Introduction
The cultural aspects of care are
crucial for nursing curricula in addressing the holistic needs of patients [1,2].
In the Sultanate of Oman, the expansion of the Ministry
of Healths (MoH) healthcare facilities and services, combined with the
Omanization policy, has led to an increased need for well-trained national
(Omani) healthcare professionals [3]. In response to this need, Ministry of
Health Educational Institutes (MoHEIs) were established and designed nursing
and allied health disciplines educational programs in support of its national
health policy. The MoH proclaims that the MoHEIs programs were designed to
emphasize culture, family, community, and the healthcare system.
There are several challenges
faced by nursing
education in the Gulf Cooperation Council (GCC) countries, including Oman.
The nursing curriculums are founded on the Western model of nursing education.
This is due to the lack of an alternative regional healthcare model and the
limited number of Arabic nursing textbooks [4]. The adoption of Western-based
nursing models often conflicts with local cultural values and beliefs [5,6]. The majority
of the nursing faculty is expatriates who originate from diverse cultural and linguistic
backgrounds, such as India, Philippines, Jordan,
Egypt, South Africa, and United Kingdom. With the prevailing view that nursing
is a technical and low-level profession, the social
image of nursing in the Gulf Cooperative Council (GCC) countries, including
Oman, remains negative [7]. Nurses in Oman are simply seen as a doctors assistant
[8]. These viewpoints, when combined with a social preference for prestigious
academic fields of study and a lack of family support, have resulted in a lack
of awareness regarding nursing as a career choice in Oman [9].
Literature
Review
“Good care” is a culturally-based
phenomenon [10]. While caring for patients, nurses may project their own
culturally based values onto them who might come from backgrounds different to
their own [11 ]. To address this
issue, several cultural competence models have been developed. These include [12]
culture-based care requires proper communication skills, which are vital to
building a strong nurse-patient
relationship [13]. Culture
is an important concept for individuals and communities as it shapes the way
health, illness, and quality of life are perceived [14]. Leininger
the founder of the movement, defined culture as “the learned and transmitted
values, beliefs, and practices that provided a critical means to establish
culture care patterns from the people” (pg. 91). Yet, this definition by
Leininger seems to ignore the culture of the nurse in the relationship and
assumes that increased knowledge and understanding of other cultures would lead
to tolerance, respect, and cause prejudiced behaviors to change [15,16]. In
addition, this definition seems to promote the idea of “us versus them”, which
may lead to discrimination. The culture care construct is a holistic
perspective that involves a cognitively learned, conveyed professional and native
values, beliefs, and ways of life [17]. Numerous authors emphasize that it is
crucial for a healthcare system to respond to patients cultural values,
beliefs, and traditions [18-21]. Culturally congruent care is that care which
is tailored for compatibility with the patients own values, beliefs,
traditions, practices, and lifestyle [22]. Therefore, the inclusion of cultural
competence in nursing education programs would provide student nurses with the
knowledge and skills necessary to serve culturally
diverse patients [23]. Indeed, as Omani people are adamant in preserving
their cultural traditions and customs, Omani nurses must understand and work
effectively within this cultural context. Therefore, it is vital that the
nursing programs prepare student nurses to understand the key concerns and
emerging challenges faced by healthcare service users and professionals within
a cultural context to provide effective, competent care.
Central Concepts
Curriculum
Any curriculum is based on the
educational philosophy of its developers; therefore, it represents the
developers values and beliefs concerning the acquisition of knowledge. When
designing an educational program, the developer must also incorporate the
philosophical values and beliefs of the educational
institution and its views on learning. According to Lawton [24], curriculum
is essential and is a selection from a societal culture. This includes aspects
of the culture or societys way of life, knowledge, attitudes, and values
perceived as important. Therefore, the transmission of these aspects to the
next generation should be entrusted to specially-trained
professionals (educators).
Professionalism
A profession is determined by
certain identified work standards, a body of knowledge, and an established
codes of ethics. Professionals are generally defined in terms of a specific
body of knowledge obtained through formal education, an expanded level of
skills, certification to verify entry to the profession, and a set of
behavioral norms known as “professionalism” [25]. Professionalism indicates
attitudes that represent high levels of identification with and commitment to a
specific profession. Attributes of professionalism include educational
preparation, research, scholarship, participation in professional
organizations, and community
service. Using theory to maintain competence in the field and abiding by
the code of nursing ethics are all part of professionalism. In the area of
nursing, professionalism is focused on the expansion of the role of nursing in
a rapidly evolving healthcare setting. The healthcare system is constantly
changing due to societal needs, service-user demands, government policies,
technological developments, and economical pressures. The development of high-quality
nursing care should incorporate these cultural changes into their
educational programs. To enhance public perception, nursing must reflect the
level of professionalism as presented in other professions.
Study
Questions
1. How do the MoHs approaches to the
nursing curriculum impact nursing education in the Sultanate of Oman?
2. How culturally congruent is the
MoHs nursing curriculum?
Methods
This is a qualitative
multiple-case research design which will investigate whether Omans nursing
curriculum adequately addresses cultural congruency [26,27]. The investigator
used educational policies, semi-structured individual interviews and focus
group interviews to collect data. Using purposeful sampling, nursing education
decision-makers, educators, students, and service users (public) were
interviewed over a 6-month period (Table
1 and Figure 1). The participants inclusion criteria were nursing
administrators, nursing
educators, nursing students, service users or the public.
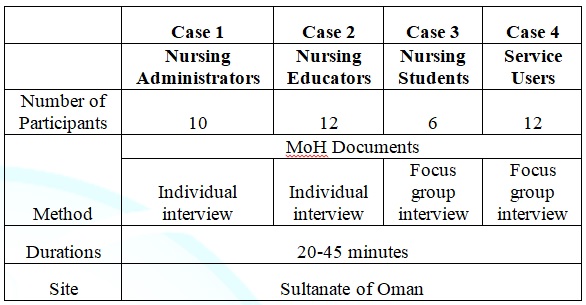
Table
1: Data Collection Schedule.

Figure
1: Recruitment
Sites.
Ethical
Considerations
Approval was obtained from the
Medical and Health Science Ethics Committee at the University of Nottingham and
the MoH Research and Ethical Review Committee of the Sultanate of Oman.
Data
collection methods
1. Documents: Nine relevant
documents were identified. These include the Directorate General of Human
Resources Development (DGHRD) mission/vision/objectives, curriculum
competences, the nursing programme, foundation programme, Omani midwifery
and nursing council codes of ethics, the student handbook, the MoHs
five-year plan, MoH mission/vision/objectives, and MoH patient satisfaction
surveys.
2. Semi-structured interviews: The
interview guide was founded on Lawtons cultural analysis model, which is based
upon the assumption that the main purpose of a curriculum is to initiate
learners into the cultural heritage of society. With cultural analysis applied
to nursing education, the following questions were asked: What is the status of
nursing education? In what ways is the nursing education provision developed?
How do members of the profession wish to see nursing education develop? What
kind of values and principles will be involved in deciding how nursing education
should develop? and How should future nursing graduates prepare for their role?
Data Analysis
All
data were initially collected and recorded in either English or Arabic, with
the Arabic sequentially being translated into English. All recoded
interviews with their transcripts were reviewed for any inconsistencies. Using
Ritchie and Spencers [28] framework analysis, the
data was analyzed with a case-within and cross-case approach. This analysis
consists of five stages: familiarizing, identifying a thematic framework,
indexing, charting, and mapping and interpretation (Figure 2, Tables 2 and 3).
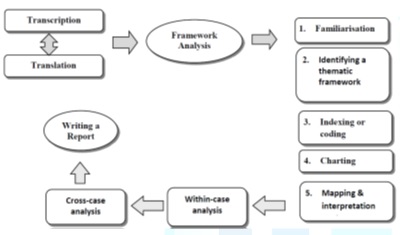
Figure
2: Phases of
qualitative multiple case study analysis.
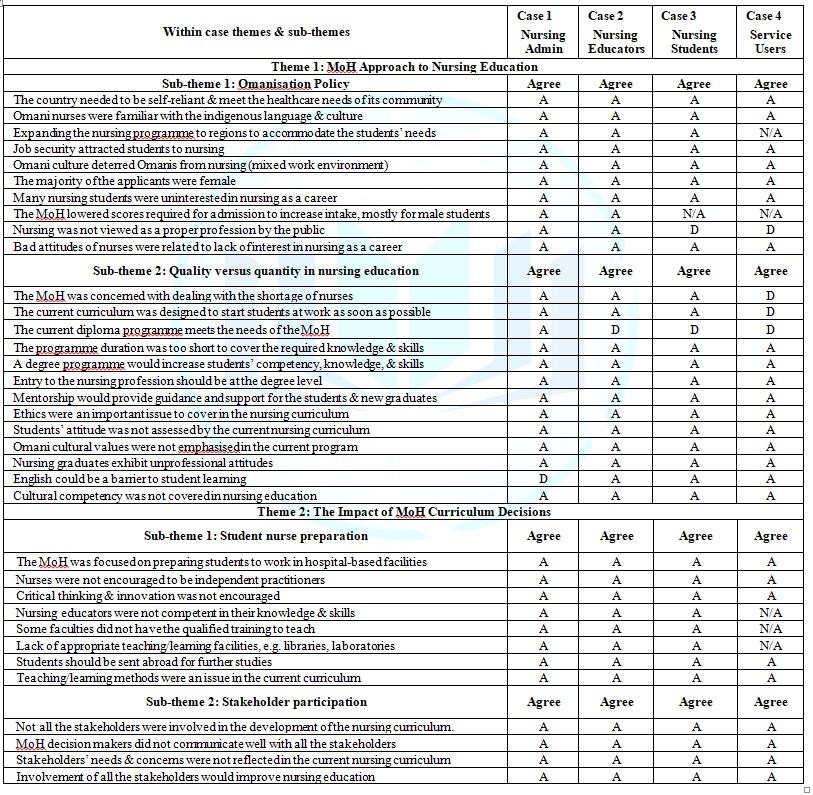
Table 2: Within-case themes
and sub-themes from the four cases.
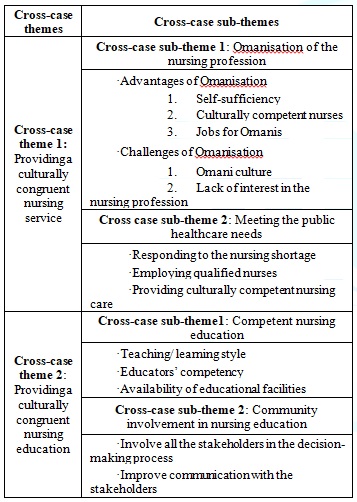
Table 3: The generated
cross-case themes and sub-themes across the four cases.
Reflexivity
As the researcher is the primary
who collected and analyzed the data, reflexivity is essential [27,29].
According to Patton [30] reflexivity allows the researcher to be aware of not
only the cultural, political, social, linguistic, and ideological origins of
their own assumptions but also the viewpoints of the study participants. It is
important that the researcher is aware of their own personal assumptions and
beliefs throughout the study [27,29]. Field notes were incorporated into the
charting and indexing of codes and themes, which enabled the investigator to
track theoretical perspectives, assumptions, and emotional reactions.
Results
and Discussion
Meeting
the healthcare needs
When examining the data, several
themes emerged. These emerging themes included whether the nursing curriculum
was meeting the needs of Oman. The study revealed that the MoH nursing
curriculum was intended to educate future nurses needed to fill expanding
healthcare facilities. Along with biomedical support courses such as
anatomy and physiology, biochemistry, and nutrition, the focus of the
curriculum is centered on core nursing courses. The findings support that the
MoH nursing curriculum is almost entirely nursing discipline-focused and is
purely to educate nurses who will be employed in the hospital setting.
An example statement is as
follows:
He the minister wanted to create
a cadre and have numbers and he was establishing new nursing institutes, so he
needed to fill the institutes, so that is a major problem here with nursing
education (Admin 5).
This is consistent with the
essentialist philosophy of education, which proclaims a philosophy that
focusses on the process of learning rather than the content of the curriculum.
Furthermore, the case study findings indicate that this approach has led to the
general belief that nursing education should be strictly discipline-focused and
rich in content. The findings suggest that the Omanization of nursing education
and practice is beneficial in Oman because it reduces the reliance on
expatriate nurses and lessens the cultural incongruences in healthcare services.
A culturally
congruent nursing education would facilitate nurses to provide patients
with care that is familiar, supportive, and meaningful within their cultural
context [1,31]. By excluding international nurses, the Omanization of nursing
may become so parochial and inward looking, resulting in a lack of cultural
diversity and mutuality. The main aim for Omanization of the nursing
profession is to minimize misunderstanding between the healthcare providers
and service users. However, the MoHs approach to nursing education only seems
to place emphasis on how many nurses are produced rather than the quality of
education. As one subject explains:
Repeating exams twice or more is
not appropriate if we want better nurses… we need a better, rigid system that
is able to filter graduates … we do not have to have 100 percent graduation, or
even 90 percent (Admin 9).
These findings are in accordance
with those of other studies, where all GCC countries have adopted policies
based on the beliefs that indigenous nurses are more suitable to care for the
population of clients within their own locals. These assumptions are based on
the belief that local nurses are best able to provide good quality nursing care
because they already understand the language and culture [32]. A study
conducted in Saudi Arabia highlighted the positive impact of healthcare
satisfaction and outcomes when Arabic language for communication is used. Not
only does using Arabic improve client satisfaction and outcomes, speaking in
Arabic decreases conflicts and miscommunication between healthcare
professionals and clients [33].
Therefore, language barriers
between the nurse and patient may result in miscommunication that could
negatively influence their relationship [34-36]. This failure to communicate
with healthcare providers not only creates a hurdle in accessing healthcare but
also challenges trust in the quality of the provided healthcare [37,38]. As
language is vital to how culture operates, even a nurses ability to speak a few
words and phrases of the patients language may increase trust by reducing
communication barriers [39].
Attitudes
and behaviors of nursing graduates
The
image of nursing as “a dirty job” posed a challenge for the MoH. It is believed
that the lack of interest in the nursing profession may be derived from this
poor image, or a lack of awareness of the professions vast opportunities. The nature
of nursing work with heavy workloads, long shifts, and holiday coverage
often clashes with the traditional Omani family lifestyle. Other factors such
as low wages, limited professional development, and absence of support for
working mothers are often stated as problematic to entering the profession [40].
These
challenges detriment the quality and type of applicants to the MoH nursing
programme. Participants commented as follows:
The
Omani culture still sees nursing as a low job and regards the mixed
(female/male) working environment as unfavourable, which means nursing is not
seen as a reputable profession, and this is the cause of the students bad
attitudes (Teacher 2).
There
are seven women in my family who are nurses… but still I did not think nursing
can be the career for me because of the long hours and different shifts. I saw
how hard they had to work (Nursing Student 3).
The
analysis of the data indicates that the current MoH nursing curriculum does not
address the negative impact of the poor image of nursing with the nursing
students which is echoed in their negative attitudes and behaviors toward
the nursing profession [41]. The poor image of nursing and the lack of interest
in nursing as a career is a global phenomenon that is not exclusive to Oman.
These findings correlate with several studies that address the image and
perceived status of the nursing profession [42-46]. According to a study by
Al-Omar [9] only 5.2% of a sample of high school students in Saudi Arabia
intended to pursue nursing after graduating secondary school. While, in
Tanzania, the nursing profession was the least popular of all allied health profession
that were indicated, with only 9% indicating an interest. This is consistent
with Fletchers study which states that most nurses do not hold a positive sense
of worth or think highly of themselves.
Despite,
the social image and professional status of nursing still being negative in
Oman and other GCC countries, there are certain emerging positive perceptions
of nursing profession in Oman. An example statement is as follows:
“Nursing
is a profession which makes us closer to Allah (God), because helping people in
need is a religious duty, and Allah rewards us when we help others in need”
Nursing Student
Assisting
a person in need is regarded as a religious duty and a way to be close to God
(Allah). Other studies positively suggest the nursing profession as a
“calling”. Other studies positively suggest that many students are driven to
select nursing from a desire to help others.
Caring:
An Omani perspective
The
current MoH nursing curriculum does not place emphasis on the concept of caring
as an essential value in nursing
education. The importance of prayer rituals in patient care were not part
of the nursing curriculum. The participants interpreted the concept of “caring”
to represent compassionate care and effective communication with patients and
their families. Participants interpretation of caring is attributed to their
cultural understanding of the meaning of care. Hence, they stressed that caring
involved respecting the spiritual and religious needs of the patients and their
families [35]. According to the study, patients appreciate the nurses caring
approach and presence more than their nursing knowledge and skills. Example
statements are as follows:
We
know for a fact… that we have a problem with our students attitude… and how
they approach and interact with patients in hospital when it comes to issues
such as confidentiality and the rights of the patients (Teacher 7).
Our
culture, as Arabs and Muslims… even without the code of ethics, we have the
code of ethics of our religion… our Islamic laws… which guide us in how to
behave and act… how to respect and listen to others (Admin 10).
In
general, the MoH healthcare
providers had no smile, no warmth, no care, no compassion… that is the problem
with the current healthcare…. no care in healthcare (Service User 8).
When
nurses try to display a caring attitude toward their patients, this positively
impacts the nurse–patient relationship [34,47]. In this study, the
characteristics of care involved being physically present with the patient,
conversing with the patient and employing active listening, avoiding prejudice,
maintaining confidentiality, flexibility in patient care, and optimism. In
Islam, caring is associated with the intention to be responsible, sensitive,
and concerned about others with the drive and commitment to act rightfully [48].
Therefore, caring in Islam is to understand what, when, who to care for, and
why [48]. The current MoH nursing curriculum defines the value of caring as a
continuous demonstration of feeling and exhibiting concern and empathy for
others, together with respect, fairness and transparency (MoH, 2008). This
definition of caring reflects the Western Judeo-Christian values and beliefs,
with a notion that nursing has a common value system [32,49-51]. This is very
problematic, as it does not help the graduate nurses or educator to make
culturally sensitive, appropriate decisions, actions, and innovations. Within
non-Western nursing educators, there is recent acknowledgement that while
nursing theory has universal aspects, differences in philosophy and culture
which are unique to each country need to be reflected in the nursing education
[34].
Teaching/learning
approaches
Due
to limited funding and duration of nursing
coursess, the nursing curriculum may not be able to include such things as
the caring aspects of nursing. Limited budget allotted for and the goals of the
MoH for nursing education often limit innovation in nursing education.
Furthermore, this study revealed that the nursing curriculum inflexibly hinders
the learning process. Therefore, many of the study participants viewed the
current curriculum to be ineffective in improving students learning
capabilities. Examples statements are as follows:
If
we pass the exam the teachers will say “good student”… but if we fail they will
only say the exam was easy and we told you everything coming in the exam… no
one cares about the quality of the student (Nursing Student 4).
I
believe the nurses are lacking the correct knowledge to deal with patients…
they do not care for the patients needs… some patients dislike coming to
hospitals (Service User 3).
These
viewpoints are in alignment with Bruners theory that uniform instruction will
not meet the needs of all learners, because everyone understands the world in
their own unique way. According to Bruner, learning is an active process in
which learners construct new ideas based upon their current or past knowledge
interacting with new information. Through this, the learner selects and
transforms information, constructs hypotheses, and makes decisions. Hence, the
learner “focuses on the how to learn, rather than what to learn”. However, the
findings revealed that the current nursing
curriculum guides nursing students to rely heavily on teachers lectures,
which limits the development of their critical thinking skills. Hence, the
findings acknowledge the need to move away from the teacher-centered approach
and toward a learner-centered process.
Educational
theorists have advocated to replace teacher-centered pedagogies with
learner-centered approaches. In teacher-centered approaches, judgements about
appropriate areas and methods of inquiry, legitimacy of information, and what
constitutes knowledge rest with the teacher. This often leads both students and
educators to resist switching to the learner-centered approach. There are
several factors contributing to this resistance [52]. Societys emphasis on
success leads students to avoid difficult work and to develop inflated perceptions
of their abilities. Traditionally, educators have taught according to the
students comfort level. Now, this is the norm that students expect. Others have
suggested that students and educators have low tolerances for challenges and
change [52].
Stakeholders
and nursing education
The study acknowledges that there
is limited stakeholder involvement in developing the MoH nursing curriculum and
lack of transparency in the decision-making process. According to the
participants, for the development of the nursing curriculum to reflect societal
needs, it should involve all stakeholders, including the community, students,
and teachers. The stakeholders also include the consumers of healthcare who are
well-positioned to contribute to decisions relating to the appropriate
qualities and skills required in graduate nurses. Stakeholders bring unique
perspectives to the process of development of the nursing curriculum. This
perspective arises from the ability of the stakeholders to discern
compassionate care as a direct result of their personal experiences.
This strength of this
multiple-case study is based on its originality in exploring the phenomena of
the cultural aspects of client care in the nursing curriculum in the Sultanate
of Oman. According to Eisenhardt, the multiple-case study approach pursues
phenomena that bring together multiple perceptions and experiences from a range
of various sources (documents and interviews). Additionally, the use of
purposive sampling in selecting study participants facilitated comparison and
contrast of the findings (cross-case analysis) of the four cases to develop a
framework for a culturally
congruent nursing curriculum.
This study was conducted in the
context of Oman, which limits the generalizability of the findings. However,
generalizability was never intended. Second, the pressures of political office
may have influenced the statements of the MoH nursing administrators.
Furthermore, non-Omani participants may have been cautious of making negative
statements against MoH policies and policymakers. Additionally, the focus group
participants may have been reluctant to make statements that were too negative
or critical of the MoH as an organization, due to their potential impact on the
dynamics of the group.
Conclusion
These findings illustrate that
there is minimal content in the nursing curriculum which addresses caring and
cultural competency. The current method of instructor-driven education needs to
give way to student-centered learning to truly develop the nursing students
critical thinking skills. Nursing
educators should critically examine their teaching strategies for teaching
the caring and transcultural components of nursing care. The interviewees
emphasized that cultural knowledge is a critical component to prepare nurses to
care for the increasingly diverse society. This increased understanding will
enable nurses to be more effective while providing care that is within the
cultural context of individuals, families, and communities from diverse
cultural backgrounds. However, this author acknowledges that there may be other
considerations such as a hidden curriculum agenda which might interfere with
the participants answers.
Future
Research
Further studies are recommended
on the cultural congruence of the nursing education/curriculum. Factors that
facilitate or hinder students cultural competency to make judgements and
decisions regarding nursing care issues in a multicultural world requires
additional investigation. Furthermore, an evaluation of the effectiveness of
the nursing curriculum after implementing the concepts of culture in nursing
education would be beneficial.
References
1.
Leininger
M. Culture care diversity & universality: A theory of nursing (1991)
National League for Nursing Press, New York, USA.
2.
Papadopoulos
I, Tilki M and Taylor G. Transcultural care: A guide for health care
professionals (1998) Quay Books, Dinton, Wiltshire, England.
3.
Randeree
K. Workforce nationalization in the gulf cooperation council states (2012) Center
for International and Regional Studies, Georgetown University, School of
Foreign Service in Qatar, Washington DC, USA.
4.
Al-Darazi
F. Women in nursing in Islamic societies (2003) N Bryant (Ed) Oxford University
Press, UK 175-87.
5.
Al-Shahri
M. Culturally sensitive caring for Saudi patients (2002) J Transcultural
Nursing 13: 133-138. https://doi.org/10.1177/104365960201300206
6.
Lovering
S. Saudi nurse leaders: Career choices and experiences (1996) Unpublished
Masters research report, Massey University, Palmerston North, New Zealand.
7.
El-Sanabary
N. Women in nursing in Islamic societies (2003) Bryant N (ed) Oxford University
Press, UK 56-89.
8.
Keshk
LI, Mersal FA, Al Hosis KF. Preparatory students’ perception about the nursing
profession and its impact on their career choice in Qassim University in KSA
(2016) Am J Nursing Res 4: 74-82.
9.
Al-Omar
BA. Knowledge, attitudes, and intentions of high school students toward the
nursing profession in Riyadh city, Saudi Arabia (2004) Saudi Med J 25: 150-155.
10.
Cooper
R. De-tracking reform in an urban California high school: Improving the
schooling experience of African American students (1996) J Negro Edu 65: 190-208.
11.
Mixer
S. Use of the culture care theory to discover nursing faculty care expressions,
patterns, and practices related to teaching culture care (2011) Online J
Cultural Competence Nursing Healthcare 1: 3-14.
12.
Campinha-Bacote
J. A biblically based model of cultural competence in the delivery of
healthcare services (2005) Cincinnati, Transcultural C.A.R.E. Associates, USA.
13.
Mahoney
J and Engebretson J. The interface of anthropology and nursing: Guiding
culturally competent care in psychiatric nursing (2000) Archives Psychiatric
Nursing 14: 183-190. https://doi.org/10.1053/apnu.2000.8657
14.
Jeffreys
M. Teaching cultural competence in nursing and health care inquiry, action, and
innovation (2nd Ed) (2010) Springer Publishing Company, New York.
15.
Gray
D and Thomas D. Critical reflections on culture in nursing (2006) J Cultural
Diversity 13: 76-82.
16.
Gustafson
D. Transcultural nursing theory from a critical cultural perspective (2005) Adv
Nurs Sci 28: 2-16. https://doi.org/10.1097/00012272-200501000-00002
17.
Leininger
M. Culture care theory: A major contribution to advance transcultural nursing
knowledge and practices (2002) J Transcult Nurs 10: 9. https://doi.org/10.1177/10459602013003005
18. Gallagher
R and Polanin J. A meta-analysis of educational interventions designed to
enhance cultural competence in professional nurses and nursing students (2015)
Nurse Educ Today 35: 333-340. https://doi.org/10.1016/j.nedt.2014.10.021
19.
Leininger
M. Culture care theory: A major contribution to advance transcultural nursing
knowledge and practices (2002a) J Transcult Nurs 13: 189-192. https://doi.org/10.1177/10459602013003005
20.
Leininger
M. Transcultural nursing: Concepts, theories, research, and practice, Leininger
M and McFarland M (Ed) (2002b) J Transcult Nurs US 117-143. https://doi.org/10.1177/104365960201300320
21. Whitt-Glover
M, Taylor W, Floyd M, Yore M, Yancey A, et al. Disparities in physical activity
and sedentary behaviors among U.S. children and adolescents: Prevalence,
correlates, and intervention implications (2009) J Public Health Policy 30: 309-334.
https://doi.org/10.1057/jphp.2008.46
22.
Jeffreys
M. Teaching cultural competence in nursing and health care, Baker and Sandra
(Ed) (2006) Springer, US 32: 343.
23.
Darnell
L and Hickson S. Cultural competent patient-centered nursing care (2015) Nurs
Clin North Am 50: 99-108. https://doi.org/10.1016/j.cnur.2014.10.008
24.
Lawton
D. Curriculum studies and educational planning (1983) Hodder and Stoughton, UK
01-161.
25.
Hampton
D and Hampton G. Professionalism and the nurse-midwife practitioner: An
exploratory study (2000) J Am Acad Nurse Pract 12: 218-225.
26.
Stake
R. The art of case study research (1995) Sage Publications Ltd, UK 1-175.
27.
Yin
R. Case study research: Design and methods (4th Ed) (2009) Sage Publications,
UK, 01-282.
28.
Ritchie
J and Spencer L. Qualitative data analysis for applied policy research, Bryman
A and Burgess RG (Ed) (1994) Routledge, UK 173-194.
29.
Merriam
S. Qualitative research and case study applications in education (1998)
Jossey-Bass Publishers, US.
30.
Patton
M. Qualitative research & evaluation methods (2002) Sage Publications, UK.
31.
Kardong-Edgren
S and Campinha-Bacote. Cultural competency of graduating US Bachelor of Science
nursing students (2008) Contemp Nurse 28: 37-44. https://doi.org/10.5172/conu.673.28.1-2.37
32.
Crawford
T and Candlin S. A literature review of language needs of nursing students who
have English as a second/other language and effectiveness of English language
support programmes (2013) Nurse Educ Pract 3: 181-185. https://doi.org/10.1016/j.nepr.2012.09.008
33.
Aldossary
A, While A, and Barriball L. Health care and nursing in Saudi Arabia (2008) Int
Nursing Review J 55: 125-28. https://doi.org/10.1111/j.1466-7657.2007.00596.x
34.
Almutairi
K. Culture and language differences as a barrier to provision of quality care
by health workforce in Saudi Arabia (2015)
Saudi Med J 36: 425-431. https://dx.doi.org/10.15537%2Fsmj.2015.4.10133
35. Almutairi
A, McCarthy A, and Gardner G. Understanding cultural competence in a
multicultural workforce: Registered nurses’ experience in Saudi Arabia (2015) J
of Transcultural Nursing 26: 16-23. https://doi.org/10.1177/1043659614523992
36.
Halligan
P. Caring for patients of Islamic denomination: Critical care nurses’
experiences in Saudi Arabia (2006) J of Clini Nursing 15: 1565-1573. https://doi.org/10.1111/j.1365-2702.2005.01525.x
37.
Weinick
R, and Krauss N. Racial and ethnic differences in children’s access to care
(2000) Am J Public of Health 90: 1771-1774.
38.
Woloshin
S, Bickell N, Shwartz L, Gany F, and Welch G. Language barriers in medicine in
the United States (1995) JAMA 273: 724-728.
39.
Green-Hernandez
C, Quinn A, Denman-Vitale S, Falkenstern S, and Judge-Ellis T. Making nursing
care culturally competent (2004) Holistic Nursing Practice 18: 215-218.
Abu-Zinadah
S. The situation of Saudi nursing (2004) Health Forum 52: 42-43.
41.
Dunagan
P, Kimble L, Gunby S, and Andrews M. Attitudes of prejudice as a predictor of
cultural competence among baccalaureate nursing students (2014) J Nurse 53: 320-328.
https://doi.org/10.3928/01484834-20140521-13
42.
Coombs
C, Arnold J, Loan-Clarke J, Wilkinson A, Park J, et al. Perceptions of nursing
in the NHS (2003) Nursing Standard 18: 33-38.
43.
Grossman
D, Arnold L, Sullivan J, Cameron M, and Murno B. High school students’
perceptions of nursing as a career: A pilot study (1989) J Nursing Edu 28: 18-21.
https://doi.org/10.3928/0148-4834-19890101-06
44.
Kalisch
P and Kalisch B. The changing image of the nurse (1987) Wesley Publishing
Company, California, USA.
45.
Kiger
A. Accord and discord in students’ images of nursing (1993) J Nursing Education
32: 309-317.
46. Spouse
J. An impossible dream? Images of nursing held by pre-registration students and
their effect on sustaining motivation to become nurses (2000) J Advanced
Nursing 32: 730-739. https://doi.org/10.1111/j.1365-2648.2000.01534.x
47. Repo
H, Vahlberg T, Salminen L, Papadopoulos I and Leino-Kilpi H. The cultural
competence graduating nursing students (2017) J Transcultural Nursing 28: 98-107.
https://doi.org/10.1177/1043659616632046
48. Salleh
K. The Islamic perspectives of caring (1994a) Proceedings of the First
International Nursing Conference: Education for Caring. Pengiran Anak Puteri
Rashidah Sa’adatul Bolkiah, College of Nursing, Brunei Darussalam 12-20.
49.
Holden
P and Littlewood J. Anthropology and nursing (1991) Routledge, London.
50.
Narayanasamy
A and Owens J. A critical incident study of nurses’ responses to the spiritual
needs of their patients (2001) J Advanced Nursing 33: 446-455. http://dx.doi.org/10.1046/j.1365-2648.2001.01690.x
51. Rassool
G. The crescent and Islam: Healing, nursing and the spiritual dimension. Some
considerations towards an understanding of the Islamic perspectives on caring
(2000) J Adv Nurs 32: 1476-1484. https://doi.org/10.1046/j.1365-2648.2000.01614.x
52.
Gregory
M. Introductory courses, student ethos, and living the life of the mind
(Initiation rights: Giving first-year students what they deserve) (1997)
College Teaching 45: 63-69.
*Corresponding author
Junaibi
SA, Adult Health Nursing Department, Oman Nursing
Institute, Directorate General of Human Recourses Development, Ministry of
Health, The Sultanate of Oman, Oman, Tel: +968 99455354, E-mail: bintmusa@hotmail.com
Citation
Junaibi SA, Chambers D and Narayanasamy A.
Nursing education and its cultural congruency in the sultanate of Oman: Case
study (2019) Nursing and Health Care 4: 6-12



