Nagaveni NB*, Meghna Bajaj, Sneha Yadav, Poornima P
Permanent mandibular second molars usually show two roots, one mesial and theother distal root with four root canals (two mesial and two distal canals). Variation in
root number and canal morphology rarely occur in these teeth. Cone Beam Computed Tomography is a new advent in the diagnostic field which provides three dimensional
clear picture of the root/canal. The present article describes the endodontic managementof permanent mandibular left second molar with Vertucci II canal configuration using cone beam computed tomography.
Introduction
Permanent mandibular second molars usually
display the normal anatomy of two roots, one mesial and the other distal with
four root canals (two mesial and two distal) [1,2]. However, the morphology of
root canal system in these teeth can vary according to the races, age and
gender of the population studied [3-6]. For the success of endodontic
treatment, thorough knowledge of canal anatomy, number
of roots and curvature of root canal is important to locate, negotiate and
finally for management of canals. The conventional diagnostic method using
periapical radiographs provides only two dimensional pictures of the roots and
canals [7]. So chances of leaving the undiagnosed canals are high which finally
ends up in the treatment failure.
Cone
beam computed tomography (CBCT) imaging is a novel diagnostic modality
which attracted the field of Dentistry in various aspects, as it provides a 3
dimensional view of the entire canal system [3-6]. The aim of this paper is to
describe the endodontic management of permanent mandibular second molar with
Vertucci II canal type which was diagnosed using CBCT scan.
Case Report
A 14-year-old female patient reported to the Department of Pedodontics and Preventive Dentistry
with a chief complaint of pain in lower left back region of jaw since 1 week.
She gave a history of nocturnal pain which was moderate, continuous,
non-radiating and increases while biting food. On clinical examination, there was
deep occlusal caries
in relation to permanent mandibular left second molar (37 – FDI tooth
notation), and the tooth was sensitive on percussion. The tooth showed positive
response to pulp test (heat test). Provisional diagnosis of acute apical periodontitis was made
considering all the above factors. To confirm the diagnosis, an intraoral
periapical radiograph was taken with respect to 37, which showed two
radiolucent canals which were in close approximation with each other near apex,
with periapical radiolucency (Figure 1, A); finally based on the clinical and
radiographic findings the case was diagnosed as chronic periapical abscess.
Endodontic treatment of 37 followed by prosthetic
rehabilitation was planned. In the following appointment an access cavity
preparation was done. 3 canals were negotiated, 2 mesially which were very
close to each other and 1 distally. The mesial root as wells as canals were
severely curved. Working length was determined using periapical radiograph,
with different angulation which suggested that the canals were fused at the
apex (Figure 1, B). To confirm the number of canals and to know whether the
canals are fused at apex or not, CBCT imaging was made with respect to 37. On
serial axial sections of CBCT imaging it was found that the two mesial canals
were very close to each other and hence looked like one canal. The distal root
had one straight canal. As the two canals progressed apically the two canals
merged each other resulting in one canal (2-1 Vertucci canal type) [8] (Figure
2). In panoramic view of the CBCT it was noticed that the mesial canal had
severe curvature (‘S’ shape based on Dobo-Nagy et al. classification [9])
towards buccal side fused with the distal root (Figure 3).
After location and confirmation of canal’s configuration and
pulp debridement,
biomechanical preparation of the canals was done using hand protaper files
along with hydrogen peroxide as an intermittent irrigant. Once the canals were
prepared triple mix antibiotic
dressing was given for 1 month. After 1 month patient was asymptomatic and
canals were obturated to the working length using single cone obturation
technique (Figure 1, C & D).
![[A] Intraoral Peri-apical, pre-operative diagnostic radiograph showing permanent mandibular left second molar with complex root anatomy. [B] Working length determination [C] Master cone selection [D] Post-obturation radiograph.](http://edelweisspublications.com/edelweiss/figures/drm-17-104_figure_1.png)
Figure 1: [A] Intraoral Peri-apical, pre-operative diagnostic radiograph showing permanent mandibular left second molar with complex root anatomy. [B] Working length determination [C] Master cone selection [D] Post-obturation radiograph.
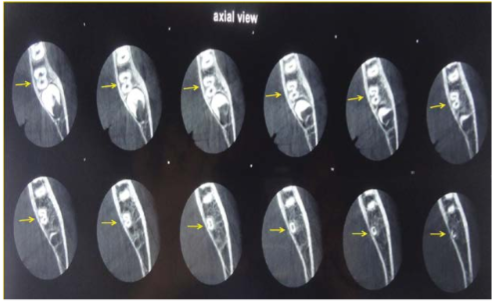
Figure 2: Serial axial sections of CBCT imaging of the permanent mandibular left second molar. Initially we can see the two canals. As the canals progress apically merging of two canals resulting in one canal can be seen (arrows).

Figure 3: CBCT image of the same tooth (37) showing Vertucci type II canal configuration (2-1) and also ‘S’ shape bend in the mesial canal (arrow).
Discussion
The type and canal morphology in mandibular molars presents
clinical complications during endodontic therapy. Vertucci in 1984 [8]
categorized the root canal configuration of human permanent teeth into eight
types as follows: Type 1 – a single
canal extends from the pulp chamber to the apex (1); Type II – two separate
canals leave the pulp chamber and join short of the apex to form one canal
(2-1), Type III – one canal leaves the pulp chamber divides
into two within the root and then merges to exist as one canal (1-2-1), Type IV
– two separate and distinct canals extend from the pulp chamber to the apex
(2), Type V - one canal leaves the pulp
chamber and divides short of the apex into two separate and distinct canals
with separate apical foramina (1-2), Type VI – two separate canals leave the
pulp chamber, merge within the body of the root and re-divide short of the apex
to exit as two distinct canals (2-1-2), Type VII – one canal leaves the pulp
chamber, divides and then rejoins within the body of the root and finally
re-divides into two distinct canals short of the apex (1-2-1-2) and Type VIII –
three separate canals extend from the pulp chamber to the apex (3). Based on
this classification, in the present case the canal shape was categorized as
Type II shape (2-1) as the two separate canals originated from pulp chamber and
merged at the apex.
Ahmad et al. [5] found 8% of permanent mandibular second
molars with fused two roots in their study using clearing technique in Sudanese
population. They have also claimed that most of the distal roots of second
molars (69%) had one canal. Most mesial roots (83%) had two canals, of which
type IV (63%) and type II (18%) canal configurations were most common. Whereas
Mirzaie et al. [4] noticed only 30.3% of type II canal shape in Hamadani
population using CBCT diagnostic tool. Recently contrary to this finding Nur et
al. [3] found maximum of type IV canal variation in Turkish population
following CBCT evaluation.
The root canal curvature is classified by Dobo-Nagy et al in
1995 [9] as I (straight), J (apical curve), C (entirely curved) and S
(multi-curved) shape based on the curvatures seen in the canal. According to
this classification, in our case the mesial canal of the molar showed ‘S’ shape
curve merging with the distal root near the apex.
Use of CBCT has several advantages compared to conventional
radiography. These include 3-dimensional image reconstruction, removal of
superimposed structures, sub-millimeter resolution and showing normal anatomy
and morphology of the root canal system without additional exposure. In
addition, it gives images of higher resolution than those obtained by
conventional periapical
radiographs. It provides much more detail about the root canal morphology
during endodontic procedure, and is more sensitive in detection of supplemental
canals compared to radiographic images [3-6,10].
In the case presented here, the permanent mandibular second
molar exhibited complicated root anatomy in CBCT imaging which was
not evident on periapical radiographs. But with CBCT it was found that both
distal root and its canal were straight. The mesial root was severely curved
from the middle to root apex fused with the distal root. As a result it
revealed Vertucci II canal configuration. Serial axial sections of CBCT also
showed that at the cervical part of the root two canal orifices (one mesial and
other distal) were found. As canals progressed apically the two canals merged
each other near the apex resulting in one canal. From this case it is
understood that occurrence of complex root canal anatomy are
possible during endodontic procedure and correct diagnosis of such variations
using advanced diagnostic technique like CBCT is highly useful for the valuable
treatment of the tooth. Conclusion
Successful endodontic
therapy involves complete pulp removal followed by three dimensional seal
of the endodontic space. CBCT is a valuable diagnostic aid in studying the root canal morphology
of human teeth in
order to enhance the success rate of endodontic therapy.
References
1. Manning SA. Root
canal anatomy of mandibular second molars. Part I. (1990) Int Endod J 23:
34-39.
2. Manning SA. Root canal anatomy of mandibular second
molars. Part II. C-shaped canals. (1990)
Int Endod J 23: 40-45.
3. Nur BG, Ok E, Altunsoy M, Aglarci OS, Colak M, et al.
Evaluation of the root and canal morphology of mandibular permanent molars in a
south-eastern Turkish population using cone-beam computed tomography (2014) Eur
J Dent 8: 154-159.
4. Mirzaie M, TorkZaban P, Mohammadi V. Cone-beam computed
tomography study of root canals in a Hamadani population in Iran (2012) AJDR 4:
25-31.
5. Ahmed HA, Abu-bakr NH, Yahia NA, Ibrahim YE. Root and
canal morphology of permanent mandibular molars in a Sudanese population (2007)
Int Endod J 40: 766-771.
6. Peiris HR, Pitakotuwage TN, Takahashi M, Sasaki K,
Kanazawa E. Root canal morphology of mandibular permanent molars at different
ages (2008) Int Endod J 41: 828-835.
7. Omer OE, Al Shalabi RM, Jennings M, Glennon J, Claffey
NM. A comparison between clearing and radiographic techniques in the study of
the root-canal anatomy of maxillary first and second molars (2004) Int Endod J 37: 291296.
8. Vertucci FJ. Root canal anatomy of the human permanent
teeth (1984) Oral Surg Oral Med Oral Pathol 58: 589-599.
9. Nagy CD, Szabó J, Szabó J. A mathematically based
classification of root canal curvatures on natural human teeth (1995) J Endod 21: 557-560.
10. Park JB, Kim N, Park S, Kim Y, Ko Y. Evaluation of root
anatomy of permanent mandibular premolars and molars in a Korean population
with cone-beam computed tomography (2013) Eur J Dent 7: 94-101.
Cone beam computed tomography, Endodontic Treatment, Mandibular Second Molar, Vertucci Classification


