Introduction
Perinatal mortality is one of the indicators of poor
obstetric. The most common fetal conditions that lead to perinatal death
include congenital anomalies, Intra Uterine Growth Restriction and sepsis [1]. Birth
outcomes are measures of health at birth. Birth outcomes have improved
dramatically worldwide in the past 40 years. Yet there is still a large gap between the outcomes in developing and
developed countries. Adverse birth outcomes such as stillbirth, low
birth weight and preterm birth constituted
the highest rates of all the adverse pregnancy outcomes and are common in
developing countries [2].
Complications of preterm birth also
outrank all other causes as the worlds number one killer of young children.
Complications from preterm
birth caused nearly 1.1 million of the 6.3 million deaths of children under
age 5 in 2013. Of those more than 3,000 children under throughout
the world, approximately 210 million women become pregnant and over 135 million
of them deliver live born infants, while 75 million pregnancies end in stillbirth,
preterm or spontaneous or induced abortion. We estimate that 2·6 million babies
were stillborn in 2015, affecting women and their families in all settings. 98%
were in low-income and middle-income countries, over two-thirds were in
sub-Saharan Africa and southern Asia [3].
Birth outcomes are measures of
health at birth. Birth outcomes have improved dramatically worldwide in the
past 40 years. Yet there is still a large gap between the outcomes in
developing and developed countries. Adverse birth outcomes such as stillbirth,
low birth weight and preterm birth constituted the highest rates of all the
adverse pregnancy outcomes and are common in developing countries [4].
The birth-weight of an infant is
the single most important determinant of newborn survival; Neonatal
illness in general is closely related to low birth-weight. Some
epidemiological observations revealed that infants born under-weight (less than
2500gram) are approximately 20 times more likely to die than heavier babies [5].
Stillbirth rate is an important indicator of
access to and quality of antenatal and delivery care. Over 2.6 million
stillbirths ≥ 28 weeks of gestation or 1000 g occur each year worldwide. 98%
were in low-income and middle-income countries, of which over two-thirds were
in sub-Saharan Africa and southern Asia [9,10].
Different studies showed that inter-pregnancy intervals one of the
determinant factors for preterm birth, low birth weight, small for gestational
age births and stillbirth [12].
In Ethiopia, 20% of non-first births occur less
than 24 months after the preceding birth, with 8% occurring less than 18 months
after the preceding birth. About 43% of women give birth at least 36 months
after the previous birth [13]. Knowing the associated factors to adverse
perinatal outcomes (prematurity, low birth-weight and stillbirth) will help the
primary prevention employed against it to be easy, safe and cost effective.
Therefore, this study aimed to assess the adverse perinatal outcome and associated
among factors among delivered
mothers in Dessie referral hospital.
Method
and Materials
Study
design, area and period
Institutional based cross
sectional study was deployed. The study was conducted at Dessie referral
hospital in Dessie administrative town, south Wollo zone. Dessie town is one of
the eleven zones in Amhara Region North east Ethiopia and the city of the South
Wollo Zone which is located at a distance of 401 km from Addis Ababa and at 488
km from Bahir Dar. Dessie referral hospital serves about 8 million catchment
populations. The hospital has different departments and obstetric ward is the
one that serves around 1500 clients per year. The ward has 31 beds and 25
staffs. The study was conducted from February 30-March 30, 2017. All deliveries in Dessie referral hospital
were the source population and all deliveries in Dessie referral hospital
during the study period were the study population. All deliveries with
gestational age of 28 weeks or more during study period were included in the study
and those critically sick mothers who cannot respond during data collection
were excluded from the study.
Sample size determination and
procedure
Sample size was determined by
using a single population proportion formula by considering the assumption Zα/2
= critical value for normal distribution at 95% confidence level which equals
to 1.96 (z value at α =0.05), P (Estimated proportion) = 24.5% is taken from
previous study conducted at Hosanna hospital (31), d (margin of error) = 0.04
and 10% non-response rate. A total of 462 sample size was determined. To ensure
the adequacy of sample size, Epi-info was used to calculate sample size for
factors associated adverse birth outcome. Then the maximum sample size 462 was
taken. Dessie referral hospital was selected purposively serving north east
Ethiopia and all mothers who were eligible to the study included in the study
consecutively until we achieve the required sample size by considering the
assumption client flow at health facility is random by itself.
Data
collection Material, procedure and quality control
Structured pretested interview
questionnaire adopted from different literatures and prepared in the context of
the local situation and the aim of the study. Questionnaire translated from
English to local Amharic language and back to English to make it consistent.
Data was collected primarily from laboring mothers admitted to Dessie referral
hospital in the study period. Data collectors were trained integrated essential
emergency surgery first year students and 2 health officers supervisors were
also recruited. One day training was given to the data collectors regarding the
data collection procedure; timing of data collection and organization of
questionnaire. The quality of data was assured by doing pre-test on five
percent of total sample or 23 delivering mothers from Borumeda hospital. Clear
explanation of the study objective was given to the study participants. Regular
supervision and follow up was made by principal investigator. In addition,
regular check-up for completeness and consistency of the data was made on daily
basis and checking of questionnaire consistency was made. Incomplete
questionnaires was discarded and considered as none response rate.
Perinatal
deaths: Pregnancy losses
occurring after seven completed months of gestation (stillbirths) plus deaths to live births
within the first seven days of life (early neonatal deaths).
Live
birth: The complete expulsion or extraction of the
product of conception from the mother, regardless of the duration of pregnancy,
which after such a separation, breathes or shows other evidence of life (e.g.
Beating of the heart, pulsation of the umbilical cord or definite movements of
the involuntary muscles) whether or not the cord has been cut or placenta
detached.
Mature
infant: Infant born after 37 completed weeks of
gestation up until 42 completed weeks of gestation.
Premature
infant: One with a gestational age of 28 weeks to less
than 37weeks.
Low
birth weight: Any infant weighing less than 2500 grams at
birth.
Fetal
death (Still birth): The absence of signs of life at birth.
Abortion:
Fetus removed or expelled from the uterus in 28 weeks or less and
weighing less than 500 gram.
Last menstrual period: The date of the
starting of last menstruation the women had to the index pregnancy.
Adverse
birth outcomes: Women had at least one of the following still
birth, low birth weight, preterm
labor, and congenital anomaly of the baby.
Data
processing and analysis
The collected data was checked;
coded and entered to Epi info 3.5 and exported to SPSS version 21 for further
analysis. Univar ate analysis like frequency; table; mean and graphs were used
to present descriptive statistics variables. Bivariable logistic regression
model used to determine the independent association of dependent and
independent variables on the bases of COR; 95 percent of CI and significance
level of 0.2. Those variables which have significance level of less than 0.2
were transferred to multivariable logistic regression. Multivariable logistic
regression was also used to control the possible effects of confounder
variables on the basis of AOR; 95 percent of CI and 0.05 significance level was
taken as significance predictors.
Results
Characteristics
of Participants
A total of 462 women with 100% of
response rate were involved in the study of which 328(71%) were in the age
group of 20-34, followed by 68(14.7%) with mean age of 27 years and standard
deviation of 6.1. Majority of the mothers 438(94.8%) were married, and
321(69.5%) were urban residents. Regarding educational status, 123(26.6%) had
secondary school education and above, while 108(23.4%) primary school and. 284
women (61.5%) mothers were followers of
Muslim and 159(34.4%) were Orthodox Christians [Table 1].
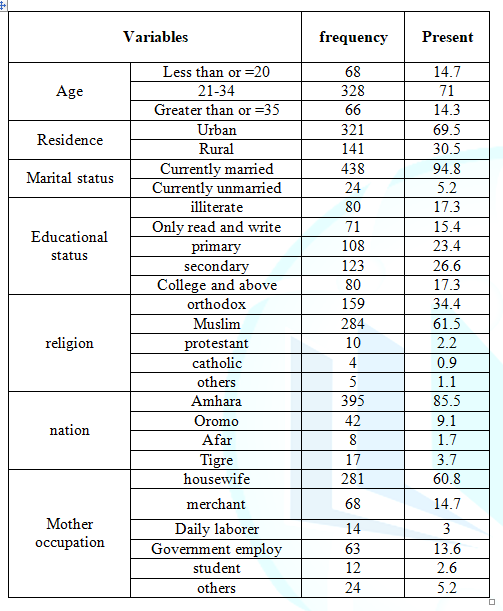
Table 1: The Socio-demographic Characteristics of women
attended labor ward in Dessie referral hospital; Dessie, Ethiopia.
Pregnancy
and labor related factors
From all participants, 174
(37.7%) mothers encountered complications during recent pregnancy. Common
complications reported by participants were Pregnancy induced hypertension78
(44.8%) followed by premature rupture of membren33 (19%), Antepartum hemorrhage
30(17.2%), poly hydraminous 19(10.9%) and others 14(8%). Among all deliveries
97 (21%) had experienced complications. From all deliveries 161 (34.8%)
neonates had Apgar score less than 7.This study indicates 322 (69.5%)
participants were referred from health centers and from all study participants
97(21%) were encountered labor complication. The common labor complications
were prolonged labor 73 (15.8%) followed by Malposition 15 (15%) and others 14
(14.4%). Among study participants 414(89.6%) had antenatal care follow up and
160(38.6%) had four and below four antenatal care visits.
Medical
and obstetric related factors
Among the study participants, 294 (63.6%) were multi-gravidas, 229
(77.9%) had greater than 23 months inter pregnancy interval 274 (83.8%) had antenatal care follow up and
322 (69.7%) had iron and folic acid supplement . majority of 372(80.5%) had
hemoglobin level greater than 11gm/dl, 296(64.5%) mothers had middle upper arm
circumference greater than 23cm ,
394(85.3%) had no previous still birth , majority of respondents 376(81.4%) had
used family planning [Table 2].

Table 2: Medical and obstetric related factors women attended labor ward during
the study period in Dessie referral hospital; Dessie, Ethiopia.
Proportion of adverse birth outcomes
The study finding showed that the
prevalence of adverse birth outcome among the study participants was
150(32.5%). Out of 150 adverse
birth outcomes the commonest in this study was low birth weight 60(40%)
followed by preterm delivery 52(35%) [Figure 1].
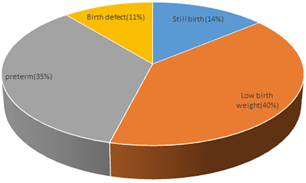
Figure 1: Common adverse
birth outcomes among delivered mothers in Dessie referral hospital, north east
Ethiopia in 2017.
Factors
associated with adverse birth outcome
This study result showed Hemoglobin less than 11gm/dl, Middle
upper arm circumference less than 23 cm,
do not had antenatal care follow up, Have chronic medical illness, Having current pregnancy
complication and Duration of labor more than 24 hours were important predictor
factors for adverse birth outcome.
Mothers who didnt attend antenatal care were 4 times
more likely to have adverse birth outcome when compared to those who attended
antenatal care follow up, [AOR=4.01, 95% CI (2.8,8.3 )]. Similarly, mothers
with hemoglobin level less than 11 mg/dl were encountered adverse birth
outcomes 3 times more when compared to those with hemoglobin level greater or
equal to 11 mg/dl [AOR=3.04, 95% CI(1.62, 5.71)]. The presence of any form of pregnancy
complication to current pregnancy were 3 times more likely to result in adverse
birth outcomes [AOR=2.9, 95% CI (1.64, 5.15)].
Furthermore, mothers whose MUAC less
than 23cm encounter adverse birth outcome 3 times when compared with MUAC
greater than or equal to 23cm [AOR=2.8, 95% CI (1.62-4.87)].
Participants who
had chronic medical illness were three times more likely to result in adverse
birth outcome [AOR=3.37, 95% CI (1.17-6.63)].
Discussion
This
study finding showed that the prevalence of adverse birth outcome among the
study participants was (32.5%). Out of study participants (14%) were still
birth, (40%) were LBW, (35%) preterm and (11%) were with visible birth defects.
Among babies with congenital malformations 20 were still births. These
figures were higher than the findings of Tanzania [14], and Ghana [15]. In
which 18%, 19% had experienced adverse birth outcomes respectively. And also
this figure were higher than the finding of Negest Elene Mohammed Memorial
General Hospital in Hosanna Town, SNNPR, Ethiopia 24.5 %( 16). The variations between the findings may be
attributable to variations in quality of maternal health services, facility and
logistic parameters in respective study areas.
Mothers with complication in recent
pregnancies were found to have higher odds of experiencing adverse birth outcomes
(preterm births, low birth weight still birth and visible birth defect) than
those without the complications. This finding was consistent with the study
done in china (24), Iran (25), Pakistan (26), and Gambia (27). The link may be
explained in terms of the fact that the complications that have occurred during
pregnancy have affected the well-being of the fetus in the uterus.
In this study, we assessed the
prevalence and associated factors of adverse birth outcomes (still birth,
preterm birth, low birth weight, visible birth defect) among deliveries at
dessie referral hospital. The prevalence of still birth was 82 per 1,000 total
births. It is also higher than the previous reports from hosanna, Gondar,
Ethiopia, Tanzania and a systemic review for sub-Saharan African studies where
the prevalence of still birth ranged from 27- 33/1,000 total births (14, 17,
and 16). Methodological and socio-economic variations explain differences in
adverse birth outcomes (29) this result is higher than with other result. This may be most normal deliveries take place
in health centers while more complicated ones are referred to the tertiary
hospital contributing to higher rates of adverse birth outcomes at referral
hospitals. Moreover, women who experienced obstetric complications are likely
to show up to health facilities and may get referred to hospitals; higher rates
of adverse birth outcomes may exist at referral hospitals.
The prevalence of preterm in this research was
15.2%.this result is higher than researches done in Tanzania 12%, Gondar,
Ethiopia 14.3% and Iran 5.1%. It associated with Clients with pregnancy
complications (pregnancy induced hypertension, Antepartum hemorrhage, premature
rupture of fetal membranes, and poly hydramnious (14, 17, and 25). This
difference may be due to methodological and population variation on top of the
socio economic and set up differences.
Women with hemoglobin level less
than 11 mg/dl were also found to experience adverse birth outcomes when
compared with those with Hgb level greater than 11 gm./dl. The finding was
consistent with studies conducted in Pakistan (26), Tanzania (14), and Nigeria
(29) and in Ethiopia (16). The reason could be linked to the effect of anemia on the oxygen
bearing capacity and its transportation to the placental site for the fetus.
In this study, pregnancy
complication also was found to be independent risk factors for adverse birth
outcomes such as preterm birth which is in agreement with a study conducted in
Gondar, Ethiopia [17]. This might be related to termination of pregnancy as a
result of medical
disorders of pregnancy like pre-eclampsia and other obstetrical problems.
In these finding mothers with MUAC less than 23cm were also found to experience
adverse birth outcomes when compared with those with MUAC greater than 23cm
this result is in agreement with the result in Bangladesh (27).
The prevalence of low birth
weight in this study was 16.7% this was higher than the previous findings of
Tanzania 8%, Ethiopia 9.8%. This increment might be due to poor nutritional
status and early termination of pregnancy in other comorbidities.
In multivariate analysis, women
who did not have ANC follow up were more likely to have adverse out comes.
During ANC follow up women will have access to information related to nutrition
and danger signs of pregnancy. Regular ANC follow up will also help a pregnant
woman seek early treatment for her potential pregnancy related problems but if
failed to showed up for ANC, she will be disadvantaged . This finding is in
line with previous studies in Nigeria (28) and Ethiopia (29).
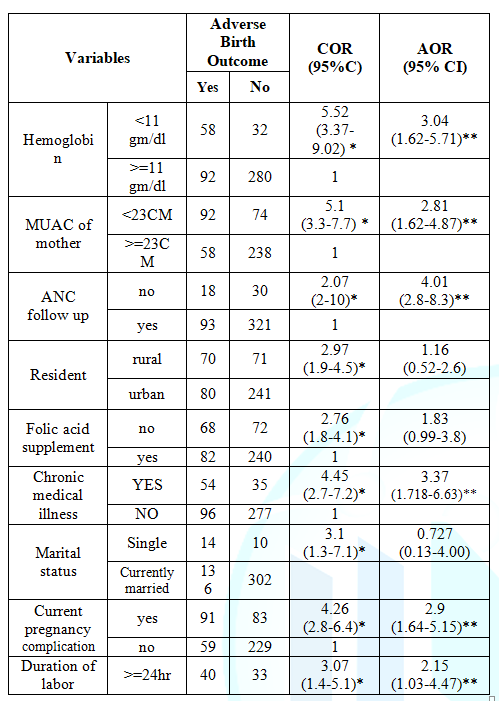
Table
3: Bivariate and multivariate analysis factors
associated with adverse birth outcomes among delivered mothers in Dessie
referral hospital, north east Ethiopia, 2017. 1reference *p<0.05
**p<0.01
In multivariate analysis, women
with duration of labor greater than 24hr were more likely to have adverse birth
outcome when we compare women with duration of labor less than 24hr. this might
be due to when the labor prolongs the fetus may be at risk for aspiration and fetal heart beat
abnormalities.
Conclusion
The magnitude of adverse birth outcome
in this research was high and from the adverse birth outcomes low birth weight
and preterm delivery covers the highest. Antenatal care follow
up, Middle upper arm circumference, hemoglobin level, chronic medical illness
and current labor complication were significantly associated with adverse birth
outcome.
Recommendations
Minister
of health
Strategies and policies should
focus on prevention and control of chronic disease through primary health care
system and community participation.
South
Wollo Zone health department
Despite high ANC follow up rate
there is still high proportion of adverse birth outcome. Supportive
supervisions should be provided for health professional working in antenatal care clinic
and labor & delivery ward to increase their capacity for identifying and
managing associated factor and labor complication for adverse birth
outcome.
For
Dessie referral hospital
Strength formal referral linkage
with peripheral health facilities to prevent long duration of labour.
Health
professionals
Awareness creation on
supplementation and proper taking of
Iron and folic acid supplementation based on the standard guideline for
all pregnant mothers. Besides this focus on early detection of complications
with appropriate action should be taken before the labor prolonged.
For
researchers
Additional investigation should
be conducted on quality of antenatal care, delivery and post-natal care at
health facilities and traditional pregnancy care practices in the community.
Ethical
Approval
Ethical approval obtained from
wollo university- medical faculty. Permission was obtained from head of Dessie
referral hospital. To ensure confidentiality interview was held in private.
Confidentiality was ensured throughout the process. Advice was given for
mothers with deliveries of adverse birth outcomes. Verbal consent was taken
from selected participant to confirm willingness to participate in the study
they have got full information what to do next to their baby if found being
under weight and premature. Vaccination to the
baby and birth control methods for the mother was given.
Financial
Disclosure: Wollo University was funded the
research. The funders had no role in study design, data collection and
analysis, decision to publish, or preparation of the manuscript.
Acknowledgment:
First, we would like to acknowledge to Wollo
University, College medicine and health Sciences,
department of Public Health for funding
this research. First of all, thanks to almighty God for giving us this
remarkable time and patience to start and finished our work. We also express
our heartfelt gratitude to data collectors and respondents.
References
1. Behrman et al. Nelson text book of
pediatrics (2004) Saunders 17th edition
2. Blencowe, Hannah Cousens, Simon Jassir, Fiorella
Bianchi Say, Lale Chou, et al. National, regional, and worldwide estimates of
stillbirth rates in 2015, with trends from 2000: a systematic analysis (2016)
The Lancet Global Health 4: 98.
3. Augustin Conde-Agudelo, Jose M Belizan,
Maureen H Norton, Anyeli Rosas – Bermudez. Effect of inter pregnancy interval
on perinatal outcomes in Latin America (2005) Obstertrics and gynecology 106:
359-366
4. Howson CP, Kinney MV, Lawn JE PMNCH (2012)
Save the Children. Born Too Soon: The Global Action Report on Preterm Birth,
WHO, Geneva.
5. UNCIEF, WHO. Low birth weight country,
regional and global estimates (2010) Executive Summary. New York, USA.
7. March of Dimes Quick Reference Fact Sheets
(2009) Low Birth Weight.
8. March of Dimes Preterm-Birth Complications
Leading Global Killer of Young Children (2014) Health Day News.
9. Martin JA, Niemeyer S, Oysterman M,
Shepherd RA Born a Bit Too Early: Recent Trends in Late Preterm Births (2009)
National Center for Health Statistics 24: 71-78.
10. Lawn JE, Blencowe H, Pattinson R, et al.
Stillbirths: Where? When? Why? How to make the data count (2011) Lancet 377:
1448.
11. Cousens S, Blencowe H, Stanton C, et al.
National, regional, and worldwide estimates of stillbirth rates in 2009 with trends since 1995: a systematic
analysis (2011) Lancet 377: 1319.
12. Lale Say and et al. The prevalence of still
Births. A systematic review (2006) Reproductive health 3:1
13. Augustin Conde-Agudelo, Anyeli Rosas –
Bermudez, Ana Cecilia Kafury-Goeta. Birth spacing and risk of adverse perinatal
outcomes. A meta-Analysis (2006) JAMA 295: 1809-1823.
14. Demographic and health survey, Ethiopia,
Central statistics Agency- Addis Ababa (2011) Ethiopia and ORC marco,
Calverton, Maryland, USA.
15. Deborah W.
Adverse birth outcomes in United Republic of Tanzania Impact and
prevention of maternal risk factors (2007) Bulletin of the WHO 85: 9-18.
16. Abdo RA, Endalemaw TB and Tesso FY. Prevalence and associated Factors of Adverse
Birth Outcomes among Women Attended Maternity Ward at Negest Elene Mohammed
Memorial General Hospital in Hosanna Town, SNNPR (2016) Ethiopia 5: 15.
17. Adane AA, Ayele TA, Ararsa LG, Bitew BD,
Zeleke BM. Adverse birth outcomes among deliveries at Gondar University
Hospital (2015) 2: 1-9.
18. CDC, International notes update (1984)
Incidence of low birth weight 33 (32).
19. F. Gary Cunninghamand et.al. Williams
Obstetrics (2005) McGraw hill 24th edition.
20. Alan H, De Cherney, Martin L Pernoll. Current
Obstetrics and gynecology (2013) McGraw hill 11th edition.
21. Juliana C. Adverse pregnancy outcomes and
maternal urban or rural residence at birth (2016) J Obstet Gynaeco 42: 496-504.
22. Cecatti JG, Correa-Silva EPB, Milanez H. The
Associations between Inter-pregnancy Interval and Maternal and Neonatal
Outcomes in Brazil (2008) Maternal Child Health J 12: 275-281.
23. Chen Y, Li G, Ruan Y, Zou L, Wang X, et
al. An epidemiological survey on low
birth weight infants in China and analysis of outcomes of full-term low birth
weight infants (2013) BMC Pregnancy Childbirth 13: 242.
24. Alijahan R, Hazrati S, Mirzarahimi M,
Pourfarzi F, Hadi PA, et al. Prevalence and Risk factors associated with
preterm birth in Ardabil, Iran (2014) Iran J Reprod Med 12: 47-56.
25. Bakhtiar UJ, Khan Y, Nasar R. Relationship
between maternal hemoglobin and perinatal outcome (2007) Rawal Med 32: 102-104.
26. Hossain N, Khan N, Khan NH. Obstetric causes
of stillbirth at low socioeconomic settings (2009) JPMA 59: 744-747.
27. Agarwal A, Agrawal VK, Agrawal P, Chaudhary
V. Prevalence and determinants of “low birth weight” among institutional
deliveries (2011) Ann Nigerian Med 15: 48-52.
28. Siza JE.
Risk factors associated with low birth weight of neonates among pregnant
women attending a referral hospital in northern Tanzania (2008) J Health Res
10: 1-8.
29.Jammeh A, Sundby J, Vangen S.Maternal and obstetric risk factors for low
birth weight and preterm birth in rural Gambia: a hospital-based study (2011)
Open J Obstet Gynecol 1: 94-103.
*Corresponding author
Niguss Cherie, Department of Public Health, Wollo University, Ethiopia, E-mail: nigucheru@gmail.com
Citation
Cherie N, Mebratu A. Adverse Birth Out Comes and Associated Factors among Delivered Mothers in Dessie Referral Hospital,
North East Ethiopia (2018) Nursing and Health Care 3: 1-6



