
Explore journal overview, editorial leadership, indexing, articles in press, latest published work, and highlights from previous issues.
Case Report :
Shweta Jain,
Sachin Jain, Shikha Jainand Sophia Thakur Introduction: Presence of foreign body in the root canal system
is a troublesome situation as they prevent the access to thorough root canal
cleaning and shaping procedure apical to their level. They might also irritate
the periapex when they protrude out of the root apex. This affects final
outcome of endodontic therapy. Hence an attempt to bypass or retrieval of the
foreign body should be made before leaving and obturating till the level of
their presence or proceeding to surgery. The procedure for removal will vary
depending on the nature of the foreign body and its position within the canal.
Many different devices and techniques have been developed to retrieve foreign
bodies from the root canal system, but none of them can consistently remove
them from the canals. One
of the complications of endodontic therapy is having an
instrument fracture or presence of foreign body in the root canal space. Over the years,
as techniques and instrumentation have developed, there have been various types
of endodontic
instruments
that have broken off in the canal. These fractured instruments or foreign
bodies hinders the clinician from thoroughly cleaning and shaping the canal
system and thus compromises the outcome of the treatment. The prognosis of case
is dependent on the stage of canal instrumentation at the time when the foreign
body separates. It has been suggested that separation of foreign body occurring
in later stages of canal instrumentation, especially if it is at the apex, has
the best prognosis, because the canal is probably well debrided and free from
infection [1]. In
most cases it is difficult to determine the true extent of how well the canal
is disinfected, when the foreign body separates, especially if it is short of
working length and therefore it is important to be able to bypass or retrieve
the separated foreign body without further
damage to the tooth. The
removal of foreign body from the root canal system in most cases is difficult
and at times impossible. There are various methods and devices developed to
retrieve them. It
is the clinicians who have to evaluate the options of attempting to remove the
foreign body, bypassing it or leaving the fracture portion in the root canal
itself. This decision should be made with consideration for the pulp status,
canal infection, canal anatomy, the position of
the fractured foreign body and its type [2]. The
main determinant for removal of the foreign body is its location in relation to
the curvature of the root canal. The foreign body removal is possible if it is
located coronal to the curve, and becomes impossible if the separation is
beyond the curvature [3,4]. The
clinicians need to weigh out the advantages and disadvantages of retrieval of
foreign body fragments. It has been shown that attempts at removal of these
fragments usually result in the removal of a large amount of root dentin which ends up
reducing the root strength by 30-40% [1]. Hence the decision to retrieve the
fragments lies in the judgment of the clinician. Case
1 An
18-year-old male patient reported to the private clinic with discolored upper left central incisor. The case
history revealed that the tooth had been treated up till biomechanical preparation a year back. Patient
did not report for obturation to the clinician and later a gingival abscess developed with
the same tooth along with pain. The patient removed the temporary and used a
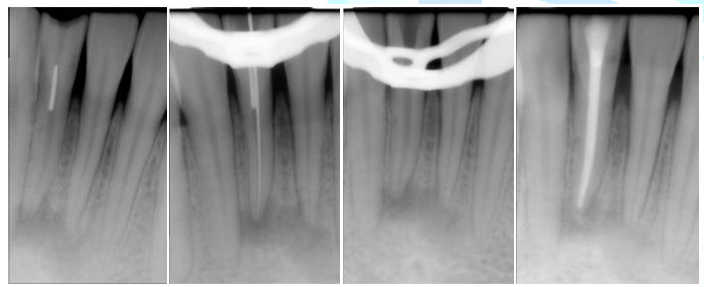
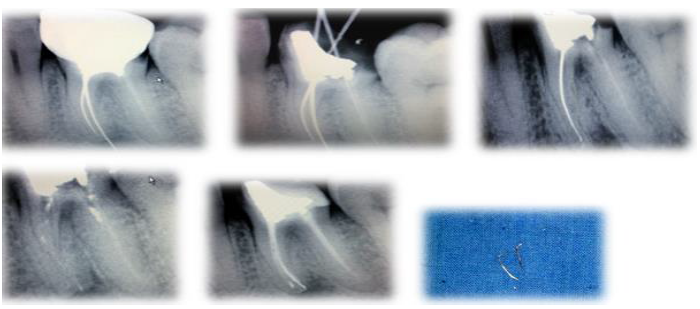
bobby pin to remove food lodged in the pulp chamber. The intraoral periapical radiograph revealed a
radio-opaque object in the canal identified as a bobby pin. Access cavity was
modified to achieve straight line access and with the help of small size K-file
and EDTA the pin was bypassed. H file was used on with circumferential filing
and pin was removed from root canal walls. Biomechanical preparation was
completed, and canal was disinfected by placing Ca(OH)2¬ intracanal
medicament for one week. Finally, the tooth was obturated with MTA followed by
post endodontic restoration. A
16-year-old male patient reported to the private clinic with discolored lower
anterior tooth. The intraoral periapical radiograph revealed a radio-opaque
object in the cervical third of the canal. On careful history from the patient,
it was revealed that the patient had inserted a piece of metallic pin in the
open pulp chamber of the lower
central incisor. After a conventional access cavity the pin was bypassed using
No. 8, 10 and 15 K files with Ethylene Diamine Tetra Acetic acid (EDTA). Once
bypassed the pin was successfully removed using 15# H file by engaging the pin.
Biomechanical preparation of the canal was then done followed by obturation and
post endodontic restoration. Case
3 A
25-year-old male patient reported to the private clinic with pain in lower left
posterior region. The case history revealed history of endodontic treatment 3-4 years back
in 46. Intraoral periapical radiograph was taken which indicated silver point
obturation in 46. The canal orifice was enlarged with the help of gate glidden
drill No. 1,2,3. The
ultra-sonic (piezoelectric) (SybronEndo) tip was used for the retrieval of the
silver points. It was introduced into the canal in contact with the canal wall,
activated for one or two minutes with a light touch. The objective was only to
transmit vibration to the silver points so that it may be dislodged from the
canal. This maneuver was repeated several times, until the canal space was
cleared of the silver points. After that canals were enlarged with protaper
system and obturation was done. Figure 3: An intraoral
periapical radiograph indicates silver point obturation in 46. One
of the most troublesome incidents is the fracture of endodontic instruments
within root canal. Separation incidences according to the number of teeth or
canals were significantly higher (P<.05) in molars than those in premolars or anterior teeth [5]. Many
foreign objects have also been reported to break and subsequently become lodged
in root canals. Presence of these foreign bodies might affect the prognosis of
endodontic treatment. Though not all the problems lead to a reduced prognosis,
but any error that compromises microbial control is likely to increase the risk
of a poor outcome. Technical
equipment should not be considered the only factor influencing success or
failure of removal procedures. The experience and skill of the operator as well
as the anatomical factors are also important, although the removal of foreign
objects sometimes is difficult, and the success rate has been reported as 55%
to 79% [6]. Many
methods are described to remove broken instruments or objects within root
canals, such as hand instrumentation, ultrasonic devices, Masserann Kit, canal
finder system or, sometimes surgical methods also are employed [7,2]. In
all cases, a careful examination with fine endodontic instrument should be the
first step. In order to observe in a high magnification, the microscope should
be used as an auxiliary tool. Gencoglu
and Helvacioglu [8] concluded that visualization of an operative microscope
influences the success of the fractured instrument management. Operating under
high power magnification enables precise use of ultrasonic, avoiding
unnecessary dentin removal thereby increasing the success rate by 67%-95%
[9,10]. The
removal of foreign bodies from a root canal must be performed with minimum
damage to the tooth and the surrounding tissues [1]. Ideally, the original
canal shape should be preserved as much as possible, just like during the cleaning
and shaping of a canal. Wilcox et al showed that canal enlargement of 40 to 50%
of the root width increased susceptibility to vertical fracture [11]. Several
studies showed that ledges were inevitably created in the process of file
removal attempts because of the staging platform. Ward et al. reported the use
of an ultrasonic
technique
in simulated canals and on extracted teeth can cause a portion of the separated
instruments to occasionally break off from the original fragment, leaving a
shorter fragment behind. This is frequently observed during the ultrasonic
removal of NiTi fragment [12,13]. Therefore,
these results suggest that it is necessary to avoid the direct contact of the
ultrasonic tip with the foreign objects. A shorter fragment is more difficult
to retrieve than a longer fragment, definitely complicating the job at hand [1]. Suter
[2] recommended that removal attempts of fractured instruments from root canals
should not exceed 45 to 60 minutes because the success rates may drop with
increased treatment time. He
suggested that the lowered success rate could be because of operator fatigue or
from over enlargement of the canal, which compromises the integrity of the
tooth and increase the risk of perforation. It is recommended that after this
period of time serious consideration should be given to other treatment
options. Since
the success of an endodontic
treatment
is dependent on degree of infection of the canal system at the time of foreign bodies
separation, if the signs of failure or symptoms are present in these cases,
surgery or extraction will be required to solve the problem. A
foreign body can be removed through K-files interlaced and it is able to
preserve the dental structure, however this
kind of procedure depends on the operator experience and also of what and where
metallic objects are found. Microscopy and ultrasonic tips are used as
auxiliary tools, increasing the chance of removal and ensuring the integrity of
the tooth structure. 1.
Terauchi
Y, OLeary L and Suda H. Removal of Separated Files from Root Canals with a New
File-removal System: Case Reports (2006) J Endod 32:789-797. https://doi.org/10.1016/j.joen.2005.12.009 2.
Suter
B, Lussi A and Sequeira P. Probability of removing fractured instruments from
root canals (2005) Int Endod J 38: 112-123. https://doi.org/10.1111/j.1365-2591.2004.00916.x 3.
Cheung
GSP. Instrument fracture: mechanisms, removal of fragments, and clinical
outcomes (2009) Endod topics 16: 1-26. https://doi.org/10.1111/j.1601-1546.2009.00239.x 4.
Madarati
AA, Qualtrough AJE and Watts DC. Vertical fracture resistance of roots after
ultrasonic removal of fractured instruments (2010) Int Endod J 43: 424-429. https://doi.org/10.1111/j.1365-2591.2010.01698.x 5.
Wu
J, Lei G, Yan M, Yu Y, Yu J, et al. Instrument separation analysis of
multi-used ProTaper Universal rotary system during root canal therapy (2011) J
Endod 37: 758-763. https://doi.org/10.1016/j.joen.2011.02.021 6.
Nagai
O, Tani N, Kayaba Y, Kodama S and Osada T. Ultrasonic removal of broken
instruments in root canals (1986) Int Endod 19: 298-304. https://doi.org/10.1111/j.1365-2591.1986.tb00493.x 7.
Hulsmann
M. The removal of silver cones and fractured instruments using the canal finder
system (1990) J Endod 16: 596-600. https://doi.org/10.1016/S0099-2399(07)80203-2 8.
Gencoglu
N and Helvacioglu D. Comparison of the different techniques to remove fractured
endodontic instruments from root canal systems (2009) Eur J Dent 3: 90-95. 9.
Ha
JH, Kwak SW, Kim SK and Kim HC. Screwing in forces during instrumentation by
various file systems. (2016) Restor Dent Endod 41: 304-309. https://dx.doi.org/10.5395%2Frde.2016.41.4.304 10.
Natanasabapathy
V, Sundar S and Koteeswaran V. Retrieval of fractured Ni-Ti rotary instrument
using ultrasonics and file braiding technique under surgical operating
microscope (2017) Endodontol 29: 65-68. 11.
Wilcox
LR, Roskelley C and Sutton T. The relationship of root canal enlargement to
finger-spreader induced vertical root fracture (1997) J Endod 23: 533-534. https://doi.org/10.1016/S0099-2399(97)80316-0 12.
Ward
JR, Parashos P and Messer HH. Evaluation of an ultrasonic technique to remove
fractured rotary nickel-titanium endodontic instruments from root canals: an
experimental study (2003) J Endod 29: 756-763. https://doi.org/10.1097/00004770-200311000-00017 13. Nevares G, Cunha RS, Zuolo ML and Bueno CE.
Success rates for removing or bypassing fractured instruments: a prospective
clinical study (2012) J Endod 38: 442-444.
https://doi.org/10.1016/j.joen.2011.12.009 Sachin
Jain, Professor, Deptartment of Conservative Dentistry and Endodontics, Shri
Bakebihari Dental College, Gaziabadh, India, E-mail: drjaindig@gmail.com,
Tel: 09536031608 Jain
S, Jain S, Jain S and Thakur S. Gripping the gripped: removal of foreign bodies
from root canal system (2019) Dental Res Manag 3: 13-15 Foreign bodies, Retrieval, Instrument fracture,
Canal obstructionGripping the Gripped: Removal of Foreign Bodies from Root Canal System
Abstract
Case Presentation: Three cases requiring removal of foreign bodies
from the different positions in the canals are presented. These cases present
the conservative management of an inadvertently lodged foreign body in the root
canal system during a routine dental procedure and describe the management
strategies for their retrieval.
Conclusion:
Provided one has good patient cooperation, management of the situation can be
quite straight forward if the appropriate diagnostic and treatment tools are utilized. Full-Text
Introduction
Case
Reports

Case
2
Discussion
Conclusion
References
*Corresponding author
Citation
Keywords

