Background
Nutrition is the intake of food
considered in relation to the bodys dietary needs. Good nutrition: an adequate,
well balanced diet combined with regular physical activity, is a cornerstone of
good health. Poor nutrition can lead to reduced immunity, increased
susceptibility to disease, impaired physical and mental development, and
reduced productivity (WHO, 2015).
Globally, under nutrition which
refers to both: protein energy malnutrition and micronutrient deficiency, is
the cause of around 3.1 million child deaths annually in low and middle-income
countries (Black et al, 2013).
When nutritional reserves are
depleted or nutrient intake is inadequate to meet the bodys daily metabolic
needs a state of under nutrition develops. Nutrient deficiency may stem from
inadequate ingestion, impaired digestion or absorption, dysfunctional metabolic
processing, or increased excretion of essential nutrients. Infants, children,
pregnant females, individuals with low incomes, hospitalized persons, and older
adults are at the greatest risk of becoming undernourished. Undernourishment
may result in impaired growth and development, lowered resistance to infection,
poor wound healing, and poor clinical outcome from disease or trauma with
increased morbidity and mortality (Mahan et al, 2012). The long-term energy and
nutrient depletion of eating disorders and the resulting malnutrition can have
lasting effects on growth (More, 2013).
Malnourished children, particularly
those with severe acute malnutrition, have higher risk of death from common
childhood illness such as diarrhoea, pneumonia, and malaria. Nutrition-related
factors contribute to about 45% of deaths in children under 5 years of age
(WHO, 2016).
Since the 1950s the case-fatality
rates in hospitals treating sever acute malnutrition (SAM) remained unchanged
in developing countries (onaverage 20–30%). In 1992, this failure to translate
scientific knowledge of what is needed to treat malnutrition in to effective
large-scale interventions(Collinset al, 2007).Important achievements have been
observed in the management of acute malnutrition over the last decade,
particularly in the development of ready-to-use therapeutic foods (RUTF). The
use of RUTF has facilitated decentralized ambulatory management of acute malnutrition
and has promoted a community approach called community-based management of
acute malnutrition (CMAM) (Kouam et al,
2014).
Community based Management of Acute
Malnutrition (CMAM) is an innovative approach for managing acute malnutrition
in children within the community. CMAM results in early detection of cases of
acute malnutrition, expanded access to treatment in decentralized sites,
greater community involvement and support, and extended coverage. A
comprehensive CMAM approach consists of community outreach, Outpatient Care
management of severe acute malnutrition (SAM) without medical complications,
Inpatient Care management of SAM with medical complications, and management of
moderate acute malnutrition (MAM) (FANTA, 2011).
The community-based management of
severe acute malnutrition is an attempt to achieve sustainable impacts at a
population level by taking the socioeconomic realities into account, balancing
the potentially conflicting demands and ethics of clinical and public
health(Collins et al, 2007).
The approach of community-based
involves timely detection of active case finding in the community, Community
health workers or volunteers can easily identify the children affected by acute
malnutrition using simple colored plastic strips that are designed to measure
mid-upper arm circumference (MUAC) and another sign can be recognized
through nutritional oedema of the feet.
Once children are identified as suffering from acute malnutrition, they need to
be seen by a health worker who has the skills to fully assess them following
the Integrated Management of Childhood Illness (IMCI) approach. The health
worker should then determine whether they can be treated in the community
through the provision of treatment for those without medical complications with
ready-to-use therapeutic foods (RUTF) or other nutrient-dense foods at home, or
whether referral to inpatient care is required. RUTF have a similar nutrient
composition to F100, which is the therapeutic diet used in hospital settings.
But unlike F100, RUTF are not water-based, meaning that bacteria cannot grow in
them. Therefore, these foods can be used safely at home without refrigeration
and even in areas where hygiene conditions are not optimal.Early detection,
coupled with decentralized treatment, reduced and prevent of hundreds of
thousands of deaths. Evidence shows that about 80 percent of children with
severe acute malnutrition who have been identified through active case finding,
or through sensitizing and mobilizing communities to access, decentralized
services themselves, can be treated at home (WHO, WFP, UNSSC and UNICEF, 2007).
Justification
Rural Kassala locality is the
second area in the Eastern Sudan states, implemented CMAM, after the pilot
conducted in North Delta locality. Two coverage surveys were conducted, to
investigate the number of children with severe acute malnutrition who were
being reached by the program. The data which used are routine program data
(such as admissions over time, MUAC on admission, proportion of discharges of
defaulters, non-response and cures, length of stay and location of admissions)
and qualitative data collected from beneficiary careers, program delivery staff
and various community members (including traditional healers, TBAs, Imams and
school-teachers) from which to make an estimate of program coverage (UNICEF,
2011). The role of community outreach workers / volunteers were not assessed,
therefore this drew the researcher attention to assess the volunteers
General
objective
To evaluate the effectiveness of
community outreach workers / volunteers in improving and increasing the
coverage of the CMAM program, in Rural Kassala locality, Kassala state.
Specific
objectives
·
To assess the
community outreach workers / volunteers performance, on the identification of
cases, Health /Nutrition education, follow up home visit, and trace defaulters.
·
To identify the
linkage between the community outreach workers/volunteers and the center
running the therapeutic feeding.
Methodology
Study
design
This study is a community based -
cross sectional study targeting the communities covered by CMAM program in
Rural Kassala locality, Kassala state.
Study
area
The study carried out in the rural
Kassala locality, villages covered by CMAM program. The rural Kassala locality was established
and set its boundary on the year 2007. It is approximately 3,650 square
kilometers with a population figure of 156 thousand. The locality has consisted
of 56 villages/communities, from which 21 communities were covered by CMAM
program.
Study
population
The populations of the study are of
two types: community outreach workers / volunteers who are part of the CMAM
program and households who inhabit in Rural Kassala locality and have children
under five, in the period October 2016 – February 2017.
Sample size
Sample size was calculated using
SMART software, (ENA SMART software (July 2015) version). A total children
(6-59months) of 24,246was used for the sampling frame with an expected 18.7%
prevalence of malnutrition (MUAC, S3M 2013, for Rural Kassala),a precision of
4.5% was used, with a design effect of 1.5.
The average household size was six people (taken from MICS 2014). The
proportion of under five year olds was taken as 17%, the MoH guideline. A 1%
contingency was included in case of non-response or invalid data. This gave a
sample size of 288 children (6 -59 months). (See Appendix 2)
Selection
of households
Upon reaching the selected village,
went to the center of the village. At the center of the village a pen was spun
and walked to the edge of the village in the direction shown by the pen,
counting the houses along this line. The first house was selected randomly by
drawing a number, from 1 to the total houses counted, blindly; the number
picked became the first household and thereafter of 5 household intervals used.
If a household with no children 6 -59 months, household with the nearest door
was selected until all the samples completed.
The study included 200 households
with 309 children 6 - 59 months. There was slight increase on the number of
children 6 -59 months from the original sample this was due to the number of
children 6 -59 months at last house found to be more than needed, so included
all.
For the community outreach workers
/ volunteers, all volunteers were included (n=62).
Data
collection
Primary data collection: The data
have been collected using a structured questionnaire that developed by the
researcher containing closed and open ended questions to the household with
children 6 -59 months and community outreach worker / volunteers (See appendix
1).
The questionnaires of the household
consisted of information about household demographic characterizes, knowledge
of the CMAM program and the role of the community volunteer. Beside that other
informations collected related to the nutritional status of their children and
whether he/she registered in the nutrition program or not. MUAC and bilateral
edema used as anthropometric assessment.
The questions of the community
outreach worker / volunteer, inquire about the role of the volunteer, coverage
areas, a way of taking the MUAC measurement and its linkage with the program
and the nutrition worker and the problem facing to do their jobs.
Pilot was conducted in areas not to
be included in the study, sample of 10 households and 5 community volunteers in
Kassala town centers, no major problem found then used as a final questionnaire
to collect the informations.
Results
Data
for Household interviewed
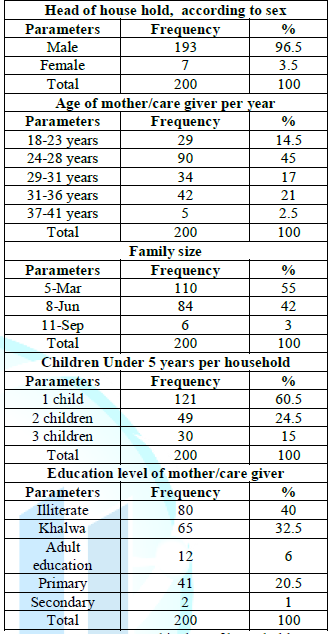
A total of 200 households were
included for the study, the results show that (96.5%) of the household are
headed by males and (3.5%) were female headed. Almost half of the mothers, 45%
in the present study were at age group of 24-28 years, and one quarter of age
group of 31-36 years. Regarding family size, 55% of the households had a family
size around 3-5 persons, and 42% had 6-8 persons and only 3% were more than 8
persons. As for the presence of children under 5 per household, 60% of the
households had only 1 child age under 5 years and one quarter had 2 children
under five years. The Educational level
of the mothers /caregiver was reported as 40% were illiterate, 30 % had with
primary level of education and only 1% had a secondary level of education.
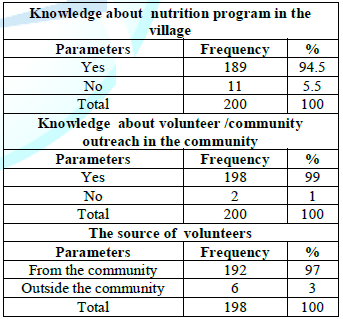
Table (2) reveals that 94.5% were
well knowledgeable of the Nutrition Therapeutic feeding programme at the
centres and only5.5% were not knowledgeable about this program .The majority of
the household (99%) well oriented by the presence of community outreach worker
/ volunteers in the community. The result also demonstrates 97% of the
community outreach worker / volunteers were from the community.
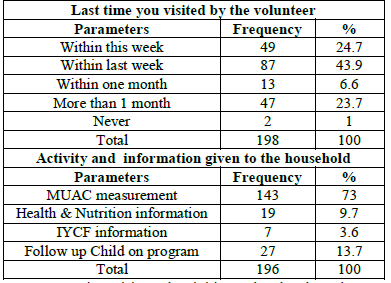
Last visits and activities
undertaken by community outreach workers / volunteers were shown in table (3).
Less than half of the study households 43.9% were visited by the community
outreach workers / volunteers within last week from the date of the interview,
and a quarter of the sample 24.7% and 23.7% were visited on the same week and
before one month from the date of interview respectively, and only 1% from the
total interviewed household mentioned that never visited by the community
outreach workers / volunteers. The activity of MUAC measurement was undertaken
by the community outreach workers / volunteers as mentioned by 73% of
household, 13.7% of households were visited by community outreach workers /
volunteer to follow up children on nutrition programme and the rest 13.3%
raised their awareness by either health and nutrition or IYCF information.
To view Table 1, Click below
Table 1: Demographic data of household.

Table 2: Knowledge of Nutrition program and volunteers.
To view Table 3, Click below
Table 3: Last time visits and activities undertaken by volunteers.
Under
five children Data
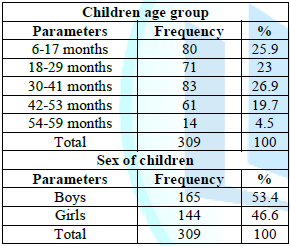
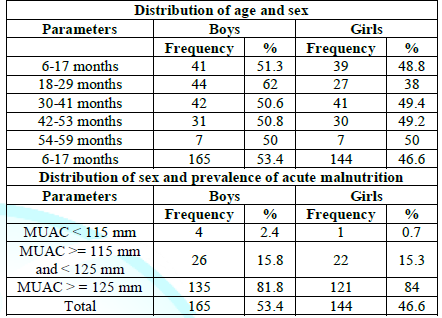
Regarding socio-demographic data,
gender distribution among the selected children, table (4) shows that 53.4% of
the children were males, while 46.6% were females. Their age group was
classified as follows 25.9% of the children were in the age group ( 6-17
months) , 23% in the age group (18 - 29
months), 26.9% in the age group (30-41
months), 19.7% in the age group (42 - 53 months) and 4.5 % at age group ( 54
- 59 months ).

Table 4: Age and sex of children under 5 years.
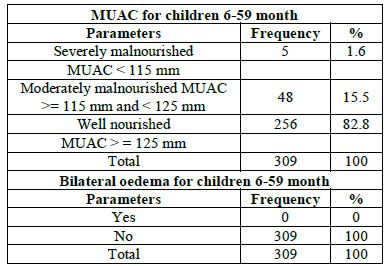
A total of 309 children of age from
6 – 59 months have their MUAC checked and bilateral oedema to find out their
nutritional status table (5). Based on MUAC cutoff 1.6% was found to be
severely wasted and 15.5% was moderately wasted, with no case report with
oedema.

Table 5: Prevalence of acute malnutrition based on MUAC cut off and/or oedema.
Table 6 the distribution of the
sample by sex shows no significant differences was found in the number of boys
and girls, P = 0.603 showing that boys and girls were equally represented.
Also, there were no significant differences in the prevalence of acute
malnutrition between boys and girls (p=0.477).
Table (7) regarding to those
identified as malnourished children, 64.2% of them were registered in a feeding
program, and 35.8 % was not registered in a feeding program. From those
registered on a feeding program, 67.6% were referred by community outreach
workers / volunteers, 20.6% self-referral and 11.8% refereed after information
got from anther mothers that their children registered in a feeding program.
For the reason behind not registered in
the program for those found to be
malnourished, 68.4% were thought their
children were not malnourished or no one identified as malnourished, 21.1 % said center was far
from their houses and 10.5% said stay long time in the program.
Data for community outreach workers
/ volunteers interviewed Table (8) results shows that (72.6%) of the community
outreach workers / volunteers were female and 27.4 were male. One third of the community
outreach workers / volunteers, 35.5% in the present study were at age group of
34-41years, 27.4% at age group of 26 – 33 years, and a reasonable % 12.9% were
at the age over 50 years. Regarding family size, 62.9% of the community
outreach workers / volunteers had a family size around 6-8 persons, and 29% had
3-5 persons and only 8.1% were more than 9 persons. As for the presence of
children under 5, 58.1% of volunteers did not have children under 5 years and
only 3.2% of them had 2 children under five years. The education level of the volunteers community
outreach workers / volunteers was reported as 37.1% were illiterate, 30.6% had
a primary level of education, 22.6% had educated through Khalwa and only 6.5%
and 3.2% had a secondary level of education and university respectively.
Table (9) reveals that 53.2% worked
as community outreach workers / volunteer between 3-5 years and 21% worked as
community outreach workers / volunteer more than 5 years. Regarding working
days per week, 53.2% were working 2 days per week and 30.6% of the community
outreach workers / volunteer worked 3 days per week. For the community outreach
workers / volunteer worked in the same
community,100% of them knew each other .The result demonstrates that 90.3% of
the community outreach workers / volunteer
had a specific area to be covered
.
Table (10) showed that the
community outreach workers / volunteers 87.1% was trained on basic CMAM
training and almost all 98.4% were receiving
Food for Work as an incentive.
Table (11) reveals that, 90.3% of
the community outreach workers / volunteers knew well their role inside the
community and only 9.7% did not know their role, 100% of community outreach workers /
volunteers had used MUAC measurement to identify malnourished children and
12.9% beside the MUAC also had used bilateral edema for checking malnutrition.
From the total interviewed community outreach workers / volunteers 90.3% had
demonstrated the correct way of measuring MUAC.
In table (12) the issue of mothers
refusal was reflected, 88.7% of the mothers were referred to the centers /
nutrition program without any objection, where some (11.3%) cases refused to
refer, from them refused cases, 14.3% were not convinced and 85.7% of them
convinced by the medicals assistance and key person from family.
Table (13) shows that, only 79% of
the community outreach worker / volunteers did their work based on their role
at the CMAM guideline, 91.9% of the community outreach worker / volunteers had
good linkage with the feeding program and 85.5% of the community outreach
worker / volunteers reported the cases identified as malnourished to the staff
at the center. Of the community outreach worker / volunteers 79% discussed
their monthly achieved activities with the nutrition program staff and 21%
demonstrated that they did not discuss their monthly achievement and report.
Table (14) regarding to the
difficulties that faced the community outreach workers / volunteers and any
issue support voluntary work, 53.2% of
the community outreach workers / volunteers reported that, did not face
difficulties, 24.2% of them reported that the community did not understand the
criteria of admission of feeding program, 16.1% mentioned that no cash payment
and 4.8% stated that, there was shortage of supply of RUTF/RUSF and super
cereal plus in the centers. For the issues support the voluntary work, 56.5% of
the community outreach workers / volunteers mentioned that they were happy and
30.6 % had requested to have full time salary or being an employment.
Discussion
This study was conducted to
investigate the effectiveness of the community outreach workers/ volunteers on
increase in the coverage of community based management of acute malnutrition
program in Rural Kassala locality, Kassala state, Sudan. The study covered 21
communities with feeding centers. Data was collected from the community
outreach workers/ volunteers total of 62, with an average of 3 volunteers for
each center. A total of 200 households were sampled for the community data. The
result showed that, a total of 1091 people living in these households, at an
average family size of 5.5 persons, this corresponding to the Sudan MICS (2014)
the average of household size were found to be 5.9 persons. The nutritional
status was identified for 309 children less than five years.
Regarding head of household (96.5%)
of the household headed by males since in Sudan generally and the rural areas
specifically men had authority to make
all of the decisions of the aspect of life,
that include not limited to the health, education and even the voluntary
work.
Concerning mothers / caregivers
education levels, education is one of the most important resources that enable
women to provide appropriate care for their children, which is an important
determinant of childrens growth and development. In the present study majority
of the sample was illiterate or participated in informal education, need
nutrition and health educator to support them in increase their awareness of
child care, improving their nutrition and health of the pregnant women and
their outcome, support on identification of their childs nutritional status,
beside spread the information about the feeding and health services at the
community.
The study reveals that, 99% of the
entire community knew the availability of the community outreach workers /
volunteers with the community. Volunteers are usually local and therefore
familiar with the area, its population and customs, and also well known by the
community members.
The results indicated that 75.2% of
the interviewed households were reached by the community outreach worker /
volunteers within last month and 73% of them were screened by MUAC, this is a
good indicator for the active case finding and early identification of
malnourished cases. This similar to the report conducted by Collins et al
(2007), who stated that in order to be able to provide the largest possible
proportion of the acutely malnourished population with access to care, a program
needs to be very effective at identifying people who need care andadmitting
them to the program. To reduce the barriers to access, screening must take
place in thecommunity using a simple, low cost method that is easy for
community-based volunteers to use and isaccepted as fair and transparent by the
population.
The coverage of feeding program was
calculated using the point coverage estimate and the result showed how well the
program was doing at the time of the study. A point coverage calculation used
the formula as follows: the cases identify as malnourished and found to be
attending SFP or OTP divided by the total cases identified as malnourished
times 100, the coverage of the program estimated by 64.2%.This stipulates
therapeutic feeding programs coverage standards of 50% for rural populations,
75% of urban populations and 90% of the camp populations as a key indicator of
programperformance (SPHERE, 2004). Regarding the effectiveness of the
identification of cases and referring them to the nutritional feeding program,
the result showed that 67.7% of the cases attending the feeding program were
referred by the community outreach worker/volunteers. In line with, Collins et
al (2007) state that, using techniques of community mobilization to engage the affected
population and maximize coverage and compliance. Wherever possible, programs
build on local capacity and existing structures and systems, helping to equip
communities to deal with future periods of vulnerability.
The majority of the volunteers were
females, this is referred to the concept of the Eastern Sudan culture and
traditions, for easily enters to the household for case finding, passing the
nutrition and health information to the mothers and caregivers. The result
showed that 58.1% of the community outreach workers / volunteers did not have
children, which allowed them to work with the community.All the volunteers used
MUAC for case identification;MUAC is a more sensitive indicator of mortality
risk associated withmalnutrition than weight for height. It is therefore a
better measure for the identification of children most in need of treatment,
9.7% of the community outreach workers / volunteers had taken MUAC measurement
wrongly which needs more training(Unicef,21014)..As state by Maleta. and Amadi, (2014) traditionally,
therapeutic feeding programs use weight-for-height percentage of median (WHM)
and/orthe presence of bilateral pitting oedema as admission criteria whilst at
the same time screening in thecommunity using Mid Upper Arm Circumference
(MUAC). The community outreach workers / volunteers 78%knew their roles in the
community. As state in Sudan CMAM manual, community outreach is essential to
make sure that undernourished children are detected early and referred for
treatment, raises awareness of the aims of services and builds support.
Moreover, it strengthens the communitys awareness of causes, signs and
treatment of SAM, and promotes health and nutrition behavior change.
On the questions of challenge and
the issue faced their volunteers work, 30% asked for a salary and 24% mentioned
that the community is confused about the admission criteria for each program.
Puett, and Guerrero, (2014).stated there are two major challenges facing
volunteer-based case finding systems. These are choosing volunteers who are
representative of their communities and secondly motivating volunteers to
perform their roles.
Concerning the linkage of
volunteers with the feeding program, 91.9% of the volunteers had good linkage
through reporting and discussing their monthly performance with the nutrition
staff at the main feeding center. In general, this indicates the good
relationship between the main feeding centers and volunteers, which emphasizes
the regular detecting of malnourished
cases, besides the updating of the situation of the entire community.
Conclusions
-
The community
outreach workers / volunteers found to 72.6% were female, from them 35.5% at
age group of 34-41years.
-
The entire
community knew the availability of the community outreach workers / volunteers
within the community.
-
Active case
finding and early identification of malnourished cases 75.2% of the households
were reached by the community outreach worker / volunteers within last month
and 73% of them were screened by MUAC.
-
The coverage of
the program estimated to be 64.2%, which is above the Sphere minimum standards
of 50% (for rural programs).
-
A good
relationship between the main feeding centers and volunteers, which emphasizes
the regular detecting of malnourished
cases, besides the updating of the situation of the entire community.
Recommendation
-
This study was
done in one locality in Rural Kassala locality, so the findings may not
represent other localities implementing same feeding program. Similar study
being recommended to be conducted targeting all localities.
-
Strengthen the
role of community outreach /volunteers at the community level, through
training, follow up and motivation.
-
On Job training,
to ensure the properly taking of the measurement of MUAC.
References
1. Black RE,
Victora CG, Walker SP, Bhutta ZA, Christian P, et al. Maternal and Child
Nutrition 1, Maternal and child under nutrition and overweight in low-income
and middle-income countries (2013) Lancet 382: 427-451.
https://doi.org/10.1016/S0140-6736(13)60937-X
2. Mahan LK
and Escott-Stump S. Krauses Food and
Nutrition therapy, edition 12th, Publisher Saunders Elsevier, London UK.
3. Collins
S, Dent N, Binns P, Bahwere P, Sadler K et al. Management of severe acute
malnutrition (2007) Lancet 368: 1992-2000.
https://doi.org/10.1016/S0140-6736(06)69443-9
4. Kouam CE.
Delisle H, Ebbing HJ, Israel AD, Salpéteur C, et al. Perspectives for
integration into the local health system of community-based management of acute
malnutrition in children under 5 years: A qualitative study in Bangladesh
(2014) Nutr J 13: 22. https://doi.org/10.1186/1475-2891-13-22
5. Food and
Nutrition Technical Assistance II Project (FANTA-2) (2011).
6. Federal
Ministry of Health of Sudan. Report of a Multi Indicator Cluster d (MICS)
(2014) Survey in Sudan, Sudan
7. Maleta K
and Amadi B. Community-based management of acute malnutrition (CMAM) in
sub-Saharan Africa: Case studies from Ghana, Malawi, and Zambia (2014) Food
Nutrition Bulletin 35: 2. https://doi.org/10.1177/15648265140352S105





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}