38-year-old male
present to the office with infertility and glucose permission, so for workup
was negative on clinical examination found to have loss of right testicular
sensation. Repeat blood work showed decreased FSH decreased TSH and decrease
testosterone levels and I proceeded with obtaining testicular ultrasound that
showed 2 discrete solid masses within the parenchyma of the right testicle both
of which demonstrate internal blood flow. The larger lesion appears to contain
calcification. The findings are most consistent with multifocal right
testicular neoplasm. The left testicle is normal. He underwent radical inguinal
orchidectomy and pathology showed stage IA T1 a seminoma the right testis after
orchidectomy patients hormone level normalized and sperm count improved.
Case
Report
38 years old male without any
medical problems presented to the office first time for routine medical
checkup. During history and examination, he told me he is having infertility
for last 2 years all the workup has been negative except low sperm count.
On my clinical examination his
right testicular sensation was missing and he never had any testicular
ultrasound. There were no signs of any gynecomastia, loss of axillary or pubic
hair. I decided to do the workup including ultrasound testes and hormone panel and
that showed decreased FSH decrease LH and testosterone level surprisingly was
normal 6 months before. Ultrasound testes he showed right testicular neoplasm
patient was sent to urologist for further management he had a right inguinal
orchiectomy done. Patient had a CT scan of chest abdomen and pelvis no evidence
of any med stasis. After 3 months of surgery patients testosterone level
improved and other hormone level normalized and sperm count improved.
Component
The right testicle measures 3.3 x
1.6 x 2.1 cm. There are 2 discrete intraparenchymal right testicular masses
identified. The largest is seen at the inferior medial aspect of the testicle,
measuring 1.4 x 1.0 x 1.3 cm, solid and with marked vascularity. There are
prominent hyperechoic foci seen at the periphery of the lesion, most likely
calcification. Within the posterior mid aspect of the testicle, there is an
additional hypoechoic solid lesion that also contains internal vascularity, measuring
0.9 x 0.7 x 0.9 cm. The findings are most consistent with a multifocal right
testicular neoplasm. There is mild degree right testicular microlithiasis. The
right epididymal head appears within normal limits.
The left testicle measures 3.7 x
1.7 x 2.2 cm, unremarkable.
CT pelvis: There is a moderate
amount of fecal material seen within the rectosigmoid colon. The prostate gland
appears unremarkable. The urinary bladder is unremarkable. There are normal
size inguinal lymph nodes. There is no discrete adenopathy seen. There is no
ascites. The appendix appears unremarkable.
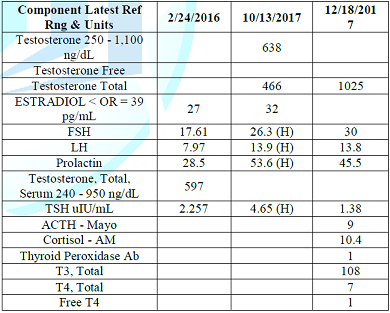
Table: Lab test and imaging studies.
Impression
1. There is no adenopathy seen.
2. There is a moderate amount of
fecal maternal seen in the rectosigmoid colon.
Discussion
Testicular cancer is the most
common solid malignancy affecting males between the ages of 15 and 35, although
it accounts for only 1 percent of all cancers in men [1]. Germ cell tumors
(GCTs) account for 95 percent of testicular cancers . They may consist of one
predominant histologic pattern or represent a mix of multiple histologic types.
For treatment purposes, two broad categories of testis tumors are recognized:
pure seminoma (no nonseminomatous elements present) and all others, which
together are termed nonseminomatous germ cell tumors (NSGCTs). In most series,
the ratio of seminoma to NSGCT is approximately one.
Testicular cancer has become one
of the most curable of solid neoplasms because of remarkable treatment advances
beginning in the late 1970s. Prior to that time, testicular cancer accounted for
11 percent of all cancer deaths in men between the ages of 25 and 34, and the
five-year survival rate was 64 percent [2]. In 2017, approximately 400 deaths
from testicular cancer are expected in the United States, with a five-year
survival rate of over 95 percent [1].
Testicular tumors usually present
as a nodule or painless swelling of one testicle, which may be noted
incidentally by the patient or by his sexual partner [3].
Occasionally, a man with a
previously small atrophic testis will note enlargement. Approximately 30 to 40
percent of patients complain of a dull ache or heavy sensation in the lower
abdomen, perianal area, or scrotum, while acute pain is the presenting symptom
in 10 percent.
In any man with a solid, firm mass
within the testis, testicular cancer must be the considered diagnosis until
proven otherwise. Prompt diagnosis and treatment of testicular cancer provides
the best opportunity for cure. Nevertheless, both patient and clinician factors
often contribute to a delay in diagnosis.
The widespread use of scrotal
ultrasound in the evaluation of male infertility occasionally leads to the
diagnosis of an incidental nonpalpable testicular mass [4,5].
Conclusion
In male infertility, physical
examination is key and ultrasound of testes should be a routine part of workup.
References
1.
Siegel RL, Miller KD and Jemal A.
Cancer statistics, 2018 (2018) CA Cancer J Clin 68: 7. https://doi.org/10.3322/caac.21442
2.
Einhorn LH. Treatment of
testicular cancer: a new and improved model (1990) J Clin Oncol 8: 1777. https://doi.org/10.1200/JCO.1990.8.11.1777
3.
Bosl GJ and Motzer RJ. Testicular
germ-cell cancer (1997) N Engl J Med 337: 242. https://doi.org/10.1056/NEJM199707243370406
4.
Toren PJ, Roberts M, Lecker I, Grober
ED, Jarvi K, et al. Small incidentally discovered testicular masses in
infertile men--is active surveillance the new standard of care? (2010) J Urol
183: 1373. https://doi.org/10.1016/j.juro.2009.12.012
5.
Eifler JB Jr, King P and Schlegel
PN. Incidental testicular lesions found during infertility evaluation are
usually benign and may be managed conservatively (2008) J Urol 180: 261. https://doi.org/10.1016/j.juro.2008.03.021
*Corresponding author:
Manoj
Singla, Reading Hospital and Medical Center, Pennsylvania, USA
Citation:
Singla
M. Unique 38 Years Old Male Presenting with Male Infertility Found to Have
Seminoma Testes: A Rare Case Report (2018) Edelweiss Appli Sci Tech 2: 234-235
Male infertility, Testicular tumor, Seminoma



