Introduction
The plants of Psoralea are used
in Traditional Chinese Medicine (TCM) for their good therapeutic effects. One
species belonging to the Psoralea plants is Psoralea corylifolia which is known
to have antimicrobial, antioxidative and anti-inflammatory
properties [1]. Besides the reported beneficial effects, there is also some
evidence of toxicity. Orally applied in form of an alcoholic seed extract
Psoralea can cause gonadal toxicity [2]. In high doses Psoralea can also induce
liver and kidney toxicity [3].
When applied externally skin-allergic reactions
have been reported when Psoralea treated skin areas were exposed to sun light [4]. Exactly this adverse effect is harnessed in
the treatment of psoriasis. The so-called PUVA therapy (Psoralen plus
ultraviolet A) is here the golden standard since initially reported in 1976 by
Fischer and Alsins. Psoralen, extracted from the plant Psoraleae corylifolia,
plus ultraviolet A (PUVA) photochemotherapy
combines the use of psoralen as a bath and long-wave ultraviolet A (UVA)
radiation. In this context skin phototoxicity is reported and the occurrence of
a phototoxic erythema as most common adverse event [5,6]. Interestingly the
word “Psoralea” is greek and means “affected with itch or with leprosy” [7]. Psoralen
in particular Psoraleae fructus (semen) (Buguzhi) is one component in a herbal mixture (BST III) used for
footbaths in Traditional Chinese Medicine. The Psoralea plant is considered
warm by nature and is used to treat the spleen and kidney meridians [8]. The
compound Psoralea admixed in herbal footbaths can be used to treat sensations
of cold (e.g. cold feet) and inflammatory disorders.
We report a case of a female patient who was prescribed a psoralen containing
herbal footbath for outpatient treatment. Without being aware of the phytotoxic
effect or Buguzhi she exposed her feet to solar irradiation during and after
the footbath and thereby provoked the formation of a phytotoxic erythema.
Case
Patient
information
A 60 year old female presented
herself at the TCM hospital in Bad Kötzting, Germany on May 24th 2016 with the
chief complaints of persistent coughing fits and disturbing smells especially
during meals for three years and diagnosis of bronchial asthma 25 years ago.
Further symptoms were nausea with vomitus, regurgitation, stomach pain,
abdominal cramping and asthenia. In March 2016 intolerances against fructose,
sorbitol and lactose have been diagnosed. She received a medical checkup with
gastroscopy, colonoscopy as well as computer tomography of cranium, thorax and
abdomen. The results of the examinations could not explain the symptoms.
Especially formation of a tumor could be excluded. At admission in the TCM
hospital, she had taken the antidepressant venlafaxine,
the thyroid hormone T4, the proton pump inhibitor pantoprazole and the
antispasmodic mebeverine. She has a familiar predisposition
for hypertension, stroke, obesity, asthma, and thyroid disease (Table 1).
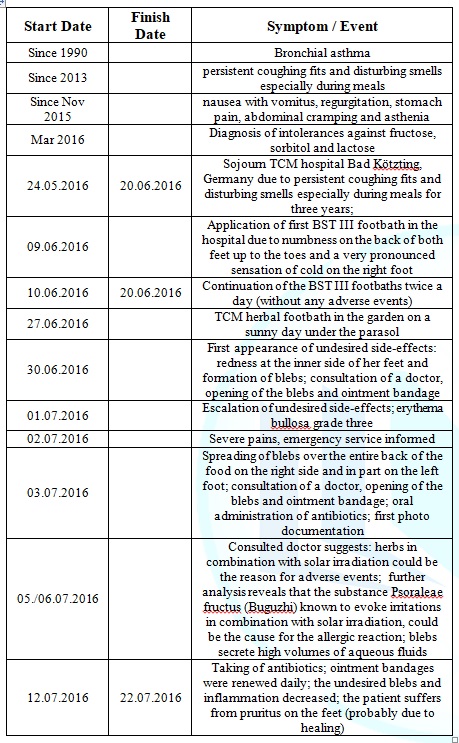
Table
1:
Important dates and times in this case.
Diagnostic
assessment
The patient used the e-health
portal VITERIO (Virtual Tool for Education, Reporting, and Outcomes) [9] which
is part of the individual
health management (IHM) program [10] developed by the Competence Centre for
Complementary Medicine and Naturopathy (CoConat), TU Munich, Germany. Briefly
VITERIO was designed to collect patient reported outcomes
(PRO) and to make them in equal measure available for the participant and the
health professional. A series of specially designed questionnaires based on
scientific findings form the core of the e-health platform.
According to the
patients information deposited in VITERIO her medical history includes
hypertension, vascular disease, respiratory disorder, gastro-intestinal disease,
thyroid disease, dermatosis, allergies and intolerances, arthropathy and
muscular disorder, as well as back pain. General anamnesis revealed loss of
efficiency and chronic fatigue, sweating, in particular in the head region and
the body, regurgitation, halitosis, nausea, vomitus, flatulence, pruritus in
the anus region, allergic reactions on the skin, the respiratory system and the
gastro-intestinal region.
Based on the general
anamnesis, specific anamnesis was carried out concerning respiratory diseases,
vascular diseases, arthropathy and muscular disorders,
dermatosis and gastro-intestinal disease in order to capture particular
symptoms more sophisticatedly and in progress. Thereby further symptoms have
been determined among them M. Raynaud, joint stiffness in the morning, muscle
cramps, varicose, tick bite, eczema, onychomycoses, pigmentary abnormalities,
gastritis, irritable colon and chronic obstipation.
At admission in the TCM
hospital, Bad Kötzting on the 24th of May 2016 the primary diagnosis was a
somatoform disorder in particular major depressive recurrent disorder (ICD-10 F45.33),
becoming manifest in the respiratory system. Further diagnoses were
tension-type headache (ICD-10 G44.2), hypothyroidism (ICD-10
E03.9), gastro-esophageal reflux disease without esophagitis (ICD-10 K21.9),
irritable bowel syndrome without diarrhea (ICD-10 K58.9).
Therapeutic
Intervention
Besides the pharmacologic
intervention with mebeverine, T4, pantoprazole and venlafaxine, which was
already administered at admission, the patient was prescribed a high dose
Traditional Chinese herb therapy with repeatedly modified ingredients three
times a week, acupuncture and qigong therapy. Due to numbness on the back of
both feet up to the toes and a very pronounced sensation of cold on the right
foot, she obtained so-called BST III herbal footbaths (Table 2), starting at day 15 of the inpatient stay until discharge
from hospital, twice daily for about 20 minutes (for about 11 days). During the
stay at the TCM hospital the patient did not develop any undesired side
effects.
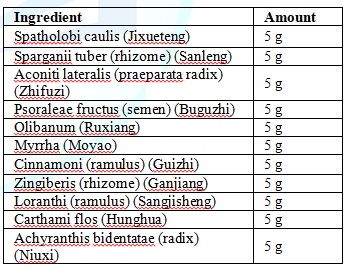
Table 2: Ingredients BST
III Herbal Footbath.
Follow-up and
Outcomes
At discharge from the hospital
the symptoms of nausea and abdominal pain correlated to gastro-esophageal reflux
disease without esophagitis (ICD-10 K21.9) and irritable bowel syndrome
without diarrhea (ICD-10 K58.9) decreased. For further treatment of the
numbness on the back of both feet up to the toes, the patient was prescribed
the continuation of the herbal footbaths and the respective recipe containing
the composition of the TCM herbs was handed out to her.
The patient continued the
footbaths at home according to this prescription after one week of
intermission. On day 15 after discharge she reported that she had carried out
the prescribed footbath in her garden under the parasol. Since then she had painful
blebs on her feet (Figure 1). She
was recommended to discontinue the footbaths immediately.

Figure 1: The three photos
show the phototoxic reaction after a herbal foorbath with Buguzhi under sun
radiation. Both feet of the patient show redness and blebs.
The patient reported that she
carried out a footbath according to the prescription in lukewarm water on a
sunny day (27.06.2016) in her garden under a parasol. Three days later she
recognized a moderate redness at the inner side of her feet and later in the
afternoon also blebs. On the same day a doctor opened the blebs and made an
ointment bandage. The day after the adverse events escalated and after another
day (02.07.2016) she could not stand on her feet any longer due to severe
pains; she informed the emergency
service. Meanwhile the occurrence of blebs spread over the entire back of
the food on the right side and in part on the left foot. The consulted doctor
opened the blebs, made ointment bandages and prescribed an antibiotic due to
heavy swelling and redness of the legs.
In this context a first set of
photos was made to keep records of the adverse events (Figure 1). On the 5th and 6th of July 2016 the doctor
suggests that the adverse events could be caused by an allergic reaction
against one of the herbs in combination with solar irradiation. The blebs
secreted high volumes of aqueous fluids.
Further analysis of the case revealed that the primary TCM recipe of the
BST III herb footbath, that originally did not contain the substance Psoraleae
fructus (Buguzhi) was modified in the year 2003 regarding the add-on of exactly
this compound (Buguzhi).
The compound Buguzhi is known to
cause phototoxic reactions; the blebs are probably a phototoxic side effect
due to the admixture of Buguzhi in the herbal foodbath. On the 12th of July
2016 the patient reports that she did not wear stockings during the herb
footbath and afterwards walked around in the garden barefoot or in sandals
without stockings exposed to solar irradiation. Formation of blebs could be
observed exactly in those areas of the feet that were in contact with the
footbath. The doctor prescribed an antibiotic that was taken by the patient for
10 days. During the next 10 days while the patient took the antibiotic, the
ointment bandages were renewed daily. After these 10 days the undesired blebs
and inflammatory reactions decreased. Probably due to healing, the patient
suffered from pruritus on the feet. On the 25th of July 2016 the patient
presented herself for the last time concerning the undesired side effects of
the Psoraleae food bath at the TCM hospital in Bad Kötzting. On the same day
the second (the last) series of Photos were taken (Figure 2). At that time the patient did hardly show any symptoms
and the blebs almost completely disappeared as can be seen in Figure 2. We
assume that therefore the patient did not show up any longer and consequently,
long term documentation is missing.

Figure 2: Treatment with ointment bandages and
antibiotics lead to melioration of the adverse event. Redness and blebs
disappeared after about 10 days
Discussion
The seeds of Psoralea corylifolia
L. (P. corylifolia), also called Buguzhi in Chinese, are a common agent in Traditional
Chinese (herbal) Medicine. Buguzhi is a Yang tonifying substance and used for
the treatment of Yang deficiencies which are associated with the sensation of
cold, listlessness, and paleness. Psoralea has been used
widely for the treatment of various types of skin diseases such as vitiligo, alopecia
areata, leukoderma, and psoriasis [11]. P. corylifolia and its standard
components are known to have medicinal properties in combating diabetes [12,13],
obesity [14], tumorigenesis [15,16], oxidative stress [13,17], and inflammation
[18,19], and to have estrogen-like effects [20,21].
Besides these encouraging
results, toxicity of Psoralea has been reported in a variety of cases. In the
context of PUVA therapy widely used for the treatment of Psoriasis, skin
phototoxicity is reported and the occurrence of a phototoxic erythema as most
common adverse event [5,6]. In a recently published study involving 84 patients
in safety case reports of P. corylifolia, the reported adverse events were mainly
liver damage (55.95%) and light toxic contact dermatitis (38.10%). This
suggests that P. corylifolia may also lead to liver damage besides the already
known phototoxicity.
Reproductive toxicity and renal damage have only been observed in studies on
animals but not in humans [22].
In the here presented case the
patient carried out a PUVA treatment (Psoralea as part of the herbal footbath
in combination with sunlight exposure) without being aware of it. As
consequence of the phototoxic effect of Psoralea, painful blebs developed on
her feet which disappeared after discontinuation of the footbath, and treatment
with antibiotics and ointment bandages. The adverse event could have been
prevented if the patient had been informed about the phytotoxic effect of
Psoralea.
Conclusion
When prescribing herbal footbaths
containing the compound Psoraleae fructus (Buguzhi), doctors must inform the
patients about the phototoxic effects of this substance and explain that these
footbaths must not be applied in combination with sun exposure.
Acknowledgments
We would like to thank the TCM
Hospital Bad Kötzting for the support.
References
1.
Shrestha S, Jadav HR, Bedarkar P,
Patgiri BJ, Harisha CR, et al. Pharmacognostical evaluation of Psoralea
corylifolia Linn. Seed (2018) J Ayurveda Integr Med 9: 209-212. https://doi.org/10.1016/j.jaim.2017.05.005
2.
Takizawa T, Imai T, Mitsumori K, Takagi
H, Onodera H, et al. Gonadal toxicity of an ethanol extract of Psoralea
corylifolia in a rat 90-day repeated dose study. The Journal of toxicological
sciences (2002) 27: 97-105.
3.
Xu Y, Zhao Y, Xie J, Sheng X, Li
Y, et al. The Evaluation of Toxicity Induced by Psoraleae Fructus in Rats Using
Untargeted Metabonomic Method Based on UPLC-Q-TOF/MS (2017) Evidence-based
complementary and alternative medicine: eCAM. 2017: 6207183. https://doi.org/10.1155/2017/6207183
4.
Anderson TF and Voorhees JJ.
Psoralen photochemotherapy of cutaneous disorders (1980) Annu Rev Pharmacol
Toxicol 20: 235-257. https://doi.org/10.1146/annurev.pa.20.040180.001315
5.
Calzavara-Pinton PG, Ortel B,
Carlino AM, Honigsmann H and De Panfilis G. Phototesting and phototoxic side
effects in bath PUVA (1993) J Am Acad Dermatol 28: 657-679. https://doi.org/10.1016/S0190-9622(08)81791-4
6. Koulu LM and Jansen CT. Skin
phototoxicity variations during repeated bath PUVA exposures to 8-methoxypsoralen
and trimethylpsoralen (1984) Clin Exp Dermatol 9: 64-69. https://doi.org/10.1111/j.1365-2230.1984.tb00757.x
7.
Chopra B, Dhingra AK and Dhar KL.
Psoralea corylifolia L. (Buguchi)-folklore to modern evidence: Review (2013)
Fitoterapia 90: 44-56. https://doi.org/10.1016/j.fitote.2013.06.016
8.
Daiquan L. Chinese Medicine. China:
Shanghai Scientific and Technical Publishers, 2000-2006, China.
9.
Melchart D, Eustachi A, Gronwald
S, Wuhr E, Wifling K, et al. Introduction of a web portal for an Individual
Health Management and observational health data sciences (2018) Patient related
outcome measures 9: 183-196. https://doi.org/10.2147/PROM.S157410
10. Melchart
D, Eustachi A, Wellenhofer-Li Y, Doerfler W and Bohnes E. Individual Health
Management - A Comprehensive Lifestyle Counselling Programme for Health
Promotion, Disease Prevention and Patient Education (2016) Forsch Komplementmed
23: 30-35. https://doi.org/10.1159/000443544
11. Zhang
X, Zhao W, Wang Y, Lu J and Chen X. The Chemical Constituents and Bioactivities
of Psoralea corylifolia Linn.: A Review (2016) Am J Chin Med 44: 35-60. https://doi.org/10.1142/S0192415X16500038
12. Lee H, Li H, Noh M and Ryu JH.
Bavachin from Psoralea corylifolia Improves Insulin-Dependent Glucose Uptake
through Insulin Signaling and AMPK Activation in 3T3-L1 Adipocytes (2016) Int J
Mol Sci 17: 527. https://doi.org/10.3390/ijms17040527
Seo E, Lee EK, Lee CS, Chun KH,
Lee MY, et al. Psoralea corylifolia L. seed extract ameliorates
streptozotocin-induced diabetes in mice by inhibition of oxidative stress
(2014) Oxid Med Cell Longev 2014: 897296. http://dx.doi.org/10.1155/2014/897296
14. Seo
E, Oh YS and Jun HS. Psoralea corylifolia L. Seed Extract Attenuates
Nonalcoholic Fatty Liver Disease in High-Fat Diet-Induced Obese Mice (2018)
Nutrients 8: 83. https://doi.org/10.3390/nu8020083
15. Jung
B, Jang EH, Hong D, Cho IH, Park MJ, et al. Aqueous extract of Psoralea
corylifolia L. inhibits lipopolysaccharide-induced endothelial-mesenchymal
transition via downregulation of the NF-kappaB-SNAIL signaling pathway (2015)
Oncol Rep 34: 2040-2046. https://doi.org/10.3892/or.2015.4154
16. Rajan
V, Tripathi J, Variyar P and Pandey BN. Mechanism of cytotoxicity by Psoralea
corylifolia extract in human breast carcinoma cells (2014) J Environ Pathol
Toxicol Oncol 33: 265-277.
17. Dang
Y, Ling S, Duan J, Ma J, Ni R, et al. Bavachalcone-induced manganese superoxide
dismutase expression through the AMP-activated protein kinase pathway in human
endothelial cells (2015) Pharmacology 95: 105-110.
18. Lee
KM, Kim JM, Baik EJ, Ryu JH and Lee SH. Isobavachalcone attenuates
lipopolysaccharide-induced ICAM-1 expression in brain endothelial cells through
blockade of toll-like receptor 4 signaling pathways (2015) Eur J Pharmacol 754:
11-18. https://doi.org/10.1016/j.ejphar.2015.02.013
19. Yang
HJ, Youn H, Seong KM, Yun YJ, Kim W, et al. Psoralidin, a dual inhibitor of
COX-2 and 5-LOX, regulates ionizing radiation (IR)-induced pulmonary
inflammation (2011) Biochem Pharmacol 82: 524-534. https://doi.org/10.1016/j.bcp.2011.05.027
20. Liu
X, Nam JW, Song YS, Viswanath AN, Pae AN, et al. Psoralidin, a coumestan
analogue, as a novel potent estrogen receptor signaling molecule isolated from
Psoralea corylifolia (2014) Bioorg Med Chem Lett 24: 1403-1406. https://doi.org/10.1016/j.bmcl.2014.01.029
21. Park
J, Kim DH, Ahn HN, Song YS, Lee YJ, et al. Activation of Estrogen Receptor by
Bavachin from Psoralea corylifolia (2012) Biomol Ther (Seoul) 20: 183-188. https://doi.org/10.4062/biomolther.2012.20.2.183
22.
Tian WY, Lan S, Zhang L, Sun L,
Huang JK, et al. Safety evaluation and risk control measures of Psoralea
corylifolia (2017) Zhongguo Zhong Yao Za Zhi 42: 4059-4066. https://doi.org/10.19540/j.cnki.cjcmm.20170919.011
*Corresponding author
Melchart D, Competence Centre for Complementary
Medicine and Naturopathy, Klinikum rechts der Isar, Technische Universität
München, Munich, Germany, Tel: +49 89 726697 0, E-mail:
dieter.melchart@tum.de
Citation
Bachmeier BE, Hager S and Melchart D. Case
report of a phototoxic reaction after application of a footbath with herbal
traditional Chinese medicine (TCM) (2019) Nursing and Health
Care 4: 13-16



