
 PDF
PDF
Introduction
Mortality rate of infants and under five serve as a more sensitive indicator of health security across and within economies. Aside from being a factor associated with population wellbeing, it also reflects improper childcare [1], state of public health and hygiene, environmental sanitation, cultural mores about feeding and clothing, socio-economic development, and above all, the peoples attitude towards the dignity and value of human life itself [2]. Clearly public health conditions and socio-economic wellbeing are greatly determined by infant and under five mortality rate [3].
Globally, according to the United Nations International Childrens Emergency Fund, it is estimated that there were around 7 million under five deaths recorded with Sub-Saharan Africa as a major contributor. Further 257 deaths per 1000 live births in Afghanistans for under-five was recorded, third highest in the world, surpassed only by the rates for Angola and Sierra Leone [4]. Even in other highly developed countries, protecting human life is still a problem. The United States rate of infant mortality did not decline from 2000 to 2005, 6.86 infant deaths per 1,000 live births, not significantly different than the rate of 6.89 in 2000 higher than those in most other developed countries [5] even in Canada with 5.1 in 2007 [6].
The Philippines is not spared of the problems that countries abroad are facing. It was recorded that there were 64 deaths per 1,000 live births in 1993 to 40 deaths in 2003 for under five children. A study conducted by the National Statistics Office; a greater risk of dying is associated to a child born in the country as compared to other Southeastern Asian Countries (NDHS, 2003) with 29 for every 1000 infants births die and 40 before reaching the age of five. In the case of under-five, the country will be able to achieve the Millennium Development Goals (MDG) of reducing the national U-5MR by two-thirds or only 19 deaths per 1,000 live births if the trend will continue [7].
The research findings can be useful value for the National Government to look into the possible major contributors of mortality rate of infants and under five in the country. Strengthening the sectors that contributes significantly may also be given sufficient focus.
Theoretical Background
Economic theory
The basic economic theory supports the study. This explains that an increase in per capita income will lead to increases in the demand for health care if everything else is held constant and if health care is a normal good [8]. In this study, it is believed that when GDP per capita increases, the budget allotted to health expenditure also increases so as average percentage for immunization.
Factors affecting mortality rate several studies were conducted to determine different factors affecting mortality rate of infants and under five. And it is also generally understood that some may influence positively or negatively. This study emphasizes significant factors that may associate mortality rate. First, it is hypothesized that GDP per capita is associated with health expenditure total percentage of GDP per capita. That is, the proportion allotted for health expenditure is affected by GDP per capita fluctuation. The country recorded the highest GDP per capita (1995-2013) in 2013 with 2787 and with 958 as the lowest in the year 2001. Several studies have confirmed that GDP per capita has a strong negative effect to infant mortality rate [9,10]. Further, the health expenditure total percentage of GDP per capita in the country is relatively high with 4.42 percent of the GDP per capita in 2012 and lowest in 2002 which accounted for only 2.80 percent. Musgrove [11] confirmed in his study that private expenditure on health reduces child mortality. In this study, it is hypothesized that GDP per capita and health expenditure total percentage of GDP per capita affect mortality rate of infants and under five and that GDP per capita affect health expenditure total percentage of GDP per capita.
Second, it is hypothesized that out of the pocket health expenditure affect mortality rate of infants and under five. It is also essential to note whether out-of-pocket health expenditure (% of private expenditure on health) affect mortality rate. The country received the highest OOPHE in 2006 which accounted for 85.3 percent of the private expenditure on health. Akinci et al. [12] revealed in their study that private spending on health significantly reduce infant and under five mortality rates.
Third, average percentage of immunization of DPT and measles is associated to mortality rate of infants and under five. Immunization is regarded to influence significantly the dependent variable. Nyrako et al. [13] found out that Immunization can substantially enhance child survival in high-mortality settings, reducing mortality by up to two-thirds in children who receive the full package relative to children who have received no vaccinations. In 2013, the country recorded a highest immunization percentage of 90.5 and lowest in 1995 with only 71 percent of 12-21 months children received DPT and measles vaccine. It is assumed that the higher the percentage of immunization, the lower the rate of infant and under five mortality rates. In this study, GDP per capita, HETPGDP and OOPHE are assumed to influence average percentage of immunization.
Research Questions
The following research questions were formulated on the basis of the theoretical discussion above:
- Which of the four independent variables affect mortality rate of infants and under five in the Philippines?
- What are the structural causal relationships among the variables affecting average mortality rate as a dependent variable?
Research Designs Variables
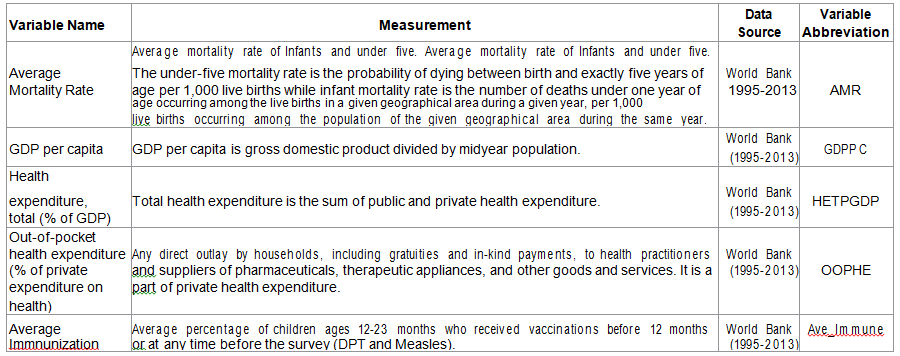
Five independent variables and one dependent variable were analyzed in the study. The independent variables include: per capita DGP, Health expenditure (total percentage of GDP), out-of-pocket health expenditure (% of private expenditure on health) and average percentage of immunization of DPT and measles. Mortality rate was the dependent variable. Please refer in the table below for the names of the variables, the measurement and the data source (Table 1).
Analysis method
First, descriptive statistics and correlation coefficients for GDPPC, HETPGDP, OOPHE, Ave immune and AMR were generated using SPSS version 20. Second, Analysis of Moment Structures (AMOS) 20.0 program was carried out for structural equation modeling (SEM). In SEM, estimating coefficients was channeled through Maximum Likelihood Estimation method. According to Ingram et al, Maximum Likelihood Estimation (MLE) is an iterative procedure that attempts to maximize the likelihood that obtained values of the criterion variable will be correctly predicted unlike OLS that minimizes the squared deviations between values of the criterion variable and those predicted by the model. Since χ2is sensitive to sample size [14], and framing the null hypotheses is often too difficult, both the χ2 and fitness tests were used to evaluate model fitness. Goodness-of-Fit Index (GFI), Comparative Fit Index and Normed Fit Index were also presented to evaluate goodness of fit of the model. Third, modification index was also carried out to find the optimal model for explaining the relationships among variables, in case the hypothetical model projected will be proved not suitable. Fourth, the mediating effects of HETPGDP and average percentage of immunization were tested employing the bootstrap method.
Hypothetical model
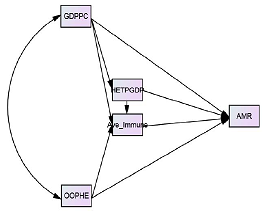
Presented below is the hypothetical constructed model to test the possible exogenous variables that may possibly affect mortality rate based on the theoretical points discussed.
In this study, GDPPC and OOPHE were treated as the exogenous variables and the rest of the variables were endogenous (Figure 1).
Results
Descriptive statistics
Presented in Table 2 is the descriptive statistics of the variables used in the study. This includes the minimum, maximum, means and the standard deviations. The data is reflective of the countrys GDPPC, HETPGDP, Ave Immune, OOPHE and AMR. On the average, the Gross Domestic Product Per Capita (GDPPC) for year 1995-2013 is 1512.56, 57.31 for health expenditure total percentage of gross domestic (HETPGDP), 81.6 in the out of the pocket health expenditure and an average immunization rate of 83.39 and 32.44 in the average mortality ate. The data for average mortality rate is suggestive to heighten
significant measures that may directly or indirectly influence on it (Table 2).

Table 2: Descriptive Statistics.
Correlation of the variables
Presented in Table 3 is the variables correlation included in the hypothetical model. The structure hypothetically presents that the four endogenous variables are directly or indirectly interconnected. In the final model, the following were found to be significantly correlated: HETPGDP and GDPPC (r=.991, p<.01); OOPHE and GDPPC (r=.560, p<.05); OOPHE and HETPGDP (r=.597, p<.01). For the dependent variable, AMR and GDPPC (r=-.829, p<.01); AMR and HETPGDP (r=-.826, p<.01); MR and Ave Immune (r=-.713, p<.01) were also found significant. This means that the gross domestic product per capita is translated is significantly translated into health expenditure total percentage of gross domestic product which can also be significantly translated from an increase in the Out- of the pocket health expenditure. An increase in the percentage of immunization will significantly decrease the average mortality rate of children (Table 3).
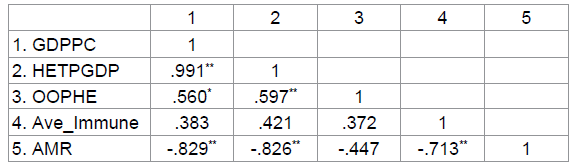
Table 3: Variable Correlation.
Goodness of Fit
According to Gao et al, as cited in Young-Chool Choi, Ji-Hye L [14] structural equation modelling does not have a widely accepted measure of goodness of fit, thus this study follows the tests explained by Ho [15] that includes chi square, GFI, CFI and NFI. Presented below is the table for the goodness of fit of the hypothesized model (Table 4).
Table 4: Goodness of Fit of the Model.
SE Model
As presented in Table 5, the model fits the data well evident in the following measures of goodness of fit: χ2 =2.748 (p=.097); CFI=.985; GFI=.946 and NFI=.978. All values exceed the recommended threshold and can be described as acceptable (Table 5), (Figure 2).
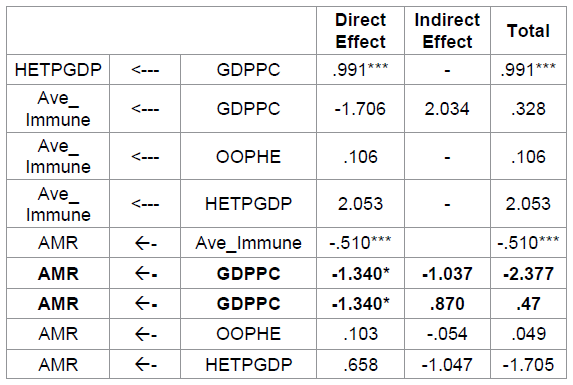
Table 5: Independent Variables Affecting Mortality Rate.
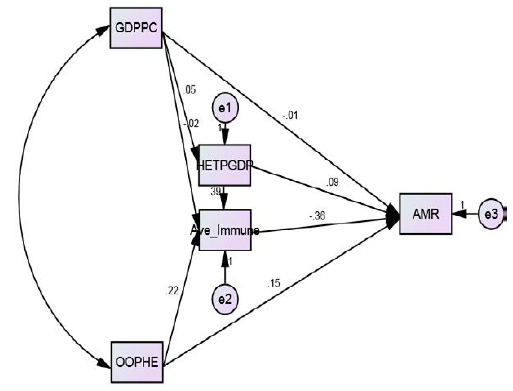
Figure 2: Structural Equation Model.
As shown in Table 5, it was found out that GDPPC significantly affects HETPGDP (β=.991; p=.000). More importantly it resulted that GDPPC (β=.-1.340; p<.05) and ave immune (β=-.510; p<.001) both affect mortality rate negatively. The direct effects of both GDPPC and ave immune are the identified key structural paths. Their negative sign implies that a higher rate of average percentage of immunization and increase in GDP per capita will reduce mortality rate. Both economic and health implications can be extracted in the result to determine ways and means to increase GDP and percentage of immunization.
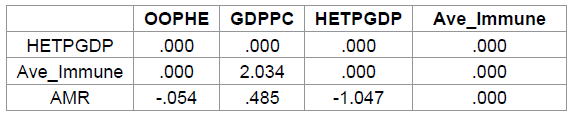
Table 6: Standardized Indirect Effects (Group number 1 - Default model).
Table 6 shows the standardized indirect effect or the as the index of mediation [16]. GDPPCs indirect effect on Ave Immune is 2.034 and not significant p=.212, 95% CI [-2.831, 7.297], OOPHE to AMR is still not significant (-.054), p=.866, 95% CI [-.327, .802]; HETPGDP to AMR not significant (-1.047), p=.116, 95% CI [.000, .885], and GDPPC to Ave Immune to Mortality rate (.485), p=.387, 95% CI [-1.310, 3.434] is also not significant.
Meaning, HETPGDP and Ave immune do not significantly mediate the effect of GDPPC and OOPHE to AMR (Table 7).

Table 7: Standardized Indirect Effects - Two Tailed Significance
Conclusions and Policy Implications
The central purpose of this endeavor is to determine the causal complex connections between GDPPC, HETPGDP, ave immune and OOPHE to the average mortality rate of infants and under five and to craft policies that can help reduce incidence of mortality rate by employing structural equation modeling technique. The study follows the requirements using the statistical tool in specifying the model and in evaluating the goodness of fit criteria. Estimating for the direct, indirect effect and total effects was also carried out.
Model fit indices include χ2 =2.748, p=.097; GFI=.946; CFI=.985 and NFI=.978. Based on the set criteria study shows that the generated model is statistically significant and can be described as acceptable. The following implications are drawn out from the findings. First, considering that the model including GDPPC negatively affect mortality rate, there is a need to look into the significant determinants of increasing the GDPPC. Second, since average percentage of immunization significantly affect mortality rate, widening immunization for both DPT and measles vaccination should also be considered.
Limitations of the Study
This study will not claim that it does not encounter the problem of empirical estimation.
covers data from 1995-2013 which may be considered as limited. A recommendation to cover years from 1980-2016 can be considered. Second, it should also be noted that the study only focused in the Philippines. Although the hypothetically projected model was proved significant, the result may not be applicable to other countries. Third, the study includes only limited number of variables, many variables may also affect mortality rate but were not included in the conceptual model. Maternal health care, environmental conditions, access to improved sanitation and nutritional status of the parents may also be considered.
The whole idea of estimation is to quantify the effects of GDPPC, HETPGDP, Ave Immune, and OOPHE to AMR. More interesting results and valid conclusions could be drawn from a more a global study and for this time may consider variables other economic and financial sectors.
References
1.
1. Zakir M, Wunnava PV. Factors
Affecting Infant Mortality Rates: Evidence From Cross-Sectional Data (1999)
Applied Economics Letters Pp: 271–273.
2.
Bawa AA. Living standards, household
size and childhood survival in Africa: Evidence from Census Data (2001)
University of Pennsylvania, Population Studies Center, Philadelphia.
3.
Miller NZ, Goldman GS. Infant
mortality rates regressed against number of vaccine doses routinely given: Is
there a biochemical or synergistic toxicity? (2011) Hum Exp Toxicol 30:
1420–1428.
4.
Adedini. Regional Variations in
infant and child mortality in Nigeria: A Multilevel Analysis (2015) Journal of
Biosocial Science 47: 165-187.
5.
MacDorman. Recent Trends in Infant
Mortality in the United States (2008) NCHS data brief, National Center for
Health Statistics Hyattsville, MD, USA.
6.
Infant Mortality (2016) Conference
Board of Canada.
7. Infant Mortality in the Philippines is Higher than Other Southeast Asian
Countries (2004) Philippine Statistics Authority.
7.
Day K, Tousignant J. Health
Spending, Health Outcomes and Per Capita Income in Canada: A Dynamic Analysis.
(2005).
8.
Upadhyay KA, Srivastava S.
Association between Economic Growth and Infant Mortality: Evidence from 132
Demographic and Health Surveys from 36 Developing Countries (2012)
International
Institute for Population Sciences
Mumbai, India.
9.
Wheatley, Lisa. Factors affecting
child mortality (2015) Honors Theses.
10.
Musgrove P. Public and Private Roles
in Health: Theory and Financing Patterns (1996) Health, Nutrition and
Population (HNP) Discussion Paper, World Bank.
11.
Akinci. Examining the Impact of
Health Care Expenditures on Health Outcomes in the Middle East and North Africa
(MENA) Region (2014) Journal of Health Care Finance.
12.
Nyarko. Immunization Status and
Child Survival in Rural Ghana (2001) Policy Research Division Working Paper
#147.
13.
Young-Chool Choi, Ji-Hye L.
Analyzing the relationships among the factors affecting educational
competitiveness: An application of the structural equation modeling approach
(2014)
Journal of Arts and Humanities 3:
40-50.
14.
Ho Robert. Handbook of Univariate
and Multivariate Data Analysis with IBM
(2014) CRC Press Taylor & Francis Group FL USA.
15.
Preacher KJ, Hayes AF. Contemporary
approaches to assessing mediation in communication research (2008a) In: The
Sage sourcebook of advanced data analysis methods for
communication
research AF Hayes, MD Slater, LB
Snyder (Edtrs.) Thousand Oaks, CA, Sage, Pp: 13–54.
*Corresponding author
Sherwin S. Fortugaliza, Davao City National High School, Davao City, Philippines, Tel: (082) 227-9102 E-mail: sherwin.fortugaliza@yahoo.com
Citation
Fortugaliza SS(2017) Factorsaffecting Mortality Rate of Infants and under Five in the Philippines: An application of Structural Equation Modeling. NHC 119: 21-25
Keywords
Infant and under five, Mortality rate, structural equation modeling
