

Research Article :
Background: While various orthodontic appliances were designed
to manage the anteroposterior and vertical discrepancy, miniscrew was one of
the powerful appliances and was widely utilized as anchorage to treatment the
anteroposterior relationship. The
logical approach to the diagnosis and treatment of orthodontic cases is now
considered as a four dimensions issue which includes the diagnose, designing
and treatment for the anteroposterior discrepancy, vertical
discrepancy, and transverse discrepancy, as well as the consideration for time
which not only refers to the treatment time but also refers to the long term of
post-treatment stability. The anteroposterior, vertical and transverse
dimension issue and the time issue interacts with each other and play a vital
role on the outcome of the orthodontic treatment. Various
orthodontic appliances were designed to manage the anteroposterior and vertical
discrepancy, such as miniscrew, Forsus, lingual
orthodontic appliance, headgear and so on [1-6]. And the miniscrew is widely
utilized in orthodontic clinical practice as anchorage. Compared with the group
treated with conventional transpalatal arch combined with high-pull headgear and
interarch elastics, the maxillary first molars had less mesial movement in the
miniscrew group in the same treatment duration [7]. The minisrew is also a
powerful technique in vertical control. Miniscrews placed in the anterior and
posterior regions of maxilla efficiently treated Class Ⅱ
skeletal discrepancy with high angle and gummy smile in adult patient [8]. The
diagnosing, designing and treatment should carefully consider the
anteroposterior discrepancy, vertical discrepancy, and transverse
discrepancy rather than neglect any one of them. In this study, we showed that
the anteroposterior discrepancy of the patient was treated by the vertical
control. Diagnose The
20 year-old girl come to us for orthodontic treatment with the main complain of
protrusion of upper incisors and unacceptable
profile and smile. She reported that her medical history was nothing special.
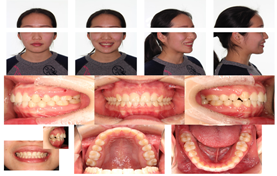
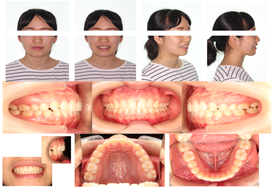
Class Ⅰ molars relationship and Class Ⅱ
canine relationship could be found in the pre-treatment photograph (Figure 1). The space in the upper
dentition was 3 mm, the overject was 7 mm and the overbite was 3 mm. The
protrude incisors could be found and she was shy to smile. The
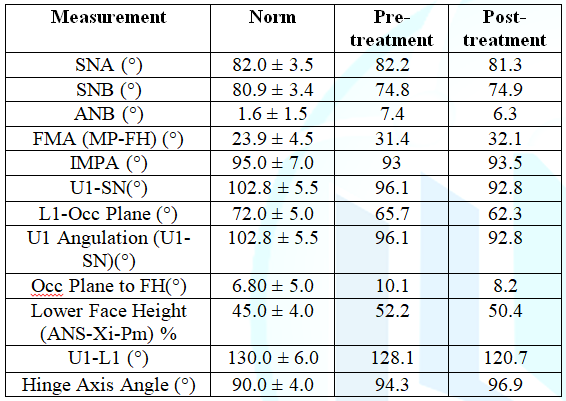
cephalometric
analysis
showed a severe skeletal Class Ⅱ relationship with mandibular hypoplasia (SNA
82.2, SNB 74.8, ANB 7.4) and protrude upper incisors (U1 angulation 96.1, U1-L1
128.1) (Table 1 and Figure 2). Figure 1: The
pre-treatment photograph. Table 1: The comparison
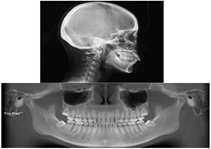
of pre-treatment and post-treatment cephalometirc analysis. Figure 2: The
pre-treatment radiation examination. The
objectives were as the following: 1) closed the space; 2) obtained Class Ⅰ molars
and canines realationship; 3) achieved the normal overbite and overject by
treating the anteropostereior discrepancy; 4) improved the profile; and 5)
obtained the esthetic smile. After
discussed with the patient, the nonextraction plan was performed.
After the alignment of the upper and lower dentition, the Spee curve was
obviously deep; on the other hand, the anteroposterior discrepancy was still
severe. After carefully analysis, we could find that the over development of
the posterior part of the alveolus was the root of the problem which caused the
clockwise rotation of the mandible and exhibited the symptom of overject. Two
miniscrew was placed in the zygomaticoalveolar, which offered
sufficient distant for the molar intrusion but did not interrupt the distally
movement of the upper dentition (Figure
3 and Figure 4). Figure 3: After 6 months
treatment. Figure 4: After 9 months
treatment, miniscrews were placed in the zygomaticoalveolar bimaxillarily. After
two years treatment, all the objectives were achieved. The space was close, the
anteroposterior discrepancy was corrected and the normal overject and overbite were obtained.
The normal Class Ⅰ molars and canines relationship were
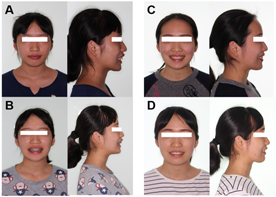
achieved. And the esthetic smile was improved (Figure 5 and Figure 6). Figure 5: Post-treatment photograph. The
radiation examination showed that the skeletal Class Ⅱ relationship was reduced
(ANB 6.3), the protrude upper incisors were degree (U1 angulation 92.8, U1-L1
120.7). And the occlusive plan was leveled (Occ
Plane 8.2). After 2 years following up, the result was still perfect. The long
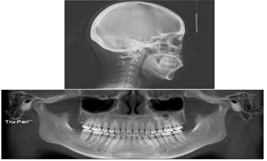
term post-treatment stability offered the self-confidence for the patient (Figure 7 and Figure 8). Figure 6: Post-treatment
radiation examination. Figure 7: Photographs of 2
years follow up. Finding
out the root of the problem is the vital logical issue in deal with the
anteroposterior, vertical and
transverse dimension
issue and the long term of post-treatment stability of orthodontic case, rather
than only focusing on the orthodontic appliances. For example, rotation effect
changes during treatment with Herb appliance were minimal in the growing
patients, and overall treatment was not associated with the significant forward
mandibular rotation [9]. Whats more, the mandibular posterior rotation will
induce a severe Class Ⅱ problem from a Class Ⅰ [10]. Anteroposterior positions of teeth variates among
different type of malocclusion, especially relating with the skeletal
relationship of different kinds of maxilla and mandible relationship. It
reported that in Class Ⅰ bimaxillary dentoalveolar protrusion
cases, the root apex of maxillary central incisor located a palatally and the
lateral teeth tipped mesially, compared with subjects with balanced profile and
normal occlusion [11]. The buccolingual inclination of mandibular second molars
is also related to the skeletal pattern of maxilla and mandible in cone-beam
computed tomography [12]. A positive correlation between anteroposterior
maxillomandibular relationship (Wits appraisal) and mandibular second molar
inclination could be found. In
this study the protrude incisors and over development of posterior alveolar was
the root problem and the mechanism of the anteroposteriorly skeletal discrepancy in the patient. The
intrusion of the upper molars with miniscrew allowed the anterior rotation of
the mandible by improving the leveling of the dentition and removing the block
of upper molar from the mandible. This vertical control not only dealt with
anteroposterior discrepancy and offered the patient an esthetic smile and
normal overject and overbite, but also improved the patients profile and smile
and offered a long term of post-treatment stability. The anteroposterior,
vertical, and transverse dimension and the time, especially the long term of
post-treatment stability, interacts with each other and must be carefully
considered during the diagnose, designation and treatment of orthodontic cases. 1.
The vertical control was vital for the anteroposterior treatment. 2.
The miniscrew was powerful in molar intrusion. 3.
The vertical, transverse and anteroposterior dimension issue and the long term
of post-treatment stability interacts with each other. This
research was supported by the National Natural Science Foundation of China
(31400808, 81570979 and 21402018), the Natural Science Foundation Project of
Chongqing (CSTS2015JCYJA10039), the Science and Technology Research Project of
Chongqing Municipal Education Commission of China (KJ1600226), and Program for
Innovation Team Building at Institutions of Higher Education in Chongqing in
2016 (CXTDG201602006). 1.
Yoon-Tarlie
C and Sadowsky G. Management of anteroposterior dental movements (2000) Sem
Ortho 6: 58-66. https://doi.org/10.1016/S1073-8746(00)80010-9 2.
Pisek
P, Manosudprasit M, Wangsrimongkol T, Keinprasit C and Wongpetch R. Treatment
of a severe Class II Division 1 malocclusion combined with surgical miniscrew
anchorage (2019) Am J Orthod Dentofacial Ortho 155: 572-583. https://doi.org/10.1016/j.ajodo.2017.09.023 3.
Michelogiannakis
D, Rossouw PE, Fishman LS and Feng C. A cephalometric comparison of treatment
effects and predictors of chin prominence in Class II Division 1 and 2
malocclusions with Forsus fatigue-resistant fixed functional appliance (2018) J
World Fed Ortho 7: 17-23. https://doi.org/10.1016/j.ejwf.2018.02.002 4.
Yanagita
T, Nakamura M, Kawanabe N and Yamashiro T. Class II malocclusion with complex
problems treated with a novel combination of lingual orthodontic appliances and
lingual arches (2014) Am J Orthod Dentofacial Orthop146: 98-107. https://doi.org/10.1016/j.ajodo.2013.08.022 5.
Wang
XD, Lei FF, Liu DW, Zhang JN, Liu WT, et al. Miniscrew-assisted customized
lingual appliances for predictable treatment of skeletal Class II malocclusion
with severe deep overbite and overjet (2017) Am J Orthod Dentofacial Orthop 152:
104-115. https://doi.org/10.1016/j.ajodo.2016.06.053 6.
Nucera
R, Militi A, Lo Giudice A, Longo V, Fastuca R, et al. Skeletal and Dental
Effectiveness of Treatment of Class II Malocclusion With Headgear: A Systematic
Review and Meta-analysis (2018) J Evid Based Dent Pract 18: 41-58. https://doi.org/10.1016/j.jebdp.2017.07.008 7.
Lee
J, Miyazawa K, Tabuchi M, Kawaguchi M, Shibata M, et al. Midpalatal miniscrews
and high-pull headgear for anteroposterior and vertical anchorage control:
Cephalometric comparisons of treatment changes (2013) Am J Orthod Dentofacial
Orthop 144: 238-250. https://doi.org/10.1016/j.ajodo.2013.03.020 8.
Wang
XD, Zhang JN, Liu DW, Lei FF, Liu WT, et al. Nonsurgical correction using
miniscrew-assisted vertical control of a severe high angle with mandibular
retrusion and gummy smile in an adult (2017) Am J Orthod Dentofacial Orthop 151:
978-988. https://doi.org/10.1016/j.ajodo.2016.04.034 9.
Deen
E and Woods MG. Rotational effects of Class II Division 1 treatment with the
Herbst appliance and fixed appliances in growing subjects with different
vertical patterns (2019) J World Fed Ortho 8: 18-23. https://doi.org/10.1016/j.ejwf.2019.01.003 10.
Echarri
P. Lingual Orthodontics: Patient Selection and Diagnostic Considerations (2006)
Sem Orthodontics 12: 160-166. https://doi.org/10.1053/j.sodo.2006.05.003 11.
Akiyama
S and Arai K. Antero-posterior positions of teeth in bimaxillary dentoalveolar
protrusion (2017) Ortho Waves 76: 46-54. https://doi.org/10.1016/j.odw.2016.11.003 12. Rakwong B, Petdachai S and Chuenchompoonut V.
Buccolingual inclination of the mandibular second molars with different anteroposterior skeletal patterns in cone-beam
computed tomography (2017) Ortho Waves 76:105-112. https://doi.org/10.1016/j.odw.2017.01.005 Xiaomian Wu, Chongqing Key Laboratory of Oral
Diseases and Biomedical Sciences, College of Stomatology, Chongqing, Medical
University, Chongqing, China, E-mail: wuxiaomian@hospital.cqmu.edu.cn,
wuxiaomian898@163.com
Hu X and WuX. Correcting the anteroposterior discrepancy of class Ⅱ patient with
overject by the vertical control of miniscrew (2019) Dental Res Manag 3: 28-31 Orthodontic
treatment, Orthodontic appliances, Protrude incisors, Anteroposterior
discrepancy.Correcting the Anteroposterior Discrepancy of Class Ⅱ Patient with Overject by the Vertical Control of Miniscrew
Xiaolei Hu and
Xiaomian Wu
Abstract
Method and Result: In the study we treated the severe Class Ⅱ skeletal
discrepancy subject with protrude upper incisors and mandibular hypoplasia by
the vertical control with the miniscrew. After two years treatment, all the
objectives were achieved. The skeletal Class Ⅱ discrepancy was improved (ANB
6.3), the protrude upper incisors were treated (U1 angulation 92.8, U1-L1
120.7) and the occlusive plan was leveled (Occ Plane 8.2). Class Ⅰ molars and
canines relationship were obtained.
Conclusion:
The vertical control was vital for the correction of anteroposterior
discrepancy. The anteroposterior, vertical and transverse dimension and the
time, especially the long term of post-treatment stability, interacts with each
other. Full-Text
Introduction
Method
and Results

Objectives
Treatment
Progress


Treatment
results
Discussion
Conclusion
Acknowledgments
References
*Corresponding author
Citation
Keywords
