
Explore journal overview, editorial leadership, indexing, articles in press, latest published work, and highlights from previous issues.
Commentary :
Over recent years the increasing pressures on hospital based services has raised the question as to whether more clinical facilities can be provided in the community. Accordingly, commissioning groups have focused much of their energy towards research into whether this shift in healthcare models is feasible, cost-effective and satisfactory to both patients and healthcare providers. Specialties which lend themselves towards the possibility of community based models of care include those that manage patients with chronic but stable diseases and Rheumatology, in particular, has been a focus of such research. The structure of rheumatology services varies widely internationally and a multitude of care models are utilized to facilitate service provision. In addition to the standard hospital based referral system and community services, other models include specialized multidisciplinary team based care, triage models using healthcare providers working in expanded roles and, in more rural settings, telemedicine and visiting provider mechanisms [1].
Community based models vary widely depending on the availability of services, but fully structured models can include onsite physicians (either consultant rheumatologists or specialist trained general practitioners), specialist nurses, physiotherapists, occupational therapists, pharmacists and imaging facilities. Such models provide a similar service design to hospital based care; however one of the advantages of a local service is easier access for patients, which is an important consideration for those with chronic debilitating conditions. Other services targeting the long term followup of stable patients may be nurse rather than physician led, though may still include multidisciplinary services. Smaller community models, however, may not provide full multidisciplinary support and therefore further referrals may be required, for example for imaging or therapy. Furthermore, community services may not have a direct relationship with other specialties, for example orthopedics, and therefore further appointments offsite may be required. If external referrals for imaging, therapy or further specialist opinions are required this may result in delays in management compared to hospital based care where such services are likely to be onsite (Table 1).
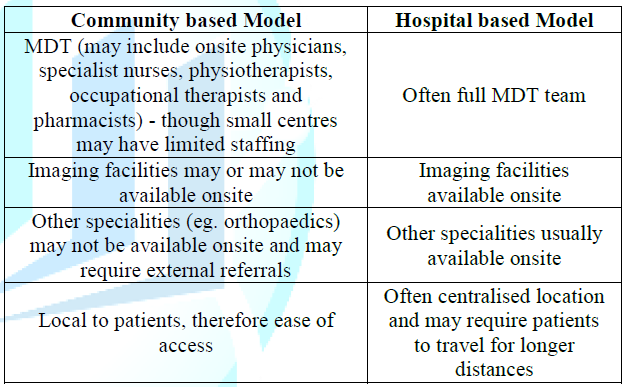
Table
1: Overview of the differences between
community and hospital based delivery models.
Evaluation of community based programs has predominantly focused on the evaluation of specific components of this service. For example, the Arthritis Self-Management Program was initially implemented in the United States as an extension of the Chronic Disease Self-Management Program; both are health promotion programs focused on patient education and enabling patients to have more of an active role in managing their disease in the community. Studies reviewing both programs with regards to quality of life outcomes (for example, global health, pain and fatigue), health behaviors (for example, practice of exercises and mental stress management), self-efficacy and health care utilization (physician visits and hospitalizations) showed positive outcomes, especially in the disease specific group [2]. For those unable to attend training sessions, internet based training programs have also demonstrated improvement in health status measures and self-efficacy [3]. Other vast but more sparsely populated countries such as Australia have additional challenges of delivering a standardized service to both urban and rural regions. In recent years, the development of Models of Care has taken precedent, with the aim to address current and projected community need in the context of local operational requirements. Distinct models exist for a variety of conditions, such as inflammatory arthritis and osteoporosis, and they differ according to community need. For example, the Western Australian Spinal Pain Model of Care uses a community based approach promoting self-management behaviors facilitated by e-health, particularly for rural communities, whereas the New South Wales Osteoarthritis Chronic Care Program is physiotherapist led and based in hospital ambulatory care settings [4].
Although the majority of countries in Asia provide the standard hospital based rheumatology services, Singapore has recently developed advanced practice nurse and/or pharmacist led outpatient clinics for patients with stable disease. A local survey conducted for this service demonstrated received positive feedback from patients, with an overall high degree of satisfaction [5]. Across Europe, the initial diagnosis and initiation of management in patients with inflammatory joint disease tends to be done by a hospital based rheumatologist, however following this, follow-up of these patients in France and Germany is largely done by the GP whereas The Netherlands and Scandinavia favor consultant rheumatologists. Specialist nurses, however, most often work in a hospital based setting, in close liaison with a rheumatologist. Sweden has an extensive network of specialist nurses and nurse led clinics [6].
In the United Kingdom, services such as Modality Partnership and the Community Rheumatology Service have been set up to provide community care in Birmingham and Shropshire, respectively [7,8]. Both services have a multidisciplinary team including physiotherapists, clinicians and nurse specialists; the Shropshire community team also includes occupational therapists, and both offer local imaging facilities. Modality partnership sees patients with simple musculoskeletal disorders such as osteoarthritis and joint overuse injuries, whereas the community rheumatology service is set up to see more inflammatory diseases such as ankylosing spondylitis and rheumatoid arthritis. More recently, in North West London there has been joint working with hospital and musculoskeletal community providers to help review and determine appropriate investigations in patients with multiple musculoskeletal symptoms who do not clearly fit rheumatic disease diagnostic criteria [9]. The aim of these services is for early diagnosis and management of rheumatological disease in the community. The teams include physiotherapists, general practitioners with a specialist interest in rheumatology, specialist nurses and consultants. These clinics also include local imaging facilities.
Furthermore, this community model involves the new role of Extended Scope Practitioners (ESPs) who are often physiotherapists who undertake further specialist training encompass tasks that may previously have been undertaken by the medical profession. This role takes away some of the burden on waiting lists to see clinicians during initial assessment and, in some cases, these specialist practitioners may be trained to perform joint injections, removing the need for clinician involvement in the management of some musculoskeletal disorders altogether. A review on the quality of patient assessment for patients with musculoskeletal disease by ESPs demonstrated high patient satisfaction as well as a high positive correlation of decision making between ESPs and orthopedic surgeons [10]. A qualitative study of nurses, hospital physicians and rheumatology practitioners views of community outreach clinics demonstrated positive overall feedback and highlighted particular advantages in convenience to patients, fluid continuity of care and improvement in the communication gap between primary and secondary care services [11]. Furthermore, nurse led clinics for stable patient follow-ups have demonstrated both good patient satisfaction and equal clinical efficacy using validated disease outcome tools [12].
Interestingly, a study by Watts, et al. [13] does not show significant cost-effectiveness of a community based nurse led model of care compared to a hospital based rheumatologist led service, which was associated with no significant difference in clinical outcomes; in keeping with this, the Kings Fund report highlights that the benefits of community services relate predominantly to quality of care, rather than cost. Gruen, et al. [14] performed a systematic review of specialist outreach clinics in primary care and rural hospital settings internationally and demonstrated that although simple shifted outpatients models of specialist outreach improved patient access, no benefit was noted to health outcomes; specialist outreach as part of more complex multifaceted interventions involving collaboration with primary care, education or other services, however, demonstrated improved health outcomes, more efficient and guideline consistent care and less use of inpatient services.
Although the cost effectiveness of the community based model compared to hospital based services remains under evaluation, services thus far demonstrate reassuring satisfaction feedback from both patients and healthcare providers. With regards to patient choice of clinic location, patients living in more rural settings and those who are older or with more debilitating disease are likely to prefer local follow-up and, as such, services need to be set up with a population health based approach. For these services to thrive, funding of adequate community modalities and infrastructure is vital and, if shown to be cost-effective, this care delivery model is likely to be the future of rheumatology care for clinically stable patients. One factor that needs to be taken into consideration is the requirement for community training posts to ensure long term success for this model. Patients who have more complex care needs, for example those with complicated systemic disease or extensive comorbidities, are likely to benefit more from a hospital based review. For both of these models, future health services research is needed to evaluate disease outcomes, health economics and patient satisfaction to allow policymakers to make informed decisions regarding appropriate local services.
2. Lorig K, Ritter PL and Plant K. A disease-specific self-help program compared with a generalized chronic disease self-help program for arthritis patients (2005) Arthritis Rheum 53: 950-957. https://doi.org/10.1002/art.21604
3. Lorig KR, Ritter PL, Laurent DD and Plant K. The internet based arthritis self-management program: a one-year randomized trial for patients with arthritis or fibromyalgia (2008) Arthritis Rheum 59: 1009-1017. https://doi.org/10.1002/art.23817
4. Briggs AM, Towler SCB, Speerin R and March LM. Models of care for musculoskeletal health in Australia: now more than ever to drive evidence into health policy and practice (2014) J compilation 38: 401-405. http://dx.doi.org/10.1071/AH14032
5. Chew L and Yee SL. The rheumatology monitoring clinic in singapore-a novel advanced practice nurse-/pharmacist-led clinic (2013) Proceedings Singapore Healthcare 22: 48-55. https://doi.org/10.1177/201010581302200108
7. Modality Partnership: Rheumatology.
8. Shropshire Community Health NHS Trust: Community rheumatology.
10. Thompson J, Yoward S and Dawson P. The role of physiotherapy extended scope practitioners in musculoskeletal care with focus on decision making and clinical outcomes: A systematic review of quantitative and qualitative research (2017) Musculoskeletal care 15: 91-103. https://doi.org/10.1002/msc.1152
11. Abdelhamid AS, Mooney J, Walker AA, Barton G, MacGregor AJ et al. An evaluation of rheumatology practitioner outreach clinics: a qualitative study (2012) BMC Health Ser Res 12: 1-7. https://doi.org/10.1186/1472-6963-12-119
12. Hill J and Thorpe R. Outcomes for patients with RA: a rheumatology nurse practitioner clinic compared to standard outpatient care (2003) Musculoskeletal care 1: 5-20. https://doi.org/10.1002/msc.35
13. Watts RA, Mooney J, Barton G, MacGregor AJ, Shepstone L et al. The outcome and cost-effectiveness of nurse-led care in the community for people with rheumatoid arthritis: a non-randomised pragmatic study (2015) BMJ Open 5: 1-8. https://doi.org/10.1136/bmjopen-2015-007696
14. Gruen RL, Weeramanthri TS, Knight SE and Bailie RS. Specialist outreach clinics in primary care and rural hospital settings (2004) Cochrane Data Sys Rev 1. https://doi.org/10.1002/14651858.CD003798
Jethwa H, Department of Rheumatology, Chelsea and Westminster Hospital, United Kingdom, E mail: hannahjethwa@nhs.net
Jethwa H and Abraham S. Rheumatology - a qualitative review of community and hospital based delivery models (2019) Rheumatic dis treatment J 1: 03-05.
Rheumatology, Orthopaedics, Physiotherapists, Mental stress management, Osteoarthritis, Rheumatoid Arthritis, musculoskeletal disease.


