
 PDF
PDF
Introduction
The
International League Against Epilepsy (ILAE) defines this disease it as a
brain disorder characterized by an abnormal electrical activity, called
epileptic seizures and the neurobiological, cognitive, psychological and social
consequences that this condition entails [1].
Epilepsy is one of the most common neurological
diseases, with more than 50 million people affected around the world and of
which about 80% come from developing regions. The prevalence of epilepsy
worldwide is estimated at 10/1000 people, being one of the most serious
non-infectious chronic diseases in the world. It is estimated that about 5
million people suffer from the disease in Latin America and the Caribbean [1]
with high incidence 30 and 50 new case per year per 100,000 inhabitants, according
to WHO and PAHO office, or 11.9 to 21/1000 according to Brazilian authorities
[2]. Unfortunately, In Paraguay there are no records or statistics of this type
of illness.
Epilepsy
is characterized by recurrent seizures, which are brief episodes of involuntary
movements that can affect a part of the body (partial seizures) or its entirety
(generalized seizures) and are sometimes accompanied by loss of consciousness.
Pharmacological treatment for epilepsy manages to control epileptic seizures in
up to 70% of patients, but in Latin America up to 60% of patients are not
diagnosed or receive treatment due to lack of access [1].
This chronic disease represents 0.5% of the total
global burden of diseases and has significant economic repercussions in terms
of health care needs and lost productivity at work [3,4]. These patients have a
higher risk of suffering physical injuries associated with epileptic seizures,
since epileptic seizures invalidate the individual's consciousness for several
minutes, and expose them to unwanted consequences during that period. If the
patients during a crisis, are performing dangerous tasks, or are surrounded by
potentially harmful elements such as fire, hot water, electricity or chemicals,
seizures will put their own health at risk.
Most studies in epilepsy outcomes were focused on
the psychosocial impact of epilepsy, paying little attention to other type of
injuries, like burns, especially in developing countries where heating or
cooking depends on fire [5]. There are few studies that describe the
association between epilepsy and burns [2,4]. One study revealed that patients
who suffered burns due to epileptic seizures were 1.3% of all hospital
admissions due to burns [6].
Thermal burns represent one of the most complex and
challenging forms of traumatic
injuries, which means great costs for the health system and imposes
significant physical and psychological care on the recovery of the patient and
their relatives [7-10], due to the prolonged hospitalization required. The incidence
severity and nature of the various types of lesions in epileptic patients are
different from those that occur in people who do not have epilepsy [4].
Burns as a result of an epileptic attack represent between 1.6-10% of admissions to burn units, while 3.7-15.9% of adult epileptics have been burned due to seizures however, there is a wide range for these events according to the region of the world and the country of study [7-10]. For this reason, it is useful to carry out these types of studies that help to make visible the problem of the consequences of uncontrolled epileptic seizures in patients belonging to countries with low income level such as Paraguay, where data is still very scarce or null.
Methodology
This
is a descriptive study based on a retrospective analysis of the medical records
of patients who were admitted for severe burns in a specialized public hospital
in the city of Asunción, capital of the Republic of Paraguay.
Unit
of analysis:
Adult patients admitted to the Hospital Specialized in Burns of Asunción,
Paraguay, during the study period.
Study Period: 01-01-2015 to 12-31-2017.
Variables: age, sex, type of burn according to the agent that produced it (Table 1), according to the extension (Table 2); according to the degree of severity (Table 3), body surface area affected [11], presence or absence of a diagnosis of epilepsy, reason for admission, cause of the burn, complications suffered, address of the patient according to urban or rural area.
Statistics: The statistical analysis was performed with the EPI INFO statistical software, each variable was coded for the program management, with its description and its categories. This program allows expressing the results in frequency and percentage of each study variable.
Ethical
aspects:
In order to ensure that research is ethically acceptable, the present work was
carried out according to international standards for biomedical research in
human beings proposed by the Council
of International Organizations of Medical Sciences (CIOMS) where the confidentiality
of the data obtained from patient records, for this purpose it was submitted to
the Research Ethics Committee of the Faculty of Chemical Sciences, UNA.

Table1:: Classification of burns according to the agent that produces it.

Table2:: Correlation of the Burns classifications
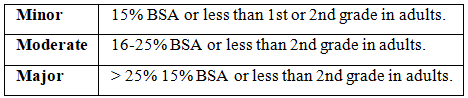
Table3:BA classification of burns according to the percentage
Results
A
total of 937 adult patients entered the Burns boarding room unit during the
study period, 35 patients suffered burns due to epileptic seizures, which
represent 3.73% of all admissions. 62.86% of the patients belong to the female
sex. The age range is between 18 to 74 years, with an average of 40 ± 16.5
years. 65.71% of the patients came from rural areas (Table 4).
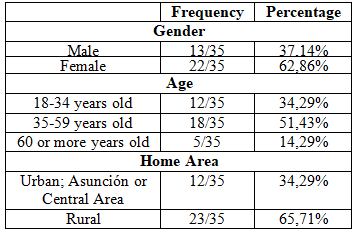
Table4:Characteristics of the patients included in the study
Direct
fire burns correspond to the highest percentage of income (57.14%), the rest
corresponds to hot liquid burns. Regarding the degree of burn, 40% of the
patients suffered second superficial degree burns, the extension is expressed
as a percentage of burned body surface, minor burns were more common, with a
frequency of 94.28% (Table 5).

Table5:Classification of burns according to their characteristics
Patients
received a total of 35 medicines, the most prescribed drug corresponded to
group N for the treatment of epilepsy (Drugs acting on the Nervous System)
according to ATC chart (Table 6).
Phenytoin was the most prescribed and administered medication, with a frequency
of 71.43% of the total patients. Patients without continuity in their treatment
had twice incidence of burns that those with epileptic therapeutical adherence.
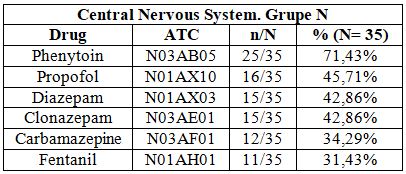
Table6:Classification of the most frequent drugs administered
Discussion
Burns are one of the most common causes of injuries in people with seizure disorders; however, the importance of this relation is often underestimated. Some of the risk factors associated with injuries and accidents in patients with epilepsy are the number of antiepileptic drugs consumed, history of generalized seizures and the frequency of seizures [12-14].
In
this study, 3.73% of admissions in the shock room, corresponded to adult
patients with burns derived from an epileptic crisis, an aspect that reflects a
similar data published by other authors [13], but has a significant difference
with others [14].
Patients
with seizure disorders most often burn while engaged in necessary household
chores or self-care activities. Our work shows that those epileptic patients
who were burned were mostly women (62.86%). This is very likely to be related
to the activity at the time of the burn, since most of the burns occurred at
home, coinciding with Faurie’s [15], and Boschini’s data [3]. 65.71% of
admissions corresponded to patients belonging from rural areas; this could be
due to the fact that in these areas there is less access to electricity or
other ways of heat or cook; also due to the limited information on the risk
factors of seizures that lead to suffer injuries such as burns. The greatest
tendency of burns was by direct fire, which corresponds to 57.14%, certainly a
higher level than data from Laura P. Boschini et al with 28% of injuries [3].
The
most frequent burn among the patients was classified as moderate (according to
the classification according to the Burned Body Surface), 94.28% of the
patients suffered burns between 2-15% in length, similar to data from other
authors [16,17].
Regarding
the degree of burn, the superficial second-degree was the most frequent in
patients studied, although it was found very little difference compared to
second deep degree burns. No patients with first degree burns were found since
they affect only the outer layer of the skin and do not require
hospitalization. Burns tend to be deep, and this is due to the inability of
epileptic patients to withdraw from the heat source during a seizure.
Patients
without adherence to epileptic treatment increased the risk of be submitted to
a burn event. Hence, it is extremely important that in epileptic patients,
continuity of treatment is guaranteed in order to prevent epileptic seizures
that put patients at risk. It is also essential to prevent burns in epileptic
patients, controlled that the environment and their habits do not expose them
to potential risks to certain.
Conclusion
In
the present study it was demonstrated that epilepsy was the cause of burns due
to a seizure crisis in 3.73% of all hospitalizations in the National Centre for
Burns in Asunción, Paraguay. The age range was 35 to 59 years. Flame injury was
the most common cause of burn. The majority of burns were classified in
severity as mild and superficial second-degree burns.
A monitoring program that guarantees access and continuity to the antiepileptic treatments, as well as a management of the environment in order to avoid possible risks might reduce the incidence of burns in this type of patients.
References
1.
Orozco
J, Quintero J, Marin Medina D, Castaño J, Hernández P, et al. Clinical and
sociodemographic profile of adult epilepsy from a Colombian reference center (2019)
Neurologia 34: 437-444. https://doi.org/10.1016/j.nrleng.2017.02.012
2.
Gragnani
A, Müller BR, Oliveira AF and Ferreira LM. Burns and epilepsy-review and case
report (2015) Burns 41: 15-18. https://doi.org/10.1016/j.burns.2014.08.004
3.
Boschini
L, Tyson A, Samuel J, Kendig C, Mjweni S, et al. The role of seizure disorders
on burn injury and outcome in sub- Saharan África (2014) J Burn Care Res 35: e406-e412.
https://doi.org/10.1097/BCR.0000000000000026
4.
Akhtar
M, Ahmad I, Khan A, Fahud Khurram M and Haq A. Burn injury in epileptic
patients: an experience in a tertiary institute (2014) Annals of Burns and Fire
Disasters 27: 126-129.
5.
Berhanu
B, Bewket T, Mengitsu K, Nestanet B, Abebe T, et al. Seizure related injuries
among people with epilepsy at the outpatient department of the University of
Gondar Hospital, Nortwest Ethiopia: Cross-Sectional Institutional Based Study
(2017) Neurology Research International Article ID 4970691. https://doi.org/10.1155/2017/4970691
6.
Torres
Amaro A and Jiménez García R. On the nutritional support of the burned patient
(2016) Revista Cubana de Alimentación y Nutrición 26: 337-364.
7.
Casal
IE. Complications and long-term outcomes of severe thermal burn Pág. 58
injuries and its onset treatment (2017) Revista Argentina de Quemaduras 27: 58-71.
8.
Arriagada
C. Multidisciplinary management of the great burned (2016) Revista Médica
Clínica Las Condes 1: 38-41.
9.
Mercadé
JM, Toledo M, Mauri JA, López FJ, Salas X, et al. Official guide of the Spanish
Society of Neurology of clinical practice in epilepsy (2016) Neurologia 31:
121-129. https://doi.org/10.1016/j.nrl.2013.12.020
10.
Arévalo-
Estrada D, Osorio J and Medina J. Burns associated with epileptic seizures,
accidents not so infrequent (2009) Revista Médica de Honduras 77: 466-469.
11.
Collado
CM, Pérez V, Lorente SR and Pérez FA. Epidemiological characterization of the
burns of the elderly admitted to the Celia Sánchez Hospital (2015) Correo
Científico Médico 3: 396-405.
12.
Schwartz
RJ, Chirino CN, Sáenz SV and Rodríguez TV. Some aspects of the management of
the burn patient in a child surgery service. About 47 pediatric patients (2008)
Rev Argent Dermatol 89: 165-173.
13.
Agbenorku
P, Adamu Bukari AR, Effah AT, Agbenorku M, Odamea Asare NY, et al. Burn injury
in epileptics: The trend and risk factors in the middle belt of Ghana (2018)
Burns Open 2: 122-125. https://doi.org/10.1016/j.burnso.2018.05.001
14.
Téllez
Zenteno J, Nguyen R and Hernández Ronquillo L. Injuries, accidents and
mortality in epilepsy: A review of prevalence, risk factors and prevention
(2010) Revista de investigración clínica 62: 466-479.
15.
Faurie
M, Allorto N, Aldous C and Clarke D. A closer look at burn injuries and
epilepsy in a developing world burn service (2015) S Afr J Surg 53: 1-3.
16.
Josty
I, Narayanan V and Dickson W. Burns in patients with epilepsy: changes in
epidemiology and implications for burn treatment and prevention (2000)
Epilepsia 41: 453-456.
17. Asadi Pooya A, Nikseresht A, Yaghoubi E and Nei M. Physical injuries in patients with epilepsy and their associated risk factors (2012) Seizure 21: 165-168. https://doi.org/10.1016/j.seizure.2011.10.009
*Corresponding author
Gustavo
H Marin, National University of La Plata-CONICET, La Plata, Argentina, Tel: +54
221 4216932, E-mail: gmarin2009@gmail.com
Citation
Montiel CS, Troche MI, Marin GH, Lugo Ortellado
G, Samaniego L, et al. Incidence of burns caused by epileptic crisis in Paraguay
(2020) Neurophysio and Rehab 3: 8-10.
Keywords
Seizures, Burns, Epilepsy.
