Introduction
The prevalence of diverticular disease
has increased over the past few decades, with estimates of up to 2/3 of the
general Western population above 40 years of age currently being affected
[1-5]. Possible explanations for the increase in prevalence are increased
aging, dietary habits
and an increase in average body mass index [6].
Most people with this abnormality go unnoticed, but
complaints can occur. Diverticulitis leading to clinical symptoms is the most
common complication of diverticular disease. This affects approximately 10-25%
of the population with diverticular disease, elsewhere, a lower incidence also
has been reported [4,7,8].
Another complication is bleeding mostly due to
the concomitant use of anticoagulant therapy. Subsequently diverticulitis
composes a major health burden and results in 18.000 yearly hospital admissions
in the Netherlands [9]. Diverticulitis
is a clinical diagnosis based on a combination of clinical features such as
abdominal pain (especially in the lower left quadrant), changes in defecation
pattern, pain on physical examination, leukocytosis and high
CRP. The diagnosis is generally confirmed by a radiological examination.
Currently, CT-scan
is considered as the gold standard, with a sensitivity and specificity of 93%
and 97% [10]. Moreover, CT-scan
has the added possible benefit of defining disease
progression and adverse events such as abscess formation, fistula, obstruction
or perforation. Ultrasound may also be used, with reported sensitivity and
specificity ranges as high as those obtained by CT-scan in some studies
[11-14]. However, the credibility of ultrasound results is highly dependent on
the physicians experience and patient characteristics such as the amount of
abdominal fat.
It is well-known that diverticuli occur at older age
and those concomitant abnormalities like adenomas or even
cancer can be present [15]. However, due to overlapping imaging features of
diverticulitis with colorectal
carcinoma, it has been hypothesized that signs of colorectal cancer might
be missed on CT-scan. Several guidelines recommend routine screening for colorectal cancer when
the acute phase of diverticulitis has resolved, usually after 6-8 weeks
[16-20].
As previous studies have shown conflicting results
as to whether patients with diverticulitis have an increased risk of colorectal
cancer when compared to the general population, the question of whether
colonoscopy should be performed after an episode of acute diverticulitis
remains a topic of debate. In normal daily practice elective endoscopic investigation
of the colon has low additional diagnostic yield. For this reason a group of
consecutive patients diagnosed with diverticulitis was studied in order to gain
more information on presence of concomitant abnormalities.
Material
and Methods
The study is unique in the sense that the inclusion
criterion was not the clinical presentation of the patient but the radiologic
diagnosis of diverticulitis.
At the department of Radiology of the Zaans Medisch
Centrum, the community hospital of the Zaanstreek region in the Netherlands,
all consecutive requests for ultrasound and/or CT-scan of the abdomen in a
three year period, from 2016-2018, were studied. Only if the term Diverticulitis was
mentioned in the text of the application (either as current differential
diagnosis or past diagnosis) the procedure was included. All the selected
procedures were meticulously read and if there was diverticulitis diagnosed and
mentioned in the conclusion, than this specific investigation was included in
the present study.
From each of the selected files the hospital records
were searched for the presence of endoscopic investigation
of the colon and rectum. This is generally done 6-8 weeks after discharge. If
this was not done the reason for not doing an endoscopy was noted. The primary
outcome of the study was the prevalence of colorectal carcinoma. Secondary
outcomes were the prevalence of polyp (s) (adenomas as well as hyperplastic
polyps) and inflammation.
Statistical analysis was done with chi-square test for contingency tables and
t-test. The alpha level was set at 0.05.
Results
In the three year period 1410 consecutive ultrasound
investigation and/or CT-scans of the abdomen were performed. In 1024, procedures
diverticulitis! or diverticulitis?, was mentioned in the application (the
exclamation mark means that the clinician diagnosed
diverticulitis, the question mark means the clinician suspected
diverticulitis to be present). These consisted of 390 ultrasounds and 634
CT-scans. After exclusion 198 patients (19.3%) remained with the radiological
confirmed diagnosis of diverticulitis. The remainder had other diagnoses or
reasons for abdominal complaints.
One hundred twenty seven out of 198 (64%) patients
underwent an additional endoscopy (group 1) (6-8 weeks after the acute
episode). Seventy one patients (36%) did not undergo a colonoscopy (group 2)
after the acute episode. Table 1
shows the demographic characteristics of both groups. There was no difference
in gender or in age between both groups.
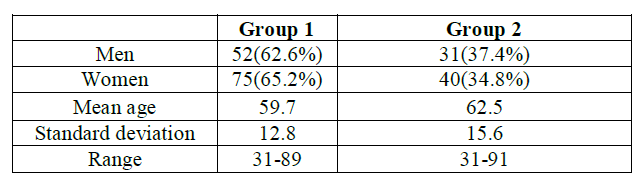
Table
1: characteristics of both groups of patients.
Colonoscopy showed
additional abnormalities in 22 (17.3%) of the patients. These were hyperplastic
polyp(s) in six, adenomatous polyp(s) in nine, polyps without histological
confirmation in three and segmental colitis in three (so-called SCAD =
segmental colitis associated with diverticulitis). Eleven polyps were larger
than 1 cm, and 10 smaller than 1 cm. Two male patients (43 and 61 years of age)
were diagnosed with sigmoid cancer. Both had non-subsiding diverticulitis with
abscess formation at the location of the tumor.

Table
2: Reasons for not doing an additional
colonoscopy.
Despite the radiological diagnosis, in group 1
diverticuli were not seen during colonoscopy in 8 patients (5 men, 3 women).
One additional patient underwent emergency surgery because of fecal
peritonitis. Diverticuli were seen in the resection specimen. A post-operative
endoscopy showed no more diverticuli. Of the remaining 7 patients one had an
undetermined colitis, and another one had a small adenoma. Table 3 presents the laboratory investigation of these 8 patients.
Number 7 was the patients with a sigmoid cancer. In
the course of the three years the number of additional colonoscopies decreased
significantly (Table 4).
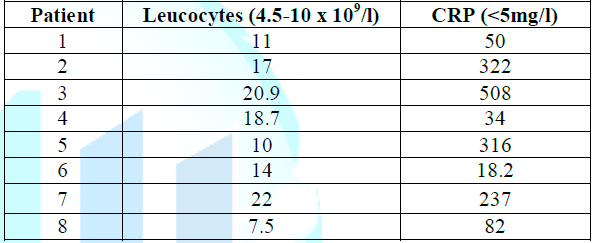
Table
3: Laboratory investigations in the patients
with clinical suspicion and radiological diagnosis of diverticulitis without
confirmation of presence of diverticuli during colonoscopy.
(= normal value).
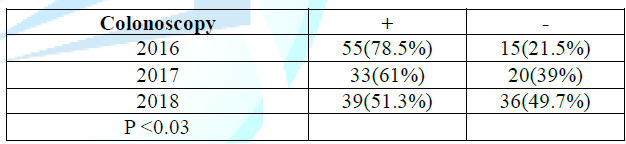
Table
4: The number of colonoscopies in the three
consecutive years after the diagnosis of diverticulitis.
Discussion
The purpose of the present study was to report on
the prevalence of colorectal
carcinoma after an episode of image proven diverticulitis in a non-selected
population. Colon
cancer was diagnosed in two patients (1.6%). During review of the CT-scans
of both patients, there were signs that raised the suspicion of a malignancy being
present in one patient. However, the radiologist reported diverticulitis as the
most likely diagnosis. The other patient underwent follow-up CT-scan because of
non-subsiding complaints, which showed persistent inflammation.
Afterwards, a malignancy was proven on colonoscopy.
The low percentage of 1.6% of colorectal carcinomas
found in our population is consistent with the majority of published research.
However, there has been some variability in the percentages reported for
colorectal carcinomas and polyps after an episode of diverticulitis. Disbrow et
al. reviewed the literature from 1984 to 2015 and reported on two systematic
reviews [21]. These reviews indicated a pooled prevalence for colorectal
carcinoma in uncomplicated diverticulitis of 1.5% and 0.7% respectively.
Moreover, Sharma et al. also reported on complicated diverticulitis and found a
pooled prevalence for colorectal
carcinoma of 10.8% for this group. [22,23]. As already stated, in the
present study both patients with colon cancer had complicated diverticulitis,
whereas no colon cancer was found in patients with uncomplicated disease.
The most recent systematic review by Meyer et al.
included 31 studies, compromising 50,445 patients, and found a pooled
prevalence for colorectal carcinoma of 1.9% [24].
When dividing this population into complicated and
uncomplicated disease, a significantly higher percentage of 7.9% was found for
complicated diverticulitis versus 1.3% for uncomplicated diverticulitis [24]. Despite
this low percentage in uncomplicated diverticulitis routine colonoscopy in all
patients after diverticulitis is still recommended.
These results from the literature add to the
discussion whether colonoscopy is mandatory after an episode of diverticulitis.
Is the incidence of colorectal cancer after diverticulitis higher than with the
incidence in the general population? A large study addressing the prevalence of
colorectal carcinoma
in the general population is by Pox et al.
They report on almost three million screening
colonoscopies performed in Germany, and they found a colorectal carcinoma
percentage of 0.9% [25]. The prevalence of colorectal carcinoma found in the
current study is only slightly higher when than that of the general population.
In addition, both patients with malignancy in our study showed that
diverticulitis and a colon cancer can be present at the same time.
Thus diverticulitis is not a risk factor for
developing colorectal cancer, and that the necessity of performing a
colonoscopy may have been exaggerated. Therefore, colonic endoscopic evaluation
should be preserved for patients with a higher risk on colorectal cancer. This
includes complicated diverticulitis, a protracted clinical course or uncertainty
of the diagnosis on CT-scan.
Of course, the present study has several
limitations. All cases came from a single center study and not all diagnoses of
image proven diverticulitis were followed up with a colonoscopy. On the
other hand a large number of these patients had a previous colonoscopy showing
diverticuli, and the population under study is a non-selected group from the
general population without selection bias.
A recent guideline in the Netherlands does not
recommend colonoscopy after a period of uncomplicated
diverticulitis [26]. This guideline was published in May 2018, and since
then the number of colonoscopies has decreased (Table 4).
In conclusion, previous studies and the data in the
present study indicate that it is safe to omit colonoscopy after an episode of
uncomplicated diverticulitis. Only in cases of complications or persistent
complaints should cancer be part of the differential diagnosis and a subsequent
colonoscopy be performed.
References
- Ferzoco LB, Raptopoulos V and Silen W. Acute
diverticulitis (1998) N Engl J Med 338: 1521-1526. http://dx.doi.org/10.1056/NEJM199805213382107
- Painter NS and Burkitt DP. Diverticular disease of
the colon: a deficiency disease of Western civilization (1971) Br Med J 2:
450-454. https://doi.org/10.1136/bmj.2.5759.450
- Painter NS and Burkitt DP. Diverticular disease of
the colon, a 20th century problem (1975) Clin Gastroenterol 4: 3-21.
- Parks TG. Natural history of diverticular disease of
the colon (1975) Clin Gastroenterol 4: 53-69.
- Tursi A. Acute diverticulitis of the colon-current
medical therapeutic management (2004) Expert Opin Pharmacother 5:55-59. http://dx.doi.org/10.1517/14656566.5.1.55
- Lee TH, Setty PT, Parthasarathy G, Bailey KR,
Wood-Wentz CM, Fletcher JG, et al. Aging, obesity and the incidence of
Diverticulitis: A Population-Based Study (2018) Mayo Clinic proceedings 93:
1256-1265. http://dx.doi.org/10.1016/j.mayocp.2018.03.005
- Stollman N, Raskin JB. Diverticular disease of the
colon (2004) The Lancet 363: 631-639. http://dx.doi.org/10.1016/S0140-6736(04)15597-9
- Loffeld RJ. Long-term follow-up and development of
diverticulitis in patients diagnosed with diverticulosis of the colon (2016)
Int J Colorectal Dis 31: 15-17. http://dx.doi.org/10.1007/s00384-015-2397-1
- Prismant (2010) Data of hospitalization in the
Netherlands.
- Ambrosetti P, Grossholz M, Becker C, Terrier F and
Morel P. Computed tomography in acute left colonic diverticulitis (1997) Br J
Surg 84: 532-534. http://dx.doi.org/10.1046/j.1365-2168.1997.02576.x
- Puylaert JB. Ultrasound of colon diverticulitis
(2012) Dig Dis 30: 56-59. http://dx.doi.org/10.1159/000336620
- Schwerk WB, Schwarz S and Rothmund M. Sonography in
acute colonic diverticulitis (1992) Dis Colon Rectum 35: 1077-1084. http://dx.doi.org/10.1007/bf02252999
- Zielke A, Hasse C, Bandorski T, Sitter H, Wachsmuth
P, et al. Diagnostic ultrasound of acute colonic diverticulitis by surgical
residents (1997) Surg Endosc 11:1194-1197. http://dx.doi.org/10.1007/s004649900567
- Zielke A, Hasse C, Nies C, Kisker O, Voss M, et al.
Prospective evaluation of ultrasonography in acute colonic diverticulitis
(1997) BJS 84: 385-388. https://doi.org/10.1046/j.1365-2168.1997.02604.x
- Koning MV, Loffeld RJ. A survey of abnormalities in
the colon and rectum in patients with haemorrhoids (2010) BMC Gastroenterol 10:
74. http://dx.doi.org/10.1186/1471-230X-10-74
- Andersen JC, Bundgaard L, Elbrond H, Laurberg S,
Walker LR, et al. Danish national guidelines for treatment of diverticular
disease (2012) Dan Med J 59: C4453.
- Biondo S, Lopez Borao J, Millan M, Kreisler E and Jaurrieta
E. Current status of the treatment of acute colonic diverticulitis: a
systematic review (2012) Colorectal Dis: The official journal of the
Association of Coloproctology of Great Britain and Ireland 14: e1-e11. http://dx.doi.org/10.1111/j.1463-1318.2011.02766.x
- Fozard JB, Armitage NC, Schofield JB and Jones OM.
ACPGBI position statement on elective resection for diverticulitis (2011)
Colorectal Dis: The official journal of the Association of Coloproctology of
Great Britain and Ireland 13: 1-11.
- Jacobs DO. Diverticulitis (2007) N Engl J Med 357:
2057-2066.
- https://www.uptodate.com/contents/acute-colonic-diverticulitis-medical-management
- Disbrow M, Foxx-Orenstein A and Agrwal N. Utility of
colonoscopy to exclude underlying malignant polyps after resolution of
uncomplicated diverticulitis (2015) J Am Osteopath Assoc 115: 720-723. http://dx.doi.org/10.7556/jaoa.2015.147
- Daniels L, Unlu C, de Wijkerslooth TR, Dekker E and
Boermeester MA. Routine colonoscopy after left-sided acute uncomplicated
diverticulitis: A systematic review (2014) Gastrointest Endosc 79: 378-389. http://dx.doi.org/10.1016/j.gie.2013.11.013
- Sharma PV, Eglinton T, Hider P and Frizelle F.
Systematic review and meta-analysis of the role of routine colonic evaluation after
radiologically confirmed acute diverticulitis (2014) Ann Surg 259: 263-272.
- Meyer J, Orci LA,
Combescure C, Balaphas A, Morel P, et al. Risk of colorectal cancer in patients
with acute diverticulitis: a systematic review and meta-analysis of
observational studies. Clin Gastroenterol Hepatol: The official clinical
practice journal of the American Gastroenterological Association 17:1448-1456. http://dx.doi.org/10.1016/j.cgh.2018.07.031
- Pox CP, Altenhofen L, Brenner H,
Theilmeier A, Von Stillfried D, et al. Efficacy of a nationwide screening
colonoscopy program for colorectal cancer (2012) Gastroenterology 142:
1460-1467. http://dx.doi.org/10.1053/j.gastro.2012.03.022
- https://richtlijnendatabase.nl/richtlijn/acute_diverticulitis/follow-up_colonoscopie_na_diverticulitis.html
*Corresponding author: Loffeld RJLF, Department
of Gastroenterology, Zaans Medisch Centrum, Zaandam The Netherlands, Tel:
31-75-6502779, Fax: 31-75-6502379, Email:
Loffeld.r@zaansmc.nl
Citation: Dijkhorst PJ and Loffeld RJLF. Routine
colonoscopy after diverticulitis should not be performed to rule out colorectal
cancer (2019) Edelweiss Cancer OA 1: 29-32.