

Research Article :
Al-Aghbari Khaled*, Bamashmoos
Mohammed and Askar Faiza Objectives: The aim of the study is to Determine, prevalence,
possible risk factors, aetiology and outcome of patient with atrial
fibrillation admitted into medical and cardiac units at Kuwait University
hospital during 2014-2017. Methods and patients: Cross sectional retrospective review of all files of
patients admitted to hospital during 2014 t0 2017. We reviewed 2030 Cardiac
cases among which 179 were atrial fibrillation. Special form was designed to
record general characters, risk factors & out come during hospitalization. Results: The prevalence of atrial fibrillation (A F) was 8% (179/2030).
The male to female ratio was 5:4 and their main age was 54±9. The common risk
factors were ischemic heart disease, Qat chewer, hyperlipidemia, rheumatic
heart disease and smoker represented to (46%,41%, 39%, 38%,38%) respectively.
Transthoracic echo was performed for all patients and revealed that 92 (51.9%)
had systolic dysfunction, while only 34(18.9%) patient had diastolic
dysfunction. Mitral stenosis was detected in 30 (16.7%) patients among
rheumatic heart disease (RHD). Regarding outcome of AF we found that 137(77%)
was improved and discharged, while 42 (13.4%) was expired, however, 18 patients
(10%) was referred to other hospitals. The prevalence of AF
in this study was higher than that reported from other countries, and occurred
in younger age group. Ischemic heart disease and RHD were prominent risk
factors for AF in this study. Atrial Fibrillation (AF) is the
most common cardiac arrhythmia affecting over 2 million patients in United states
of America alone [1]. Much of the morbidity associated with AF is attributed to
a 5 to 6 fold increase in the risk of stroke [1] .Pooled data from studies of
chronic AF in North America, the United Kingdom & Iceland reported a prevalence
of 0.5-1%. In the general population AF is associated with risk factors of
cardiovascular disease including, Ischemic Heart Disease (IHD), Rheumatic Heart
Disease (RHD), Hypertension & Dilated, Hypertrophic, Restrictive &
congenital cardiomyopathy and other related diseases [2-6]. These risk factors
were reported from various part of the world [2-6]. However, to the best of our
knowledge there is no any study have been done yet in Yemen. The aim of this study was to
determine the prevalence of AF, common characteristics of the patients and
possible risk factors and hospital outcome among patients admitted into Kuwait
University Hospital in Sanaa city during 2014-2017. A retrospective cross sectional
study was carried out among patients with AF admitted into Kuwait University
hospital during January 2014 to Dec 2017, using the Guide line for the
management of patient with AF of the America College of cardiology, American heart
association & European Society of cardiology [3]. We reviewed all files of
the patients admitted to the medical and coronary unite during the period of
study. Special form was designed to document demographic data (age, sex, habit,
and patients characters) clinical examination, investigations like
Echocardiogram, chest x-ray & Lab data. Possible risk factors or causes of
AF included; IHD, RHD, Hypertension, diabetes mellitus, Chronic Obstructive
Pulmonary Disease (COPD), & Hyperlipidemia were sought for and recorded
from patients file. The outcome of the patient during hospitalization was
recorded and analyzed. We included all patients with AF in both sexes if their
age above 5 years, AF documented by ECG and echocardiogram. We excluded cases
that treated in the ER. But not admitted to the ward, Age below 5 years and
those discharged against medical advice. All data collected was entered into PC
and statistically analyzed using SPSS software. Chi square was used to detect
the differences between two groups and qualitative data was compared using Fishers
exact test. A probability level of <0.05 was considered statically
significant. During the period of study, the total number
of admission in medical wards were 5344 patients, of this 2030 were cardiac
cases admitted into cardiology unit which reflecting 32% of total admission . The
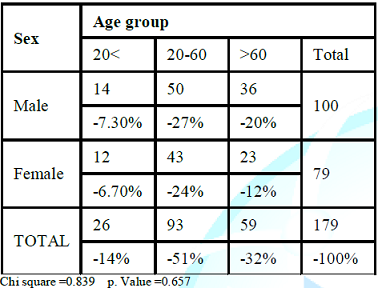
AF among cardiac patients was 179 given prevalence of (8%).The age group and
sex of patients is shown in the Table 1.
The main age of patients was 54 ±9. Year, 100 were males &79 were females
given male to females ratio 5:4. We divided the patients according to age into
3 groups (< 20years, 20 -60 years & >60 years). We found high
prevalence of AF in the age group (20 -60 years) in both sexes with no
significance differences between them (P value 0.657). Table 1: Age groups and sex distribution of patients with AF. There was high prevalence of
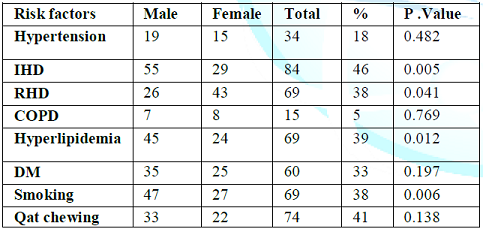
Ischemic Heart Disease (IHD), Qat chewer, Hyperlipidemia RHD, smoker and
diabetes mellitus represented (46%,41%,39% 38% 38%,&33%) respectively (Table 2). The prevalence of
hypertension (18) % and COPD (5%) were not common as other comorbid conditions
in these patients with (AF). Ischemic Heart Disease(IHD), smoking,
Hyperlipidemia and rheumatic heart disease were independent risk factors in AF
with P Value (0.005, 0.006, 0.012&0.041) respectively. Table 2: Distribution of risk factors in patients with Atrial fibrillation. Transthoracic Echo for those
patients with AF revealed 92 patients had systolic dysfunction & 34
patients had diastolic dysfunction. The most common lesion in RHD were Mitral
stenosis found in 30 patients, Mitral
incompetence in 11 patients ,while Aortic
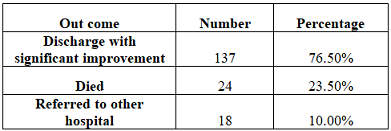
valve involved found only in 8 patients. The outcome of AF patients during
hospitalization was shown in Table 3.
137 (76.5%) patients discharge with significant improvement, 24(23.5%) patient
died & 18(10%) patients referred to other hospital for more advanced
management. Table 3: Outcome of AF patients during hospitalization. In this study the prevalence of
AF was (8%) higher than reported from Kuwait or Malaysia where they reported
prevalence of (4.24% &2.8 %) respectively [8,9]. Possible explanation of
this variation could be related to period of study, there study were limited to
few months while in our case we included all patient admitted throughout 5
years. Other possible explanation is high prevalence of RHD among our patients.
We found that AF was more prevalence in males (55%) than in females (45%) ,this
results are coincide with other studies from Gulf , they reported AF among,
male was 53% and female 48% nearly same results were reported from Germany
[10-12]. The result of this study demonstrated that the main age of our
patients admitted with AF is 54 years±9 younger than ages reported from other countries.
These may be related to effect of rheumatic fever and (RHD), which is more
prevalence in younger age and it leads to high morbidity and mortality in our
country. In patient with rheumatic heart disease we found the commonest valve
lesions is mitral stenosis. Previous study indicated that RHD is well known
cause for (AF) [14,19]. The most important risk factors
for AF in our study were (IHD) followed by Hyperlipidemia and (RHD). (IHD) play
significant role in atrial fibrillation, however, the (IHD) in our study was
higher than previous studies that reported from various countries [13-18]. (IHD)
in AF was ranged from (35%- 28%) in Gulf countries and that in Western countries
(7.8%-26 %). This high rate in our study may be related to lack of proper
follow up of IHD cases & there is no control Program for IHD risk factors. The
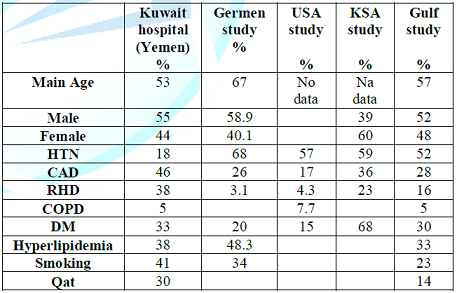
second significant risk factor for AF in our study was (RHD). Comparing our result
to studies from neighbors our results was (38%) higher than any reported before
which quoted prevalence of (4,3%-23%) [17-19] (Table 4). The possible explanation for our
high numbers is that rheumatic fever & RHD is still endemic in our country
especially in young age groups. Diabetes mellitus (DM) is well known risk for
Ischemic heart disease, it was found in 33% in patients with AF in our study,
in KSA it was found in 68% which is higher than the results of our study
because the prevalence of DM in Saudi Arabia is high in general population
(23%) and associated with obesity in (24%) [13]. Smoking is well known risk for
ischemic heart disease all over the world, in our study it is present in (38%) of
patients with AF, which is higher than that found in Germany (34%) & Gulf
study (23%) [14-19]. Qat Chewing in Yemeni people increase the desire for smoking,
Qat chewing itself may increases the
incidence of AF by its possible increase in heart rate & blood pressure [20,21].
Other risk factors such as (DM) did not have significant role in AF in our cases
which needs prospective study to clarify their roles. Of interest in this study
is the prevalence of AF in hypertension is low when compared to other studies
it present in 18%, other causes of AF like COPD and myocarditis are less in
proportion. 1. This
study was retrospective study we found difficulty on extracting the data from
files and information was not systematically organized. We strongly recommend
improving the recording system in our hospitals to become in a computerized
manner which will facilitate the future researches. 2. The
prevalence recorded by this research was underestimated because many cases are
Asymptomatic or treated as outpatient, so we recommend further more researches
in this field to help health providers in making the proper management plan for
example to strongly encourage the use of Long acting penicillin as a primary
prevention for rheumatic heart disease. The prevalence of AF among admitted
patients in our study almost higher than other countries and occurred at young
age RHD more frequent in our patients & represent the second possible precipitating
cause for AF after Ischemic heart disease Other possible risk factors such
as DM & Hypertension were less frequent in our cases. Qat chewing habit was
present in considerable number of patients which may increase the risk of
Hypertension & AF. It is suggested that further prospective study is needed 1. Feinberg
WM, Blackshear JL, Laupacis A, Kronmal R and Hart RG. The prevalence, age
distribution, and gender of patients with atrial fibrillation. Analysis and implications
(1995) Arch Intern Med 155: 469-473. doi:10.1001/archinte.1995.00430050045005 2. Wolf
PA, Dawber TR, Thomas HE Jr and Kannel WB. Epidemiologic assessment of chronic
atrial fibrillation and risk of stroke: The Framingham study (1978) Neurology
28: 973-977. DOI:
https://doi.org/10.1212/01.wnl.0000407150.80523.a4 3. Uster
V, Ryden LE, Asinger RW, CannomDS, Crijns HJ, et al. ACC/AHA ESC guidelines for
the management of patients with atrial fibrillation: Executive summary a report
of the American College of Cardiology/American Heart Association task force on
practice guidelines and the European Society of Cardiology Committee for
practice guidelines and policy conference (Committee to develop guidelines for
the management of patients with atrial fibrillation) developed in collaboration
with North American Society of Pacing and Electrophysiology (2001) Circulation
104: 2118- 2150. https://doi.org/10.1093/eurheartj/ehl176 4. Flagel
KM, Shipley MJ and Rose G. Risk of stroke in non-rheumatic atrial fibrillation
(1987) Lancet 1: 526-529. https://doi.org/10.1016/S0140-6736(87)90174-7 5. Vaidya
PN, Bhosley PN, Rao DB and Luisada AA. Tachyarrhythmias in old age (1976) J Am
Geriatr Soc 24: 412-414. 6. Ostrander
LD Jr, Brandt RL, Kjelsberg MO and Epstein FH. Electrocardiographic findings
among the adult population of a total natural community, Tecumseh, Michigan
(1965) Circulation 31: 888-898. https://doi.org/10.1161/01.CIR.31.6.888 7. Wolf
PA, Abbott RD and kannel WB. Atrial fibrillation as an independent risk factor
for strok: The Framingham study (1991) stroke 22: 983-986. http://dx.doi.org/10.1161/01.STR.22.8.983 8. Frost
L, Johnsen SP, Pedersen L, Husted S, Engholm G, et al. Seasonal variation in
hospital discharge diagnosis of atrial fibrillation: A population-based study
(2002) Epidemiology 13: 211-215. http://dx.doi.org/10.1097/00001648-200203000-00017 9. Freestone
B, Rajaratnam R, Hussain N and Lip GY. Admissions with atrial fibrillation in a
multiracial population in Kuala Lumpur, Malaysia (2003) Int J Cardiol 91: 233-238.
https://doi.org/10.1016/S0167-5273%2803%2900031-7 10. Wang
TJ, Massaro JM, Levy D, Vasan RS, et al. A risk score for predicting Stroke or
death in individuals with new onset with Atrial fibrillation in the community: the
Framingham Heart Study (2003) JAMA 290: 1049-1056. https://doi.org/10.1001/jama.290.8.1049 11. Fuster
V, Ryde’n LE, Asinger RW, Cannom DS, Crijns HJ, ACC/AHA/ESC guidelines for the
management of patients with atrial fibrillation: executive summary: a report of
the American College of Cardiology/American Heart Association Task Force on
Practice Guidelines and the European Society of Cardiology Committee for
Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for
the Management of Patients With Atrial Fibrillation) (2001) J Am Coll Cardiol 104:
2118-2150. https://doi.org/10.1161/circ.104.17.2118 12. Fuster
V, Ryde’n LE, Cannom DS, Crijns HJ, Curtis AB et al. ACC/AHA/ESC (2006) European
Heart Rhythm Association, Heart Ryhtem Society, USA. 13. Al-Nozha
MM, Al-maatouq MA, Al-Mazrou YY, Al-Harthi SS, Afrah MR, et al. Diabetes
mellitus in Saudi Arabia (2004) Saudi Med J 25: 1603-1610 14. Ali
WM, Zubaid M, AL Motarreb A, Singh R, Al-shereiqi SZ, et al. Association of
khat chewing with increased risk of stroke and death (2010) Mayo Clin Proc 85:
974-980. https://dx.doi.org/10.4065%2Fmcp.2010.0398 15. Fuster
V, Ryde’n LE, Cannom DS, Crijns HJ, Curtis AB, et al. ACC/AHA/ESC (2006) European
Heart Rhythm Association, Heart Ryhtem Society, USA. 16. Fuster
V, Rydén LE, Cannom DS, Crijns HJ, Curtis AB, et al. Guidelines for the
management of patients with Atrial fibrillation: A report of the American
College of cardiology/American Heart Association Task Force on practice Guidelines
and the European Society of cardiology Committee for practice Guidelines
(Writing Committee to Revise the 2001) (2006) Eur Heart J 27: 1979-2030.
https://doi.org/10.1161/CIRCULATIONAHA.106.177292 17. Fuster
V, Rydén LE, Cannom DS, Crijns HJ, Curtis AB, et al. Guidelines for the
management of patients with atrial fibrillation developed in Collaboration with
the European Heart Rhythm Association & the Heart Rhythm Society (2006) Circulation
114: 257-354. https://doi.org/10.1161/CIRCULATIONAHA.106.177292 18. Gage
BF, Waterman AD, Shannon W, Boechler M, Rich MW, et al. Validation of clinical
classification schemes for predicting stroke: Results from the National
Registry of Atrial fibrillation (2001) JAMA 285: 2864-2870. http://dx.doi.org/10.1016/S1062-1458(01)00458-5 19. J
Assim AlSuwaidi. Acute coronary syndrome and khat herpal (2011) Circulation
124: 2681-2689. https://doi.org/10.1161/CIRCULATIONAHA.111.039768 20. Ali
WM, Zubaid M, Al-Motarrieb A, Singh R, Al-shereiqi SZ, et al. Association of
khat chewing with increased risk of stroke and death in patient presenting with
acute coronary syndrome (2010) Mayo clinic pro 85: 974-980. https://doi.org/10.4065/mcp.2010.0398 Al-Aghbari Khaled, Associated professor of internal Medicine, Sanaa University, Yemen, Tel: 967711118376, E-mail: dr_khaled_alaghbari@yahoo.com Atrial fibrillation, Risk factors, Cardiac,
YemenThe Prevalence of Atrial Fibrillation Among Acute Medical Admission in Kuwait University Hospital in Sanaa City
Abstract
Full-Text
Introduction
Patients and
Methods
Results
Discussion
Limitations
Conclusion and
recommendations
References
*Corresponding author:
Citation
Keywords
