

Explore journal overview, editorial leadership, indexing, articles in press, latest published work, and highlights from previous issues.
Research Article :
A Diagnostic Ultrasound Report (DUR) is a leading method of communication from the radiographer to the clinician in order to provide feedback on the requested ultrasound examination/s.1 This feedback is important in the provision of quality healthcare delivery. Therefore, any inadequacies in the communication between the clinicians and the radiographers on DUR can compromise the clinicians diagnosis, and may as well lead to wastage of resources in the radiological department.
The growth in the use of ultrasound as a diagnostic imaging tool has led to the high demand for a workforce with appropriate competencies to perform and interpret diagnostic ultrasound imaging. According to Makanjee et al, diagnostic ultrasound imaging is a dominant first-line investigation for a variety of abdominal symptoms because of its applicability and comparative accessibility in most healthcare institutions.2 Diagnostic ultrasound imaging success in terms of diagnosis, however, depends upon numerous factors, the most important of which is the competency of the operating practitioner. Other factors include the status of equipment and the body stature of the patient.
Diagnostic ultrasound imaging is considered to be safe, effective, and highly adaptable to varied clinical needs and settings. This diagnostic imaging modality is capable of providing clinically relevant information about most internal parts of the body cost-effectively. Obtaining maximum clinical benefit from diagnostic ultrasound, as well as ensuring the optimal utilization of healthcare resources, requires a combination of appropriate ultrasound diagnostic equipment and competencies in the performance and interpretation of the ultrasound examinations.4
Diagnostic reporting is inseparable from sonographic imaging, as a means of communication from the radiographers to the referring clinicians.
Clinicians generally do not have direct contact with radiographers to discuss and clarify ultra-sonographic findings. Therefore radiographers are expected to provide clinicians with duly detailed diagnostic ultrasound reports as feedback to the clinicians clinical question/s.
Based on anecdotal information, the returned DURs as feedback from clinicians to the radiographer in relation to the inadequacies of DURs, clinicians especially from Internal medicine, general surgery, pediatrics, obstetrics and gynaecology raise concerns over the quality of the DURs or radiographers competencies.6 The radiographers equally try to shift the blame to the inadequacies in the radiological requests from the clinicians. The clinicians concerns are sometimes viewed as in conflict with the scope of ultrasonography. Yet the overall inadequacies could result into clinicians receiving questionable results, which in turn would negatively affect conclusive decisions on the management of patients.6,7, 8 As a result, clinicians have excessively gone for second opinions. Such approach contributed to delays and increased cost in the patients clinical management.
Studies have been conducted and documented in different countries such as the United Kingdom, India, Uganda and Ghana, assessing clinical communication between clinicians and radiographers and effect on the quality of diagnostic ultrasound reports.5, 9, 10 There has been no known documented study in Zambia or neighboring countries in this regard. It is envisaged that this study would provide useful information for promoting the quality of Diagnostic Ultrasound Imaging and Reporting by radiographers in Zambia and other comparable healthcare settings.
A cross-sectional descriptive study design was used in the study. The study was conducted at the University Teaching Hospital in Lusaka, which is the highest referral hospital in Zambia. Collectively 30 clinicians from the departments of Internal Medicine, General Surgery, Pediatrics, Obstetrics and Gynecology were conveniently sampled; and 12 radiographers who carry out sonographic examinations in the UTH Radiology Department were purposively recruited into the study.
Convenience sampling methods were used to select the study participants. Using EPI Info 7, from a collective total of 150 clinicians serving the Departments of Internal Medicine, General Surgery, Paediatrics, Obstetrics and Gynaecology, a sample size of 40 clinicians was generated. A self-administered, semi-structured, questionnaire was administered to each of the clinicians recruited in the study. All the 12 radiographers practicing ultrasonography in the UTH Radiology Department were included in the study. Each of these radiographers was as well given a semi-structured questionnaire specifically suited to them for self-administration, in line with the themes in the clinicians questionnaires.
All the 40 clinicians included in the study had earlier requested for ultrasonography with DURs from the radiographers. Despite serving in the mentioned Departments, a clinician without history of requesting for a DUR was excluded from the study. The radiographers included in the study were on full-time employment and performed ultrasonography in the UTH Radiology Department. The student radiographers and qualified radiographers that did not perform sonographic examinations were not included in the study.
Statistical Package for Social Sciences (SPSS) Version 22 software was used in data analysis. Microsoft Excel 2007 was used to generate figures and tables. Ethical clearance was obtained from the Lusaka Apex Medical University Ethics Committee, and permission to proceed with the study was granted by the UTH Management. There were no foreseen risks or harm to the participants and UTH as an institution. Participation in the study was voluntary. The consent was obtained from the participants prior to issuing them with questionnaires by endorsing the consent form adjoining the information sheet.
A total of 52 questionnaires were administered to the study participants of which 40 were clinicians and 12 were radiographers, which entailed the distribution of participants between clinicians and radiographers: 40 of 52 (77%) and 12of 52 (23%) respectively. With regard to data realization, 30 (75%) duly completed questionnaires were obtained from the clinician-participants while 10 (83.3%) were obtained from the radiographers. This attainment represented collective realization of 77% response rate.
Socio-demographic Profiles of the Participants
The participants in this study belonged to two professional disciplines: clinicians and radiographers. The clinician-participants departmental affiliations were: 26.7% Obstetrics and Gynaecology, 26.7% Internal Medicine, 23.3% Surgery and 23.3% Paediatrics. The majority of the clinician-participants (77%) were males, while 23% were females. In terms of age, the majority (36.7%) of the clinician-participants were of 35- 44 years age group. The oldest (3.3%) clinician-participant was older than 55 years. With respect to professional qualifications, most clinician-participants (60%) held Masters degree as highest qualification in respective areas of specializations compatible with the affiliation departments (Table 1).
The radiographers constituted 10 of 40 (25%) realized participation, out of which 60% of them were males and 40% were females. Most (40%) of the radiographer-participants were older than 40 years, while the youngest age group (20-25 years old) constituted 20% as in Table 1.
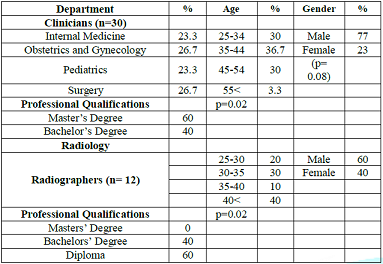
Table 1: Socio-demographic Profiles of the Participants
Work Experience and Competency of Clinicians and Radiographers at the UTH
The study showed that at least 30% of the clinician-participants at UTH had the longest work experience of at least 16 years. The shortest work experience among the clinicians was one to five years, and constituted 23.3% of the clinician-participants. The majority (60%) of the clinicians did not have formal qualifications in Diagnostic Ultrasound (DU) although 40% of the clinicians had history of short in-house training in DU. In-house training involved workshops (20%) and specific modular trainings (10%). Furthermore, some clinicians (6.7%) undertook short courses and others (3.3%) pursued diploma training in DU (Table 2).
The findings indicate that 40% of the radiographers had more than 5 years of work experience as ultrasonographers while the other (60%) radiographers had work experiences ranging from less than one year to five years. The study further showed that the majority (80%) of the radiographers practicing ultrasonography at the UTH had formal training in DU at diploma qualification (70%) with one (10%) holding Bachelors degree in Sonography. There were 20% of the radiographers who obtained competencies through in-house training (Table 2).
Use of DU Standard Operating Procedures by Clinicians and Radiographers
On the presence and use of Standard Operating Procedures (SOPs) between clinicians and radiographers, 47% of the clinicians stated that SOPs were never in existence in their Departments while 43% of the clinicians indicated that they had SOPs, whereas 10% of the clinicians indicated that they had never heard of these procedures during their years of practice. Out of the 43% clinicians with SOPs in their departments, the majority (69.2%) of them reported that they always requested DU examinations according to the SOPs, whereas 23.1% indicated that they occasionally followed SOPs in requesting for DU examinations. However, 7.7% of the clinician-participants indicated that they never followed the SOPs.
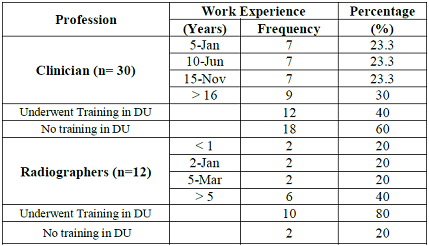
Table 2: Work Experience and Competencies of Clinicians and Radiographers.
There were 60% of the radiographer-participants indicating that they had SOPs for DU examinations, whereas 40% of the radiographers reported that they did not have the SOPs. Among the radiographers that indicated presence of the SOPs, 83% of them reported that the SOPs were not displayed in their ultrasound rooms, though 17% of the radiographers indicated that the SOPs were readily available in the operating rooms. Among 60% of the radiographers that indicated availability of SOPs, the majority (83.3%) indicated that they followed the SOPs of sonographic reporting, while 16.7% of the radiographers indicated that they never followed the SOPs of sonographic reporting. The latter reaffirmed that they did not follow the standard way of writing the reports, but used their own improvised formats of reporting.
Quality of Clinical and Diagnostic Information on the Generated Sonographic Requests and Report Forms
The study showed that clinicians were divided on the use of standard radiological forms or Sonographic Requests (SRs) when requesting for DU examinations with 50% indicating use of standardised or approved radiological forms. The other 50% of the clinicians indicated infrequent use of standardised radiological forms (Figure 2).
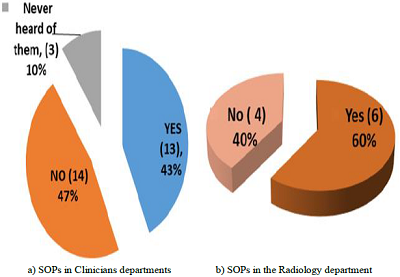
Figure 1: Standard Operating Procedure Presence and Use in the Departments.
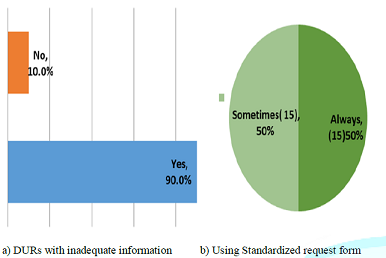
Figure 2: Sonographic Reports with Inadequate Information.
With respect to clinical information in the Sonographic Requests (SRs), 60% of the clinicians who indicated that they infrequently used standardised SRs, rarely included all clinical information on their requests for DU examinations, whereas the other 40% indicated that they included all the necessary clinical details in their requests. With regard to the quality of the Diagnostic Ultrasound Reports (DURs), 53% of the clinicians expressed satisfaction with the DURs by the radiographers.
Whereas 47% of the clinicians indicated that they were not satisfied. Most (80%) of the radiographers indicated that they did not always receive requisitions for DU examinations on the standardized request forms, while 10% of the radiographers indicated that they always received requests on standard forms. Another 10% of the radiographers expressed that they always received SRs on non-standard forms (Table 3).
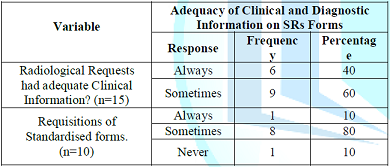
Table 3: Adequacy of Clinical and Diagnostic Information on SRs Forms.
On the adequacy of diagnostic information, 90% of the clinicians responded that they received DURs with inadequate information, whereas 10% of the clinicians revealed that they always received adequate diagnostic information from the radiographers DURs. It was further observed that the frequency by which the clinicians attested that they always received DURs with inadequate information was 59.3%, whereas 40.7% of the clinicians indicated that the DURs always had adequate information.
Communication between Clinicians and Radiographers All the radiographers (100%) had experiences of handling partially filled-in SRs from the clinicians. There were 40% of the radiographers that indicated that handling of partially filled-in SRs occurred most of the time, while 20% of the radiographers stated that they always received incomplete SRs from the clinicians (Table 4).
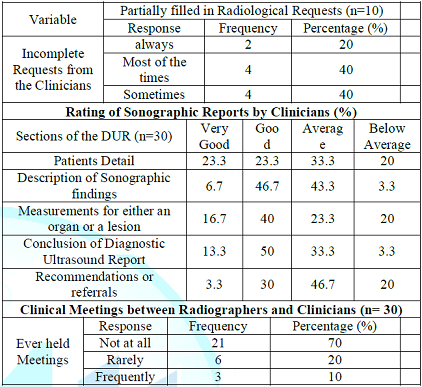
Table 4: Communication between Clinicians and Radiographers.
Most clinicians (33.3% and 46.7% respectively) rated the radiographers capabilities in handling the defined aspects of DURs as average with respect to patient details and recommendations or referrals. With regard to description of sonographic findings, structural measurements and conclusion of DURs, most clinicians (46.7%, 40%, and 50% respectively) rated the radiographers capabilities as good (Table 4).
Request for a Repeat or Second Opinion DURs
According to the findings in this study, 93% of the clinicians sought repeat or second opinion ultrasound DURs, which essentially included diagnostic ultrasound examination and only 7% of the clinicians reported that they never requested for repeat or second opinion DURs following the radiographers DURs. In terms of the frequency of the requests for repeat or second opinion DURs among the clinicians who sought this service, most (89.3%) of the clinicians indicated making such requests occasionally, whereas 7.1% indicated calling for repeat or second opinion DURs most of the times. With regard to predictability of calling for second opinion DURs, 3.6% expressed consistency in demanding this service.
Clinical Meetings between Radiographers and Clinicians
Most (70%) of the participants (clinicians and radiographers) indicated that they never held any clinical meetings in which subjects on or related to DURs were discussed. About 20% of the participants revealed that clinical meetings took place though rarely. However, 10% of the participants indicated that they regularly held meetings (Table 4). All (100%) of the participants were of the opinion that meetings on DURs were or could be of great importance for enhancing healthcare delivery.
This study assessed the adequacy of clinical communication between clinicians and radiographers on the quality of the Diagnostic Ultrasound Reports (DURs) at the University Teaching Hospital in Lusaka, Zambia. The focus of the study specifically covered subjects concerned with related work experience and competencies of clinicians and radiographers, application of Standard Operating Procedures (SOPs) in Diagnostic Ultrasonography (DU), quality of clinical and/or diagnostic information in DU process involving request for investigation and reporting of findings.
Socio-demographic Profiles of the Participants
The participants belonged to the professional disciplines of clinicians and radiographers respectively, at a University Teaching Hospital involved in provision of clinical services and teaching. The participants had different levels of training and experiences. Reference was made to fairly comparable studies done at public healthcare setting in South Africa and National Health Service (NHS) in the United Kingdom (UK).2,11
The interactional communication coherence in requests for a diagnostic imaging investigation, and the imaging process leading to diagnoses requires corroborative communication between physicians and radiology practitioners to optimise outcomes. The radiographers need not helplessly find themselves at a higher risk as in being blamed for poor quality of DURs. The approach to realize this goal could be translatable across varied global regions involving the physicians, radiologists, reporting radiographers and sonographers.11
Edwards et al (2014), in their research, what makes a good ultrasound report, point to the DURs as usually influenced by the quality of communication between the practitioners requesting for ultrasound investigations and those generating ultrasound reports.1
Work Experience of Clinicians and Radiographers at the UTH
This study showed that participants gender did not influence the adequacy of communication between clinicians and radiographers. Equally, gender orientation did not affect the quality of the DURs (p= 0.08). On the other hand, it was observed that qualifications and work experience of the participants in the study had a significant influence on the adequacy of communication and quality of the DURs generated at the UTH (p=0.02).
The findings in this study could be related to those by Booth and colleagues, in which they revealed that healthcare facilities where most clinicians and radiographers were highly qualified and with commendable number of years of effective practical experience, produced sonographic reports of good quality, which made it easier to reach valid diagnostic decisions.7, 12 However, in this study more clinicians (60%) had Masters Degrees in respective areas of specialization and none of the radiographers could have held competencies derived from such qualifications. Adequacy in communication between the two professional dimensions at varied levels of competency could be attributable to quality of communication affecting the quality of DURs, diagnoses and timely management of patients needs or treatment of diseases.
More specifically, despite the radiographers not possessing Masters Degrees, the majority (80%) of them underwent specialised training in Diagnostic Ultrasound whilst (40%) of the clinicians lesser versions of training, such as short orientation courses in diagnostic ultrasound. In the midst of statistical evidence pointing to qualifications as affecting the adequacy and quality of DURs generation, Diagnostic Ultrasound training gave most of the radiographers an increased advantage over the clinicians in ultrasonography just as the clinicians had increased advantage in respective areas of specializations. This consideration requires recognition and appreciating indispensible need for intra-professional and inter-professional team work dynamics for optimal healthcare delivery, backed by continuing professional developments that enhanced essential competencies.13
Use of DU Standard Operating Procedures by Clinicians and Radiographers
The research findings showed that the clinicians were divided between the use of the standard radiological forms and non-standard medium of requesting for diagnostic ultrasound examinations with 50% indicating that they always used the standard forms. The other 50% indicated that they only used the standard forms at times and mainly used plain papers, consultation forms, or laboratory request forms for making sonographic requests (SRs)
Clinicians who had used alternative forms attributed cause to non-availability of the standard radiological forms. Such unconventional modes of communication proved as inefficient as clinicians were not adequately filling in the required information for the radiographers to carry out sonographic ultrasound examination. On the other hand, 60% of the radiographers indicated that they had SOPs in their departments. The majority (83.3 %) amongst radiographers attested to following the standard way of reporting as opposed to 16.7% that indicated that they used improvised ways of writing sonographic reports.
Based on comparable findings, as cited above, Bosmas and colleagues highlighted areas of improvements in the quality of sonographic reports.8 These authors pointed out Standard Operating Procedures to be strictly followed by the practitioners in issuing a diagnostic imaging requests DU and DURs. The use of unconventional request forms increases the chances of important information being missed from the request forms, which could be undesirable recipe for substandard DURs.14 The use of unconventional forms greatly hampers the adequacy of communication between clinicians and radiographers.6, 15
A clear message in the communication of requests is very important so as for the receiver to comprehend the request and be able to give appropriate feedback message. This process also matches the communication process where the clinicians clinical questions brought before the intended radiographers led to factual evidence-based answer as feedback in form of clear DUR.17, 18
With respect to the above pointed out channel of communication, Most (80%) of the radiographers indicated that they did not always receive requisitions for DU examinations on the standardized request forms, implying that the radiographers feedback encountered communication barriers to quality DUR. About 47% of the clinicians expressed dissatisfaction with the quality of DURs generated by the radiographers. Due to this dissatisfaction, radiographers reported that the majority (93%) of the clinicians dissatisfied with available DUR consistently requested for repeated or second opinion DURs.
Antwi and his colleagues in their study of assessing the effectiveness of multicultural communication between radiographers and patients and its impact on outcome of examinations, reveal that communication becomes effective if regular meetings among the practitioners are incorporated at every level of structured organization. This study shows that most (70%) of the participants had no clinical meetings in which DURs or related subject was discussed. Such a finding calls for interactional platforms where the clinicians and radiographers discuss the desirable improvements in communication linked to quality of DURs. With such interactional forum missing or presumed missing, the DURs quality is highly compromised as status quo and areas of improvement could be fragmented and without consensus.
It is hereby reaffirmed that the communication between clinicians and radiographers at UTH was inadequate. This could have been attributed to clinicians not providing adequate clinical information on the request forms, coupled with non-usage of standard radiological forms. In comparative terms, the inadequacy could equally be premised in the DURs. Inadequate clinical meetings between clinicians and radiographers influenced clinical communication between these two healthcare practitioners at the UTH. In this regard, the quality of the DURs generated by the radiographers at UTH required methodical approaches to improvement and minimize widespread sonographic repeated requests for DU and DURs.
The study showed that clinical communication between clinicians and radiographers was cardinal in expediting detection of diseases and subsequent healthcare and/or treatment. Such communications also implored provision of appropriate and adequate clinical communication tools and procedures.
Based on this study identification of approved DU competencies and practitioners by formal training in ultrasound at degree, postgraduate certificate, or postgraduate diploma could be recommended. The Continuing Professional Development (CPD) programmes involving short courses in needy areas should be part of sonographic practice norms. Clinicians could also undergo short courses in fundamentals of ultrasonography to enhance intra-professional and inter-professional healthcare delivery. There should be consistent platforms for joint clinical meeting where the clinicians and radiographers discuss sonographic SOPs, SRs and DURs as part of scheduled clinical meetings.
The authors would like to acknowledge support offered to them by the University Teaching Hospital Management, the Management of the Evelyn Hone College and Management of the Lusaka Apex Medical University.
1. Edwards H, Smith J and Weston M. What makes a good ultrasound report? Ultrasound. (2014) 57-60.
2. Makanjee CR, Bergh A and Hoffmann WA. Healthcare Provider and Patient Perspectives on Diagnostic Imaging Investigations (2015) African J Primary Health Care Family Medicine 15: 1-7. https://dx.doi.org/10.4102%2Fphcfm.v7i1.801
3. Giroldi E, Veldhuizen W and Mannaerts A. Doctor, Please Tell me its Nothing Serious: An Exploration of Patients Worrying and Reassuring Cognitions Using Simulated Recall Interviews (2014) BMC Family Practice 15: 73-60. https://doi.org/10.1186/1471-2296-15-73
4. Pallan M, Linnane J and Ramaiah S. Evaluation of an independent, radiographer-led community diagnostic ultrasound service provided to general practitioners (2013) J Public Health 2: 176-181. https://doi.org/10.1093/pubmed/fdi006
5. Antwi WK, Kyei KA and Quarcoopome, LNA. Effectiveness of Multicultural Communication between Radiographers and Patients and Its Impact on Outcome of Examinations (2014) World J Medical Res 6: 12-18.
6. Field LJ and Snaith BA. Developing radiographer roles in the context of advanced and consultant practice (2013) J Medical Radiation Sciences 6: 11-15. https://dx.doi.org/10.1002%2Fjmrs.2
7. Booth L. The radiographer-patient relationship: Enhancing understanding using a transactional analysis approach (2018) Int J Diagnostic Imaging Radiation Therapy 4: 323-331. https://doi.org/10.1016/j.radi.2007.07.002
8. Bosmans JML, Weyler JJ, De Schepper AM and Parizel PM. The Radiology Report as Seen by Radiologists and Clinicians (2011) J Radiology 259: 184-195. https://doi.org/10.1148/radiol.10101045
9. Larson DB, Froehle CM, Johnson ND and Towbin TJ. Communication in Diagnostic Radiology: Meeting the Challenges of Complexity (2014) Ame J Radiology 203: 957-964. https://doi.org/10.2214/AJR.14.12949
10. Danton G. Radiology reporting: Changes worth making are never easy (2010) Appl Radiology 39: 19-23.
11. Grieve F, Plumb A and Khan S. Radiology reporting: a general practitioners perspective (2010) British J Radiol 83: 17-22. https://doi.org/10.1259/bjr/16360063
12. Lockhart ME, Robbin ML, Berland LL, Smith JK, Canon CL, et al. The sonographer practitioner: One piece to the radiologist shortage puzzle (2017) J Ultrasound Med 22: 861-864. http://dx.doi.org/10.7863/jum.2003.22.9.861
13. Eddy A. Work-based learning and role extension: A match made in heaven? (2010) Radiography 16: 95-100. https://doi.org/10.1016/j.radi.2009.12.001
14. European Society of Radiology. Good practice for radiological reporting. Guidelines from the European Society of Radiology (ESR) (2010) Insights Imaging 2: 93-6.
15. Kasper J, Légaré F, Scheibler F and Geiger F. Turning signals into meanings-shared decision making meets communication theory (2011) Health Expect 1: 3-11. https://doi.org/10.1111/j.1369-7625.2011.00657.x
16. Leigh J. A tale of the unexpected: Managing an insider dilemma by adopting the role of outsider in another setting (2014) Quality Research 4: 428-441. https://doi.org/10.1177%2F1468794113481794
17. Robert L, Cohen M and Jennings G.A new method of evaluating the quality of radiology reports (2016) Academic Radiology 13: 241-248. https://doi.org/10.1016/j.acra.2005.10.015
18. Bernard A, Whitaker M and Ray M. Impact of language barrier on acute care medical professional is dependent upon role (2006) J Professional Nursing 6: 355-358. https://doi.org/10.1016/j.profnurs.2006.09.001