
 PDF
PDF
Introduction
Cancer is a group of diseases
that are characterized by the abnormal proliferation of cells, which divide
without control and have a high capacity to invade organs, tissues and spread
through the blood and lymphatic system. It is currently one of the most serious
health problems of humanity, it is among the first as a cause of death in developed
and developing countries. The lung in the organ most commonly affected by this pathology.
Because its diagnosis is made in advanced stages, it is estimated that in 2030
it will continue to be one of the main causes of death. Lung
cancer is one of the most frequent diagnoses worldwide. In Spain, some
20,000 new cases of lung cancer are diagnosed each year, being one of the
tumors with the highest incidence and mortality. According to data from the Global
Cancer Observatory (Globocan), approximately 190,667 incident cancer cases
occur in Mexico each year, of which 7,811 correspond to lung cancer cases. In
Cuba in 2019, cancer was the second cause of death with 25,035 deaths.
Malignant tumors of the trachea, bronchi and lung were the ones with the
highest mortality rates due to cancer, with 5,626 deaths for a rate of 50.1 per
100,000 inhabitants, being 1.3 higher in males than in females [1-6].
As is known, lung cancer is
classified into two large groups: Non-Small
Cell (NSCLC) (which represents 85% of cases and whose most frequent type
currently corresponds to adenocarcinoma), and that of Small Cell (SCLC). These
are totally different tumors in terms of behavior, treatment and prognosis.
About 70% of patients with NSCLC are diagnosed with advanced disease at the
time of diagnosis. Although not They constitute a histopathological variety,
malignant tumors located in the lung apex are called Pancoast Tumor, in honor
of the eminent physician who conducted studies on their presentation and
treatment [1,4,6].
There are several risk factors
that can increase the chances of lung cancer such as tobacco smoke. On many
occasions, the Pancoast tumor debuts with osteomyoarticular manifestations and
the patient goes first to an orthopedic consultation than to others such as
Internal Medicine or Comprehensive General Medicine. Metastatic
disease (FS) is the most common malignant entity. In the United States of
America each year 1.2 million new cases are diagnosed, of which 50% have invasion
of bone structures. On many occasions, the metastasis is the cause of the
patient attending the medical consultation and not the primary tumor. A
clinical approach and medical thinking are necessary to make an accurate
diagnosis of cancer [1,7-9].
Clinical Case
72-year-old white male patient,
peasant origin and health history, who spontaneously attends the Orthopedic
Guard Corps of the Mártires del 9 de Abril University Hospital in Sagua la
Grande province of Villa Clara, Cuba, because for a few weeks An increase in
volume is noted in the back of the right hand accompanied by pain without any
history of trauma. The following examinations revealed.
Physical Exam
SOMA:
Discrete increase in volume of the back of the hand towards the ulnar side,
painful on deep palpation, no collateral circulation or color changes (Figures 1 and 2).
Respiratory
system: Vesicular murmur preserved in both lung
fields and no rales. FR of 22 per minute.
Complementary
made:
Hemoglobin (Hb): 12.3 g/dL
Leukogram: 9.3 x 109/L
Polymorphonuclear: 60%
Lymphocytes: 37%
Eosinophils: 03%
Platelet count: 200,000/mm3
Calcium (Ca): 2.7 mmol/l
Phosphorus (P): 1.6 mmol/l
Alkaline phosphatase: 62 IU/L
Alanine aminotransferase (TGP):
12 IU/L
Aspartate aminotransferase (TGO):
30 IU/L
Electrocardiogram (EKG): Normal
AP
and Lateral X-ray of the hand: An osteolytic
image of the carpal bones is observed with effacement of the Great and Hook
bones and partial involvement of the Pyramidal and the Hamate (Figure 3).
Chest
X-ray: Image of condensation in the right
upper lobe of the lung compatible with a block of pneumonic condensation, TB or
Pancoast tumor (Figure 4). They are
also indicated:
Bacteriological sputum I and II:
Negative
Cytological sputum: Negative
BAAR I and II sputum: Negative
It is discussed in conjunction
with Medicine and Anesthesiology and it is decided to take to the operating
room for regional anesthesia (Phleb-analgesia) to perform excisional biopsy of
the hand injury.
Biopsy
of hand lesion: Anatomical-pathological report:
metastasis of highly undifferentiated lung adenocarcinoma. With this result,
Oncology is sent where chemotherapy treatment begins immediately.


Figure 2: Side view of the hand where the increase in volume is better seen.
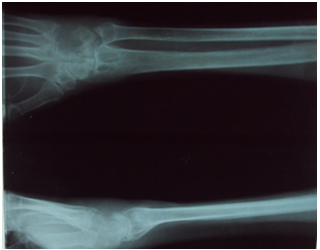
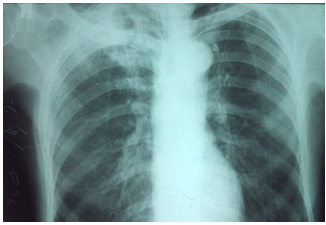
Figure 4:Chest X-ray showing image of condensation in the upper lobe of the right lung.
Discussion
Several authors agree that lung
cancer is more frequent in males, and the ages between 61 and 80 are affected.
This coincides with the case studied, which is a 72-year-old male patient
diagnosed with right lung cancer. In studies carried out in Cuba, it was found
that in terms of the topographic location of the lung cancer, it was more
frequent in the right lung, mainly in the upper lobe of this same side. The
case under study coincided with this topographic location of the tumor, the
which is called a Pancoast tumor [10,11].
Although the Pancoast tumor
generally manifest clinically as pain in the shoulder and towards the arm,
Horner's syndrome (enophthalmos, ptosis, myosis and anhidrosis) and atrophy of
the muscles of the hand; in the case described, none of the symptoms were present
or any respiratory symptoms. When the patient attended the consultation, he
only complained of osteomyoarticular symptoms due to the increase in volume in
the back of the right hand accompanied by pain, with no history of trauma in
the region. In several reported cases, a warning is given to the fact that
patients with Pancoast Tumor mostly attend the Orthopedic consultation first
because they generally present with osteomyoarticular manifestations, as
happened in this case [1,8].
The radiological signs in Pancoast
Tumor are a small and homogeneous shadow at the end of the lung apex
accompanied by more or less local destruction of the rib and vertebral
infiltration. In the case presented, the chest X-ray showed an image of
condensation in the upper lobe of the right lung compatible with Pancoast
tumor, without ribs or vertebrae; However, in the right hand lesion, an
osteolytic image involving carpal bones corresponding to bone metastasis in the
appendicular skeleton is observed, which is not the most frequent found by
other authors who affirm that 70% of bone metastases occur in the axial skeleton
and only 10% in the appendicular. The types of bone metastases can be according
to their radiographic appearance: bone destroying (lytic), bone producing
(blastic) and mixed. Lytic lesions are the most common and represent 75%, the
above described corresponds to the type of lesion found in the X-ray of the
hand of the patient under study [1,9].
At present, adenocarcinoma of the
lung is the most common primary lung cancer seen in the United States and in
most of the countries of the world. In studies carried out in Cuba and also in
Paraguay on the behavior of lung cancer, a higher incidence of non-small cell
carcinoma and with a predominance of the histological variety adenocarcinoma.
To perform the histological diagnosis of cancer, it is necessary to perform a
biopsy of the lesion, as in this case studied, the lung lesion had difficult
access while the lesion at the carpal level led to fewer complications, it was
decided to perform excisional biopsy of the lesion of the carpus and
histological study of the sample after which it was diagnosed as a result:
metastasis of highly undifferentiated lung adenocarcinoma, which coincides with
what was found in the different studies by other authors. Although it has been
described that this type of tumor has a strong association with previous
smoking, in our case this antecedent is not collected, so factors such as aging
and genetic predisposition could be invoked in the risk factors present in this
patient [7,9].
The standard treatment for
Pancoast's tumor is induction chemoradiotherapy,
followed by surgical resection. In this case, the patient was consulted with
Internal Medicine and Oncology and chemotherapy was indicated. The presence of
osteomyoarticular symptoms in a patient with X-ray that shows an image
suggestive of a lytic lesion should suggest a possible bone metastasis from a
distant malignant process and the study should focus on its diagnosis. Pancoast
tumor is one of the most common lung adenocarcinomas, and its osteomyoarticular
presentation highly possible [12].
References
1.
Cordero AER, Labrador LJ, Castaneda
RA, Gomez EH and Pereda Gonzalez EP. Pancoast tumor report of a case (2019)
Cuban J Health Tech 10: 5.
4.
Marco FA. Lung cancer in our days
(2019) J Respiratory Pathol 22: 39-42.
5.
Arrieta O and Lazcano E.
Lungcancer the burden of the disease and advances in diagnosis and treatment (2020)
Public health Mex 61: 217-218. https://doi.org/10.21149/10660
6.
Statistical
Yearbook 2019. Directorate of Medical Records and Health Statistics.
7.
Leon SJA, Aguero MA, Gauna C and
Leon MA. Etiological factors and characterization of patients with lung cancer
at the National Cancer Institute, Paraguay (2020) virtual Soc Parag Med Int
marzo 7: 56-65.
8. Velazquez EP, Gongora DR and Trista MS. Pancoast tumor diagnosis (2016) Electron magazine 41: 853. http://revzoilomarinello.sld.cu/index.php/zmv/article/view/853
9.
Lopez AA, SotoCarrasco SR and
GarciaLorenzo YC. Bone metastases: orthopedic approach (2019) AMC 23: 144-154.
10. Suarez
NH, Ravelo DD, Sanchez MS, Rojas MPM and Diaz MH. Epidemiological clinical
characterization of lung cancer in patients seen from 2016 to 2017 (2020) Rev
Medical Sci 24: 4056.
11. Garcia
AC, Mulet EC, Gonzalez TR, Smith NN and Reguifero JCC. Clinical and
epidemiological aspects in patients with lung cancer in a pulmonology service (2018)
Madison 22: 403.
12.
Munante JGH. Tumor and pancoast
syndrome (2019) J Peruvian Soc Inter Med 32: 81-81.
*Corresponding author
Claribel Plain Pazos, Faculty of Medical
Sciences of Sagua la Grande, Villa Clara, Cuba,
Email: claribelpp@infomed.sld.cu
Citation
Pineiro SM, Pazos CP, Plain LD, Sarduy A, Moreira
TM, et al. Osteolysis of the carpus as a presentation of pancoast's tumor (2020) Edel J Biomed Res Rev 2: 38-40.
Keywords
Lung cancer, Pancoast tumor, Bone metastasis.
