pregnancy should be
lower than 11g/dl [18]. The normal Hb level in pregnancy in different
trimesters is important for anemia diagnosis in pregnancy [19] In a study done
by Duria in Khartoum state the hemoglobin levels in the different trimester
were found to be: (10.8 g/d-10.6 g/dl-10.8 g/d) during 1st, 2nd
and 3rd trimester respectively. Here in this study the mean of Hb
during the 1st trimester was 11.6 g/dl, in 2nd trimester
was 11.4 g/dl, while in 3rd trimester was10.3 g/ dl. There is
significant decrease of Hb level during the trimesters of pregnancy (table 1) which can be explained by the
nutrition of the ladies, and there is significant relation between the decrease
in Hb level and PCV. Also there was significant relation between Hb level and
the Number of parity in this study.
As
shown in figure (1) there is significant difference between Hb in this study
from normal Adult Sudanese females [7]. The decrease in Hb level in pregnancy
is mostly related to hemodilution, also there is significant difference between
Hb in this study and normal adult females in Port Sudan whose mean Hb was 12.5
g/d, (P=0). According to the WHO definition of anemia in pregnancy all the
pregnant females in the third trimester in this study are considered anemic and
38.1% of all the sample are considered anemic. If the hemodilution has been
considered as factor the diagnosis of anemia the PCV is an indicator of anemia:
Dilution factor=Pregnant plasma%/Standard plasma%, then the PCV of the pregnant
women in the third trimester was 32% (table1)
which means that the plasma % was 68% and the normal plasma % is 61% (table 2), so the dilution factor will
be: 68/61=1.1 (69). If we multiply this dilution factor with the third
trimester Hb: 1.1 x 10.2 it will equal 11.4g/dl, which is not the level of
anemia. If we consider the total Hb in a normal women with Hb level of 12g/dl
(below which she will be considered anemic), with a 5L blood volume then her
total blood Hb will be:
Total
blood Hb = Blood volume in ml/100 X the Hb level = 5000/100 x 12 = 600g
If
hemodilution considers 40-50% of plasma in pregnancy, will increase the blood
volume to about 6.5L in pregnancy, then the normal total Hb of 600 g will give
a level in pregnancy of: 600/6500 x 100=9.2g/dl, below which she can be
considered anemic. So, Anemia in pregnancy should be diagnosed if the Hb level
is less than 9.2g/dl (Less than 66%).
Conclusions
Calculation the mean of Hb, PCV, and RBCs in pregnant ladies in Port Sudan .The
normal hematological values in pregnancy are different from normal Sudanese
values. There is decrease in Hb level due to delusional effect of pregnancy it
is suggested that the diagnosis of anemia on pregnancy if Hb is less than 9/dl.
References
1.
Locktich G.
Clinical biochemistry of pregnancy (1997) Crit Rev Clin Lab Sci 34:6.
2.
Lund CJ. Donovan
JC: Blood volume during pregnancy (1967) Am J Obstet Gynecol 98: 393.
3. Tchernia G.
Pregnancy-associated thrombocytopenia revisited: assessment and follow-up of 50
cases (1998) Blood 92: 4573-4580. https://doi.org/10.1182/blood.V92.12.4573
4.
Barriga C,
Rodriguez AB and Orega E. Increased phagocytic activity of polymorph nuclear
leucocytes during pregnancy (1994) Eur J Obstet Gynecol Reprod Biol 57: 43-46. https://doi.org/10.1016/0028-2243(94)90109-0
5. Crocker IP,
Baker PN and Fletcher J. Neutrophil function in pregnancy and rheumatoid
arthritis (2000) Ann Rheumat Dis 59: 555-564. http://dx.doi.org/10.1136/ard.59.7.555
6.
World Health
organization. The prevalence of anemia in women. Second edition, Geneva WHO 1992.
7.
Kamal MA, Amir
AB, Asim AO, Mohamed AM, Abdalla A, et al.Reference values for Hemoglobin and
Red Blood Cells Indices in Sudanese in Khartoum state (2019) Int J Health sci res
9:1.
8.
Ishaq A, Gehad El-Ghazali, Munier M
and Mustafa IE. Anemia in pregnant Sudanese women (2004) Saudi med j 25:
1119-1120.
9.
Abdelgadir
MA, Khalid AR, Ashmaig AL, Ibrahim ARM, Aziz AM, et al. Epidemiology of anemia
among pregnant women in Geizera, central Sudan (2012) J Obst Gyn 32: 42-44. https://doi.org/10.3109/01443615.2011.617849
10. Abdullahi H, Gasim G, Saeed A, Imam MA and Adam I. Antenatal
iron and folic acid supplementation use by pregnant women in Khartoum, Sudan
(2014) BMC Research Notes 7: 498. https://doi.org/10.1186/1756-0500-7-498
11. Siddig AA, Khalid RA, Ali AI, Omer A and Musa OA, Normal
Values of Hemoglobin A1c in Sudanese healthy pregnant ladies in Khartoum state
(2017) Saudi J Med 40-45. https://doi.org/10.21276/sjm.2018.3.2.2
12. Ibrahim AA, Rahim HMA, Almobasher B, Bad RM, Alborai A, et
al. Reference Range of Hemoglobin A1c in Khartoum State (2018) Anatomy Physiol
Biochem Int J 4: 55564439.
13.
Mubaraka N, Gasimb GI, Khalafallac
KE, Alid NI and Adama I. Helicobacter pylori, anemia, iron deficiency and
thrombocytopenia among pregnant women at Khartoum, Sudan (2014) Royal Soci Trop
Med Hyg.
https://doi.org/10.1093/trstmh/tru044
14. Adam I, Khamis A and Elbashir MI. Prevalence and risk factors for anemia in pregnant
women of eastern Sudan (2005) Transc Royal Society Tropic Med Hyg 99: 739-43. https://doi.org/10.1016/j.trstmh.2005.02.008
15.
Bushra M, Elhassan EM, Ibrahim AN and Adam I. Anaemia, Zinc and Copper Deficiencies Among Pregnant
Women in Central Sudan (2010) Bio trace element res 137: 255-261. https://doi.org/10.1007/s12011-009-8586-4
16. Wafa MMA, Khalid A and Musa OA. Effect of pregnancy on
packed cell volume and total white blood cells count among Sudanese pregnant
women attending antenatal care at Ribat University Hospital (Khartoum state)
(2018) Int J Reprod Contracept Obstet Gynecol 7: 371-374. http://dx.doi.org/10.18203/2320-1770.ijrcog20180150
17. Ishage Adam and Abdelaziem.A Ali. Anemia during pregnancy,
INTECh, 2016.
18. Rayis DA, Ahmed MA, Abdel-moneim H, Adam I and Mohamed FL.
Trimester pattern of change and reference ranges of hematological profile among
Sudanese women with normal pregnancy (2017) Clinics and Practice 888. https://doi.org/10.4081/cp.2017.888
19. Ahmed MAS, Ibrahim AA and Omer AM. Effect of
pregnancy on packed cell volume and hemoglobin level among Sudanese pregnant
women attending antenatal care at Omdurman military hospital (Khartoum state) (2018)
Gynecol Reproduct Endocrinol 2: 2. https://doi.org/10.35841/2591-7994.2.3.2-4Corresponding author
Manal Hamed Awad
Elmadih, Assistance Professor in Physiology, Head Department of Physiology,
Faculty of Medicine, Red Sea University, Port Sudan, Sudan, Email: manalelmadih@hotmail.com
Citation
Elmadih MHA,
Khalid A, Ali IA, Hussein AA and Musa OAE. Hemoglobin and red blood cells count
in pregnant Sudanese women (2022) J Obesity and Diabetes 5: 8-11.