"Cambria Math"/>

Explore journal overview, editorial leadership, indexing, articles in press, latest published work, and highlights from previous issues.
Research Article :
"Cambria Math"/>
With the ongoing evolution of ever faster and more sophisticated multi–detector row Computed Tomography (CT) technologies, CT of the heart has evolved into an examination that is applied to a broad variety of clinical situations [1]. With the advantage of the latest iterations of multi-detector CT technology, both the temporal resolution and the spatial resolution of coronary CT angiography (hereafter CT Angiography) have improved to a point where the threshold for routine noninvasive assessment of the coronary arteries for atherosclerotic disease may have been crossed [2].
Imaging of the heart has always been technically challenging because of the continuous cardiac motion. The development of Electrocardiographically (ECG) synchronized Multi-Detector CT (MDCT) scanning and reconstruction techniques have yielded fast volume coverage and high spatial and temporal resolution for successful cardiac imaging [3-6].
The exceedingly powerful technology that enables one to perform CT angiography, however, transcends routine CT applications and thus needs to be used in a manner that facilitates optimized results with the lowest degree of invasiveness for the patient [4].
Patients who may benefit from CT angiography for cardiac evaluations can be classified under several broad categories. These include; screening of asymptomatic patients, examination of symptomatic patients, and specialized applications [5].
The discriminatory power of CT coronary angiography to identify patients with obstructive (above 50 %) coronary stenosis should be regarded as "high diagnostic evidence", to identify patients without coronary stenosis as "persuasive diagnostic evidence". The discriminatory power of both types of coronary angiography to identify patients with or without functionally relevant coronary stenosis should be regarded as "weak diagnostic evidence" [3-6].
It can be assumed that patients with a high pretest probability of CAD will need invasive coronary angiography and patients with a low pretest probability of CAD will not need subsequent revascularization. Therefore, CT coronary angiography may be used according to the pretest probability of CAD, for identifying or excluding obstructive coronary stenosis [7-11].
CT coronary angiography was shown to be more cost-saving at a pretest probability of CAD of 50 % or lower and invasive coronary angiography at a pretest probability of CAD of 70 % or higher stenosis [10-14]. The use of both types of coronary angiography to identify or to exclude functionally relevant coronary stenosis should be regarded as highly cost- consuming with regard to ethical, social or legal aspects, the following possible implications were identified: under-provision or over-provision of health care, unnecessary complications, anxiety, social stigmatization, restriction of self- determination, and unequal access to health care [4-10].
This single center retrospective study was done at the international medical center in Jeddah Saudi Arabia over 2 years started from May of 2015 up to May of 2017. Patients referred for invasive coronary angiogram after already had CT coronary angiogram. The medical evaluation was based on systematic reviews of all diagnostic studies with invasive coronary angiography and those with CT coronary angiogram. Data on special indications (bypass graft, in-stent-restenosis) were also included in the evaluation. CT scanners used with at least 320 slices.
Inclusion data:
1. Diabetic or not
2. Hypertensive or not
3. Smoker or not
4. Ejection Fraction
5. Serum creatinine and GFR
In the study we included 99 patients who underwent CT coronary angiogram, which was positive for any coronary artery disease followed by invasive coronary angiogram, some of these patients had normal CT coronary angiogram with ongoing chest pain, which needed evaluation by invasive coronary angiogram, so we considered those patients as our control group.
Results were analyzed using the simple sensitivity and specificity methods with positive and negative predictive value. During statistical analysis, Left main (LM) was divided to proximal and distal segment, Left Anterior Descending (LAD) was divided to proximal, mid and distal together with diagonal branches, Left Circumflex (LCX) was divided to proximal and distal segment together with the obtuse marginal branches and finally Right Coronary Artery (RCA) was divided to proximal mid and distal segments as well as bypass grafts.
We had analyzed more than 1205 segments of the 99 patients, which gave us more accurate assessment and results as compared to the previous major studies.
Results
Of the 99 patients, 80 were male and 19 were female, 70 patients were hypertensive, 57 diabetic, 77 dyslipidaemic and 34 were smokers (Table 1, Figures 1-3).
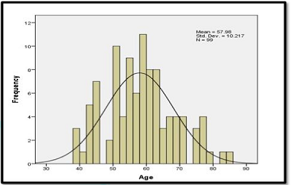
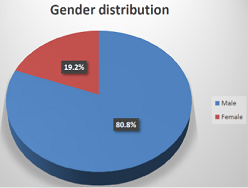
Figure 2: Gender distribution.
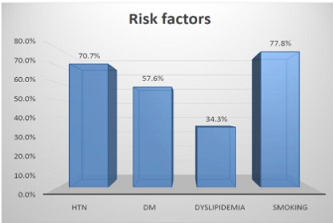
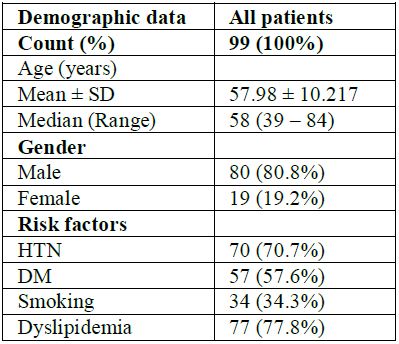
Table 1: Baseline demographic data.
Among the total lesion, sensitivity was 87.1%, specificity was 98.1%, positive predictive value was 88.2 %, negative predictive value was 98.8% and accuracy 96.5% (Table 2 and 3). 198 different LM segments were included in this study which had the lowest sensitivity (83%) and specificity of 100% (Table 4 and 5).

Table 2: Concordance between invasive CA and CTCA in the total lesions.

Table 3: Assessment of CTCA total diagnostic performance.

Table 4: Concordance between invasive CA and CTCA regarding the LM lesions.

Table 5: Assessment of CTCA LM lesions diagnostic performance.
17 different graft segments were included in this study which had the highest sensitivity and specificity of almost 100% (Figure 4, Table 6 and 7).
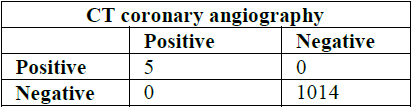
Table 6: Concordance between invasive CA and CTCA regarding the Grafts lesions.

Table 7: Assessment of CTCA grafts lesions diagnostic performance.
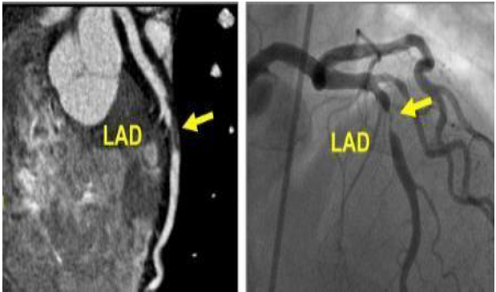
Figure 4: Left anterior descending (LAD) artery.
Total 396 LAD was divided to proximal, mid and distal segments in addition to the diagonal branch. The LAD had good sensitivity of 89.2 % and specificity of 95% with a positive predictive value of 80.5%, negative predictive value of 97.5% and 93.9% accuracy (Figure 5, Table 8 and 9).
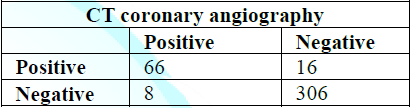
Table 8: Concordance between invasive CA and CTCA regarding the LAD lesions.

Table 9: Assessment of CTCA LAD lesions diagnostic performance.
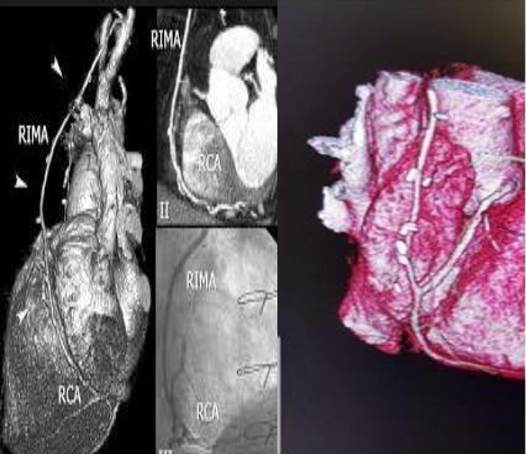
Figure 5: Right internal mammary artery (RIMA) graft evaluation.
The LCX was divided to proximal and distal segment together with the OM branch. LCX had good sensitivity of 84.2% and very good specificity of 99.6% with a positive predictive value of 97% and negative predictive value of 97.7% and 97.6% accuracy (Table 10 and 11).
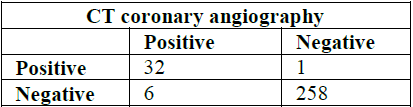
Table 10: Concordance between invasive CA and CTCA regarding the LCX lesions.

Table 11: Assessment of CTCA LCX lesions diagnostic performance.
The RCA was divided to proximal and distal segments together with the PDA branch. RCA had good sensitivity of 85.4% and very good specificity of 98.8% with a positive predictive value of 93.2% and negative predictive value of 97.2% and 96.6% accuracy (Table 12 and 13).
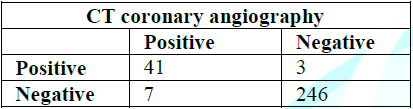
Table 12: Concordance between invasive CA and CTCA regarding the RCA lesions.

Table 13: Assessment of CTCA RCA lesions diagnostic performance.
19 patients had normal or non-obstructive coronary artery disease in the CT but due to ongoing chest pain and presence of risk factors we did invasive coronary angiogram to all 19 patients and all revealed the same results.
6 patients had high calcium score in the CT coronary, 4 of them had multi vessel disease in the invasive coronary angiogram and 2 had moderate CAD for medical management.
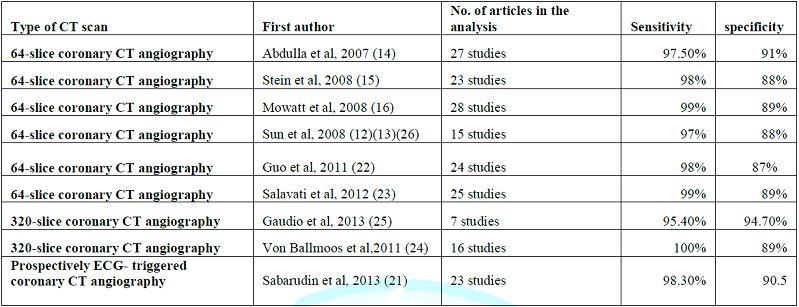
Currently, 320-slice CT represents the recent technological developments in imaging coronary artery disease with good results achieved. Expansion of multislice CT systems from a 64-slice to 320-slice system has allowed for the accurate assessment of stenosis severity and atherosclerotic plaque composition, or even the acquisition of whole-heart coverage in one gantry rotation [11-26]. Two recently reported systematic reviews and meta-analyses further confirmed the high diagnostic accuracy of 320-slice CCTA [26,27] (Table 14).
The diagnostic sensitivity was similar to that reported in the 64-slice CCTA, but the specificity was higher in 320-slice CCTA than in 64-slice CCTA studies, indicating the high value of 320-slice CCTA for excluding coronary artery stenosis [19,25,26,28]. However, it has to be recognized that diagnostic performance of 320-slice CCTA is similar to that of 64- and 128-slice for the determination of ≥50% coronary artery
Stenosis due to its limited temporal resolution, despite improved extended z-axis coverage [28].
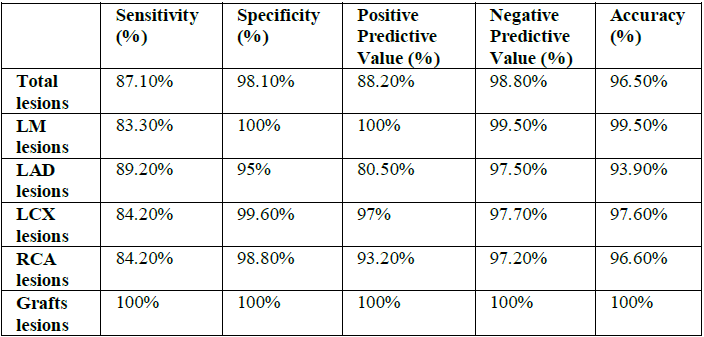
Table 14: Summary of CTCA diagnostic performance regarding coronary lesions.
Coronary CT angiography has developed as reliable less-invasive imaging modality in the diagnosis of coronary artery disease. Tremendous progress has been made over the last decades in the technological improvements in cardiac CT imaging, thus enabling coronary CT angiography to become a potential alternative to invasive coronary angiography in selected patients [17,18]. 320-slice MDCT has a high discriminative power to detect obstructive coronary artery diseases in comparison with invasive coronary angiography as revealed in our finding. To be a clinically useful tool for the diagnosis of patients with suspected CAD, complete visualization of all therapeutic relevant coronary arteries without excluding segments is necessary [19,20]. In the present study, we evaluated all arteries being >1.5 mm in diameter, thereby finding a sensitivity and specificity of 87.1% and 98.1% was expected.
Similar to our study Niemann et al reported a sensitivity of 81%, a specificity of 97%, a positive predictive value of 81% and a negative predictive value of 97% for detection of stenoses >50% in 35 patients [2]. Achenbach et al. found a sensitivity of 91% and a specificity of 84% in 64 patients [29]. Several other studies have compared the degree of stenosis detected by quantitative coronary angiography with that detected by 16- or 64- slice CT [30-33]. The overall correlation between 64 slice MDCT and invasive coronary angiography varies in different studies and appears to be moderate, even for selected segments with high image quality [30,31].
The sensitivities of 64-slice MDCT for the detection of stenosis of less than 50%, stenosis of greater than 50%, and stenosis of greater than 75% have been reported to be 79%, 73%, and 80%, respectively, and the specificity has been reported to be 97% by Leber et al [32].
Some recent studies have reported excellent diagnostic accuracy for 64-slice MDCT in the detection of significant stenosis in smaller coronary artery segments and side branches as well (86%– 94% sensitivity and 93%-97% specificity) [30,32,33] (Table 15). In our study we evaluated small coronary vessels like obtuse marginal vessels and diagonal branches for stenosis. Our results to detect stenosis among these small vessels were also comparable with Raff et al findings [30]. Our study documents an excellent ability of 320 slice MDCT to rule out functionally relevant CAD as indicated by the high NPV. The high negative predictive values of 98.8% suggests an important future role of CT coronary angiography for reliably excluding CAD in patients with an equivocal clinical presentation, who may currently undergo a cost-extensive invasive coronary angiography. Our study result of high NPV was also comparable with some other studies [30-33]. On the other side an abnormal 64-320-slice CTA is a moderate predictor of functionally relevant coronary stenosis (PPV=88.2%). Patients with positive CT angiogram should be scrutinized and might not need to go for further evaluation including invasive CA.
From a medical point of view, CT coronary angiography using scanners with at least 320 slices should be recommended as a test to rule in obstructive coronary stenosis in order to avoid inappropriate invasive coronary angiography in patients with an intermediate pretest probability of CHD. Multi detector CT (MDCT) has reasonably high accuracy for detecting significant obstructive CAD when assessed at artery level.
1. Schoepf U. CT of the heart: principles and applications (2004) Totowa NJ: Humana 120: 1010-1012. DOI: 10.1385/1592598188
2. Nieman K, Cademartiri F, Lemos PA, Raaijmakers R, Pattynama PMT, et al. Reliable noninvasive coronary angiography with fast submillimeter multislice spiral computed tomography (2012) Circulation 106: 2051-2054. https://doi.org/10.1161/01.CIR.0000037222.58317.3D
3. Johnson TR, Nikolaou K, Wintersperger BJ, Leber AW, Von Ziegler F, et al. Dual-source CT cardiac imaging: initial experience (2006) Eur Radiol 16: 1409-1415. https://doi.org/10.1007/s00330-006-0298-y
4. Ohnesorge B, Flohr T, Becker C, Kopp AF, Schoepf UJ, et al. Cardiac imaging by means of electrocardiographically gated multisection spiral CT: initial experience (2014) Radiology 217: 564-571. https://doi.org/10.1148/radiology.217.2.r00nv30564
5. Ohnesorge BM, Hofmann LK, Flohr TG and Schoepf UJ. CT for imaging coronary artery disease: defining the paradigm for its application (2012) Int J Cardiovasc Imaging 21: 85-104. https://doi.org/10.1007/s10554-004-5346-6
6. Schoepf UJ, Becker CR, Ohnesorge BM and E Kent Yucel. CT of coronary artery disease (2014) Radiology 232: 18-37. https://doi.org/10.1148/radiol.2532081738
7. Jacobson TA, Griffiths GG, Varas C, Gause D, Sung JC, et al. Impact of evidence-based “clinical judgment” on the number of American adults requiring lipid-lowering therapy based on updated NHANES III data (2011) Arch InternMed 160: 1361-1369. https://doi.org/10.1001/archinte.160.9.1361
8. Spalding L, Reay E and Kelly C. Cause and outcome of atypical chest pain in patients admitted to hospital (2013) J R Soc Med 96: 122-125.
9. Kroenke K and Mangelsdorff AD. Common symptoms in ambulatory care: incidence,evaluation, therapy, and outcome (2005) Am J Med 86: 262-266. http://dx.doi.org/10.1016/0002-9343(89)90293-3
10. Braunwald E, Antman EM, Beasley JW, Califf RM, Cheitlin MD, et al. ACC/AHA 2002 guideline update for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction (2012) J Am Coll Cardiol 40: 1366-1374.
11. Quiroz R, Kucher N, Zou KH, Kipfmueller F, Costello P, et al. Clinical validity of a negative computed tomography scan in patients with suspected pulmonary embolism: a systematic review (2005) JAMA 293: 2012-2017. https://doi.org/10.1001/jama.293.16.2012
12. Sun Z, Cao Y and Li HF. Multislice computed tomography angiography in the diagnosis of coronary artery disease (2011) J Geriatr Cardiol 8: 104-113. https://dx.doi.org/10.3724%2FSP.J.1263.2011.00104
13. Sun Z and Jiang W. Diagnostic value of multislice CT angiography in coronary artery disease: A meta-analysis (2006) Eur J Radiol 60: 279-286. https://doi.org/10.1016/j.ejrad.2006.06.009
14. Abdulla J, Abildstrom Z, Gotzsche O, Christensen E, Kober L, et al. 64-multislice detector computed tomography coronary angiography as potential alternative to conventional coronary angiography: a systematic review and meta-analysis (2007) Eur Heart J 28: 3042-3050. https://doi.org/10.1093/eurheartj/ehm466
15. Stein PD, Yaekoub AY, Matta F and Sostman HD. 64-slice CT for diagnosis of coronary artery disease: a systematic review (2008) Am J Med 121: 715-725. https://doi.org/10.1016/j.amjmed.2008.02.039
16. Mowatt G, Cook JA, Hillis GS, Walker S, Fraser C, et al. 64-slice computed tomography angiography in the diagnosis and assessment of coronary artery disease: systematic review and meta-analysis (2008) Heart 94: 1386-1393. https://doi.org/10.1136/hrt.2008.145292
17. Vanhoenacker P, Heijenbrok-Kal M, Van Heste R, Decramer I, Van Hoe LR, et al. Diagnostic performance of multidetector CT angiography for assessment of coronary artery disease: meta- analysis (2007) Radiology 244: 419-428. https://doi.org/10.1148/radiol.2442061218
18. Johnson T, Nikolaou K, Busch S, Leber AW, Becker A, et al. Diagnostic accuracy of dual-source computed tomography in the diagnosis of coronary artery disease (2007) Invest Radiol 42: 484-491. https://doi.org/10.1097/RLI.0b013e31806907d0
19. Pelliccia F, Pasceri V, Evangelista A, Pergolini A, Barillà F, et al. Diagnostic accuracy of 320-row computed tomography as compared with invasive coronary angiography in unselected, consecutive patients with suspected coronary artery disease (2013) Int J Cardiovasc Imaging 29: 443-452. https://doi.org/10.1007/s10554-012-0095-4
20. Motoyama S, Sarai M, Harigay H, Anno H, Inoue K, et al. Computed tomographic angiography characteristics of atherosclerotic plaques subsequently resulting in acute coronary syndrome (2009) J Am Coll Cardiol 54: 49-57. https://doi.org/10.1016/j.jacc.2009.02.068
21. SabarudinA, Sun Z and Ng KH. Coronary CT angiography with prospective ECG- triggering: A systematic review of image quality and radiation dose (2013) Singapore Med J 54: 15-23.
22. Guo SL, Guo YM, Zhai YN, Ma B, Wang P, et al. Diagnostic accuracy of first generation dual- source computed tomography in the assessment of coronary artery disease: a meta- analysis from 24 studies (2011) Int J Cardiovasc Imaging 27: 755-771. https://doi.org/10.1007/s10554-010-9690-4
23. Salavati A, Radmanesh F, Heidari K, Dwamena BA, Kelly AM, et al. Dual-source computed tomography angiography for diagnosis and assessment of coronary artery disease: systematic review and meta-analysis (2012) J Cardiovasc Comput Tomogr 6: 78-90. https://doi.org/10.1016/j.jcct.2011.10.018
24. vanBallmoos MW, Haring B, Juillerat P and Alkadhi H. Meta-analysis: diagnostic performance of low-radiation-dose coronary computed tomography angiography (2011) Ann Intern Med 154: 413-420. https://doi.org/10.7326/0003-4819-154-6-201103150-00007
25. Gaudio C, Pellicia F, Evangelista A, Tanzilli G, Paravati V, et al. 320-row computed tomography angiography vs conventional coronary angiography in patients with suspected coronary artery disease: a systematic review and meta-analysis (2013) Int J Cardiol 168: 1562-1564. https://doi.org/10.1016/j.ijcard.2012.12.067
26.Sun Z and Jiang W. Diagnostic value of multislice CT angiography in coronary Artery disease: A meta-analysis (2006) Eur J Radiol 60: 279-286.https://doi.org/10.1016/j.ejrad.2006.06.009
27. Li S, Ni Q, Wu H, Dong R, Chen L, et al. Diagnostic accuracy of 320-slice computed tomography Angiography for detection of coronary artery (2013) Int J Cardiol 168: 2699-2705. https://doi.org/10.1016/j.ijcard.2013.03.023
28. Sun Z. Comment on: Diagnostic accuracy of 320-slice computed tomography angiography for detection of coronary artery stenosis: meta-analysis (2013) Int J Cardiol 168: 4895-4896. https://doi.org/10.1016/j.ijcard.2013.07.023
29. Achenbach S, Moselewski F, Ropers D, Ferencik M, Hoffmann U, et al. Detection of calcified and noncalcified coronary atherosclerotic plaque by contrast-enhanced, submillimeter multidetector spiral computed tomography: a segment-based comparison with intravascular ultrasound (2004) Circulation 109: 4-17. https://doi.org/10.1161/01.CIR.0000111517.69230.0F
30. Raff GL, Gallagher MJ and O’Neill WW. Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography (2005) J Am Coll Cardiol 46: 552-557. https://doi.org/10.1016/j.jacc.2005.05.056
31. Kefer J, Coche E and Legros G. Head-to-head comparison of three dimensional navigator-gated magnetic resonance imaging and 16-slice computed tomography to detect coronary artery stenosis in patients (2005) J Am Coll Cardiol 46: 92-100. https://doi.org/10.1016/j.jacc.2005.03.057
32. Leber AW, Becker A, Knez A, von Ziegler F, Sirol M, et al. Accuracy of 64-slice computed tomography to classify and quantify plaque volumes in the proximal coronary system: a comparative study using intravascular ultrasound (2006) J Am Coll Cardiol 47: 672-677. https://doi.org/10.1016/j.jacc.2005.10.058
Leschka S, Allkadhi H, Plass A, Desbiolles L, Gru’nenfelder J, et al. Accuracy of MSCT coronary angiography with 64-slice technology: first experience (2005) European Heart J 26: 1482-1487. https://doi.org/10.1093/eurheartj/ehi261
*Corresponding author
Hassan W, Professor of Medicine and Senior Consultant, Director of the Cardiac Center of Excellence, Jeddah 21451, Saudi Arabia, Fax: + 966-12-650-9789, Tel: +966-12-650-9000, E-mail: whassan@imc.med.sa
Citation
Zaghloul SM, Hassan W, Reda AM, Sultan GM, Salah MA, et al. CT Coronary Angiography versus Coronary Angiography to Detect Specificity and Sensitivity of CT Coronary (2019) Clinical Cardiol Cardiovascular Med 3: 1-6
CT Coronary angiography, Computed tomography, Coronary artery disease, Multi detector CT