The integration of Indian economy in the
world is stronger than ever before and combined with its current demographic
dividend, India is sure to witness an ever-increasing economic growth rate.
However, the era of demographic dividend will end soon and the generation of baby
boom will soon join the cohort of elderlies and the generation which was an
active contributor of economic progress will be the largest demander of health
and social security schemes in next few years.
With an increase in medical and clinical research
combined with other perquisites the death rates have come down substantially
across the globe and thus demographic ageing is a global phenomenon and picking
up momentum in all parts of the world. Dr. Margaret Chan, Director-General of WHO
asserts that “Today, most people, even in the poorest countries, are living
longer lives,” (WHO). However, the elderlies particularly in developing and
poorer nations are mostly deprived of basic amenities and
have little or no access to Social support, security and insurance making them
physically vulnerable and economically dependent on their heirs. The situation
is substandard for women in these countries since they have higher life
expectancy but less social
security and economic independency relative to males.
Along with the changing time and
the changing lifestyle of people, the Earth has picked up a speed at which it
is changing too. With this, resources are depleting at a high speed and our
ecosystem and the environment are also deteriorating at a rapid rate. With
these alterations, theres a continuous transition in the health patterns as
well as in the diseases from which people suffer. The new age diseases are
perfectly correlated with increasing mental exercise and declining physical
activities leading to excessive pressure of mental problems like Depression, stress, Dementia etc. However,
owing to stringent social stigma attached to mental illness, these
diseases are often unreported or underreported and many a times are ignored to
be considered as a serious ailment. Thus diseases associated with mental
ability are not extensively integrated in the public policy domain despite
their high prevalence rate.
From being one of the most
advanced empires during Indus valley civilizations to being the first nation to
realize the significance of primary healthcare,
India has always excelled in bringing transformations and moving towards a new
milestone. Proving to be a cradle to some of the most intellectual people,
India has been fetching great minds since eternity whose cumulative knowledge
has helped in evolving the healthcare system
which we witness in the present day. However, given the large population of
this nation, providing basic health services, free of cost, seems to be a
mirage. But with the prevailing poverty in the nation, primary healthcare is as
necessary as having food, clothing or a shelter to live under as Yusuf Hamied has
asserted while referring to India signing up for TRIPS, Hamied stated that
“With a population of 1.3 billion, India cant afford a monopoly in healthcare.
Monopolies lead to higher prices and we cant allow them in a country like India
with so much poverty and misery.” Thus providing affordable primary healthcare
is not a luxury, but rather, a necessity in a diverse nation like India.
Unlike other nations, India has
made a distinction by focusing on the environment of the problem and not just
the physical sickness of the patient. Way of treating sick and unwell people
has evolved from the use voodoos and spirits to the stars and gods to the
modern technology and equipments. Medicines have, as
well, been evolved from the use of plants and herbs to the problem-specific and
prescribed medicines. This evolution is not just restricted to medicines and
the means of treating a problem, but also to the diseases from which we suffer.
In lieu of the demographic change
combined with epidemiological transition or shift in the composition of
diseases the policy paradigm should involve effective interventions to ensure
that longevity in the life is accompanied with good health and assurance of
dignified lives to the elderlies. In turn it will ensure not only betterment of
an individual but for the society as a whole. (WHO). This is particularly
important for developing and growing economies like India where the demographic
transition has speeded up but the reach of public health infrastructure is
still on a marginal stage owing to the three major constraints in India namely,
“shortage of doctors across India”, “Poor medical infrastructure” and “Poor
health insurance resulting in a higher share of private expenditures” that
erodes the health care system in (Nadkarni, 2013)
Research
Objectives
In an era where major challenges
lie in front of India to serve the growing needs for healthcare services
arising from demographic transition, the present research aims to assess the
changing demographic trends and analyze the availability, requirement and
constraints pertaining to the delivery of health care services in India. This
study further reflects upon inter and intra socioeconomic differentials across
various groups in receiving the free medical services. The present research
would highlight major reasons for increasing share of mental diseases in
total disease burden with a specific focus on Dementia which despite being a
big shark is yet unnoticed by the public.
Literature
Review
There exists a wide range of
literature validating the indispensable link between demographic transition and
epidemiological transition. Omran (1971) asserted that the pattern of
demographic structure is determined not only by social, economic and demographic factors
but also by epidemiologic factors, which predicts the long-run effects of
changing disease patterns on the health of the population. (Omran A. R., 1971).
Omrans (1971) ideas were opposed by Mackenbach (1994) on grounds of the
underlying assumption of treating all the nations equally and assuming uniform
transition in all the countries by taking only western countries in the sample.
(Mackenbach, 1994). Omran (2005) has further strengthened his arguments on this
link by asserting that changes in mortality pattern
widens the gap between birth and death rates owing to the impact that
epidemiological transition has on fertility rate, sex ratios, dependency ratio
etc. and thus changes in epidemiological structure alters the composition of
population. (Omran, 2005)
The change is not constrained to
age-structure but also there are highly prevalent changes in the lifestyle
which involves the vices of less physical activity, less social inclusion, more
mental and mechanised work, unhealthy eating habits, etc. Further, over the
decades the world has experienced major depletion of its natural resources,
ecosystem and environment which has wide ranging repercussions on ones health
and wellbeing. Climate changes and increased urbanization accompanied with
changes in lifestyle and human
behaviour has resulted in continuous transitions in disease patterns.
(Lindahl & Grace, 2015)
Frenk J et.al.(1991) has
identified different stages of epidemiological transition for developing
nations. The authors asserted unlike in most developed nations where in the
first stage there is a shift from infectious to non-communicable diseases as a
dominant cause of death, developing countries face both pre-and-post transition
phase diseases which often reoccur in the second stage. The authors have
highlighted the idea of epidemiological polarization i.e. the differences in
disease pattern are observable between different social groups or different geographical areas
within the same country. (Frenk, et al., 1991)
One of the examples where
epidemiological transition can easily be seen is with the case of dementia. Dementia is a disease
where mental ability of a person is hindered to such an extent that his/her
daily life gets interfered due to this. In a study by Suh Shah (2001),
epidemiological transition was found in the diseases like Dementia and
Alzheimer and it was found that Alzheimers disease (AD) is more prevalent than
Vascular Dementia (VaD) in Korea. Similar results were found in the nations
like Japan, China, America and Europe, however contrary to other nation it was
found that both AD as well as VaD prevailed equally in case of India. (Suh
& Shah, 2001)
Rizzi et.al. (2014) concluded
from their study that the dementia patients are increasing at a rapid rate. The
authors further asserted that though the cases are increasing in both developed
as well as developing nations but developed countries, like America show more
cases of Dementia and Alzheimers
disease than the less developed countries However, the reason behind this
could be that least developed nations do not have that updated technology to
properly diagnose such diseases and also, theres no methodological uniformity
in these nations. (Rizzi, Rosset, & Roriz-Cruz, 2014)
However, irrespective of lag in
identification of the disease it can be safely concluded that with the
ever-increasing population worldwide, the number of people suffering from these
diseases is escalating as well. Prince et. al (2013) asserted that in 2010, an
estimate of 35.6 million people was found to be enduring Dementia with the
number getting doubled almost every 20 years. (Prince, Bryce, Albanese, Wimoc,
Ribeiro, & Ferri, 2014).
With an increasing focus upon
mental health, the research on issues pertaining to mental illness has
increased in developing nations. Recently, 19th national conference of ARDISI
(Alzheimers and Related Disorders Society of India) was held in Mumbai, India .
It implored to give more attention to these diseases as it was highlighted that
by 2020, Dementia cases in India will rise to about 7 million in coming years
and shockingly, it will further rise to 13-14 million by the end of the year
2050. In the conference, major focus was put on Dementia and to increase the
awareness level among people about it.
This increase in research can
also be attributed to the estimates of WHO (World Health Organisation),
according to which, in developing nations like India, the population of aged
people is increasing and with this increase in their population, soon dementia
will become an epidemic among old people by 2025. An urgency was felt when it
was realised that estimated annual numbers of cases of Dementia are the highest
in Asian countries and in low income countries, such as India, the most
stricken age group from Dementia will be the youngsters of the country. (WHO)
With different perspectives and
approach towards these diseases, people stand firm in carrying diverse stance
from one another. Seeking a single solution to the problem of Dementia still
carries a big question mark along with it. One of the suggestive measures from
amongst millions of poles apart viewpoints is from Wimo et.al. (2013) who in
their study has asserted that world-wide cost of dementia will increase as the
gap between diagnosis
and treatment widens thus investing more in research and cost-effective
approaches in the present is the only solution to safeguard our coming progeny
from the perilous consequences of it. (Wimo, Jönsson, Bond, Prince, &
Winblad, 2013)
With so many views and studies of
different researchers, the studies on India have been increasing as well,
despite the fact that the list of cases of these diseases particularly
diagnosed cases) is not that huge as compared to developed nations. It is also
asserted that in a few years, the cases of Dementia and other mental problems
will be at least two folded. Therefore, the need was realised to do more
research on these diseases to protect future generation and to make them aware
as to how to save themselves from suffering from it.
Significance of the Study: Indian
constitution regards “Health as a state subject” and thus there are persistent
variations in the health
outcomes across different states in India. Differences in interventions and
other background social demographic differentials; literacy rate for instance
are accounting for such differences. While states like Tamil Nadu, Kerala have
progressed in both health and education others like Bihar, Uttar Pradesh
have left behind. Although the concept of “Universal Health Coverage” has been
articulated in the Twelfth Five Year Plan but in light of changing demographics
accompanied by changes in the social, cultural and economic institutions, India
needs to increase the momentum in coming decades to effectively provide health
goods at affordable prices accounting and controlling for disparities and
inequities persistent in India. (Ayushi Gudwani, 2012) The study would be of
great relevance to policymakers since it will unveil the current potential and
challenges ahead on the present healthcare infrastructure to cater the growing
needs of changing demographics.
Data
and Methods: The data for the above study is sourced from the large scale
surveys including NSSO 71st Round, Census 2011, CEIC, etc. The authors adopt
structured equation model and margins plot to measure the differences in
healthcare expenditure across different social groups and mediating factors.
The structured equation model (SEM) used to highlight the differentials in medical expenditure
incurred by different socio-economic groups and interaction factor is as
follows:
Description
of Variables
lo: Log of (total medical
expenditure-amount reimbursed through insurance)
age group =
0, if age <=59
=
1, if age >60
ecdp = 0, if economically independent
= 1, if economically dependent
se = 0, if sector is rural
= 1, if sector is urban
sex = 0, if male
= 1, if female
Insu = 0, if insured
=
1, otherwise
Hh size = size of the household
The SEM has been used to take account of interactions and multiple relations
present in the model. The exogenous independent variables are converted into
dichotomous variable
Further, the paper reviews
Dementia in the light of existing research and then will describe the
seriousness of the issues and suggest relevant policy measures to deal with
Dementia. Dementia will be studied through various secondary reports.
The study henceforth is divided
into three sections. First section cover the dynamics of demographic
transition, second section studies the inter and intra group differentials in
healthcare expenditure and the last section lays down the factors responsible
for epidemiological transition with a specific focus on Dementia.
Dynamics of Demographic Transition
The
demographic structure of India is changing at a rapid pace with an increase in
median age from 20 in 1980 to slightly less than 25 in present and is expected
to rise further to 29 by the year 2020, and the proportion of old age
population (60 and above) is expected to rise substantially from 7% in 2005 to
20% in 2050 (Subaiya, 2011). Figure 1 shows the trends in Birth rates and death
rates across diverse group of Indian states. A close examination of the figure
clearly depicts that states belonging to Empowered Action Groups (EAG) started
with very high figures of birth and death rates and despite a noticeable
decline in past two decades. Contrarily Southern States has started with low
birth rate and relatively high death rates as
compared to Union Territories (UTs), North-Eastern States (NEs) and other
states of India. Thus the pace of demographic transition varies sharply across
different state groups.
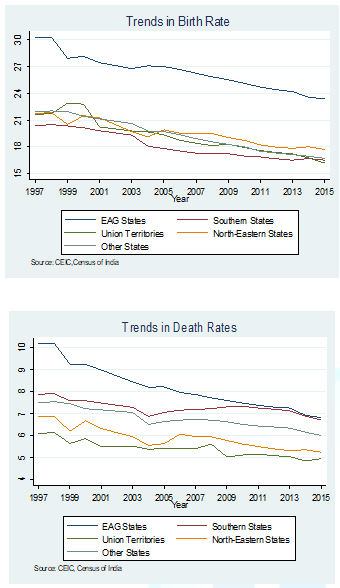
Figure 1: Trends in Birth and Death rates.
The birth rates have declined considerably but death
rates have remained relatively high. Overall India states are witnessing a
demographic transition by moving from a phase of high birth and death rates to
declining birth and death rates. The figure clearly implies that India is
currently moving from middle transitional phase to late transitional phase
where birth rates are continuously declining, however decline in death rates
have been slowed down. (P.M.Kulkarni, 2014).
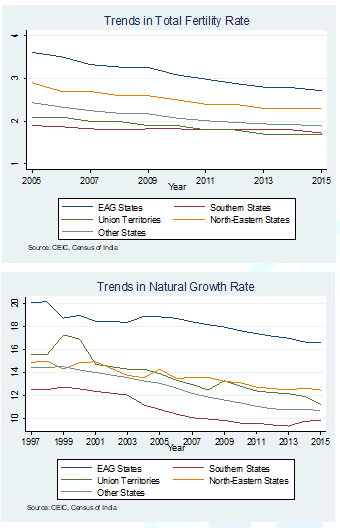
Figure 2: Trends in total Fertility Rate and Natural
growth Rate.
The trends in fertility
rate and natural growth rate depicted in Figure 3 validate the fast rates of
decline in birth rates across all state groups. It is noteworthy to mention
that the fertility rate in Southern states and UTs of India is falling below
the normal replacement rate of 2.1 thus clearly indicating that in near future
there will be less proportion of population in the 0-14 age group. This phase
of demographic transition has yielded a large proportion of working-age
population (approximately 60 percent of total population, as per Census 2011)
to India. The current scenario has a potential economic advantage to India as
acknowledged by Aiyar and Mody, 2011 Demographic dividend in India has a
potential to contribute around 2 per cent annually to the GDP for the next
twenty years. (Aiyar & Mody, 2011).
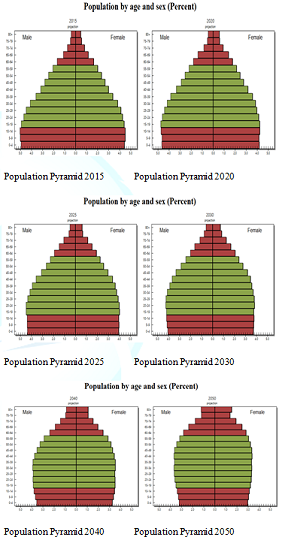
To view the figure of population pyramids click below
Figure 3: Population Pyramids.
However, the trend will
change very soon in India and the population group who are the major
contributors to demographic dividend will soon join the cohorts of elderly
population and India will witness a record-high number of elderlies. The share
of elderlies in the total population is 8.6 per cent, out of which only 41 per
cent are working as per Census 2011. The figures clearly indicate the strength
of demand for social goods like health, pension etc. This demand will increase
manifolds with changing demographic structure which is more skewed towards
elderly population as depicted in Population Pyramids in Figure 4.
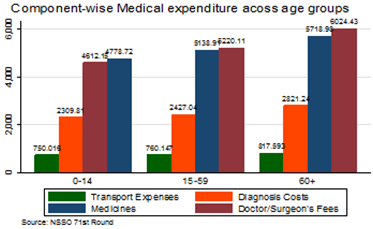
Figure 4: Medical Expenditure across Different Age Groups.
Inter
and Intra Group Differentials in Healthcare Expenditure
With an improvement in technology
and innovations in medical research, Life Expectancy has increased but the new
technology is expensive and is beyond the reach of masses. Although Indian
government has strengthen its health infrastructure over the time by making the
health care services cashless. Despite that people are incurring high medical
costs which vary across different social groups. The differences are not
restricted to inter-group but are also prevalent across intra groups.
Table 1 shows the results of
Structured Equation Model. It can be inferred that as we move from 0 to 1 i.e.
from younger population to elderlies the probability of being insured gets
reduced substantially while medical expenditure rises. The situation is
substandard for females who have 1 per cent less changes of being insured and 2
per cent higher medical expenditure than males. People belonging to urban
sector, though has approximately 7 per cent higher medical expenditure than
their rural counterparts but are highly probable to get insured. Elderlies are
more dependant economically than the younger population and also less probable
to get insured and given that they are more prone to illness, their medical
expenditure is substantially higher and thus elderlies pose potential demand
for the social services like pension, insurance, free health etc.

Table 1: The results of Structured Equation Model
Demographic change is accompanied
with changes in the social institutions whereby large number of elderlies are
left with little or no social economic or financial security from their heirs.
The inadequacy in economic independency is accompanied with high medical costs
on all the components as shown in Figure 4.
The situation gets aggravated
depending upon ones position in the socio-economic hierarchy. As depicted in
Figure 5 elderlies belonging to the age group of 60 + have relatively very high
medical expenditure as compared to the other two-age groups; however within the
similar age group females have higher medical expenditure as
compared to males. One noteworthy observation from the figure is significant
differences across sectors. Across all age groups people belonging to urban
sector have significantly higher medical expenditure as compared to their rural
counterparts. The reason for the same can be ranging from non-availability of
proper medical services in rural areas to high prevalence rate of diseases in
urban areas owing to rapidly changing lifestyles making people more and more
prone to falling ill both physically and mentally.
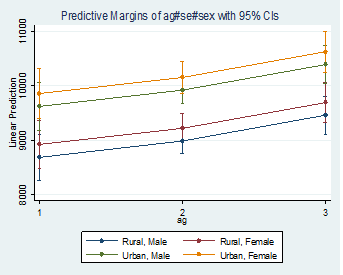
Figure 5: Differences in Medical Expenditure Across Age
Group, Sector and Gender.
Epidemiological
Transition and Dementia
Demographic change has been
accompanied with epidemiological transition a term attributed to shifting
patterns of mortality and diseases. Over time the number of deaths ascribed to
changing lifestyles (like stress, smoking etc.,
exposure to artificial substitutes of nature like excessive use of pesticides
in agriculture, excessive reliability on medicines) degradation in the
environment has increased. The basic question that arises now is what could be
the possible reasons behind these transformations. Various authors have
highlighted different factors responsible for epidemiological changes, but the
most common ones in the medical sciences are as shown in Figure 6.
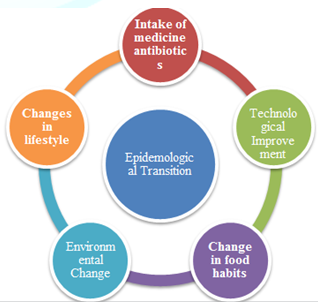
Figure 6: Common Causes of Epidemiological transition.
While evolution is an effect, the
cause of this lies in various leaves. One of the thousands of reasons for this
alteration is too much dependence upon medicines and antibiotics. It is
said that prevention is better than cure and in the race of preventing
themselves from any sort of disease, people are becoming over conscious and
rely on medicines for even a minor disease. When antibiotics started to become
a solution for every problem, it inversely affected the tolerance power of
people making them more addictive to medicines, leading to permanent increasing
the body temperature of humans. With this new temperature level, our body
system starts working to adapt this change, leading to reaching a new level of
stability, making us immune to some virus/bacteria while making us prone to
others. This change in adaptability causes epidemiological transition. Further,
Jones et al. suggests that “medicine struggles to keep up with the changing
burden of disease” (David S. Jones, 2012) implying the continuity of transition
in disease patterns faster than evolution in medical sciences
Apart from the above, others
reasons for epidemiological transition may include changes in lifestyle
(McKeown, 2009) and food habits or nutrition transition
(Popkin, 2002), environmental changes, technological improvements and mobility
of living beings and non-living beings from one place to another that alters
the natural working of biodiversity. (Wahdan, 1996)
All these changes and evolution
not only brings instability in the ecosystem but also, hinders the natural
working of species for which they were designed. Resultantly, an ordinary allout
does no harm to mosquitoes and little cuckoo birds are nowhere to be seen. This
has also adversely affected human beings leading to their speed of
transformation being much higher than the speed of adaptation. Prime example of
this variation in speed is overlooked attention to mental health. Since
revolution, the only attention that has been given is on the conventional part
of physical health, whilst mental health continues to be ignored. Furthermore,
if we look closely, the root cause of all the diseases reflects mental health as it is
constantly said that most of our illness is psychological, despite these
sayings and evidences, mental health is still aloof from the attention it
deserves and still, all the mainstream methods of putting spotlight to only
physical health can be seen.
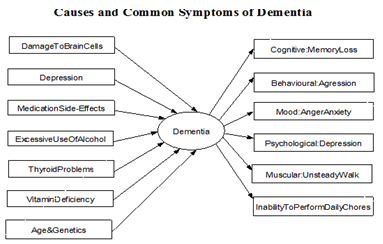
Dementia is one such disease that
verifies that its now time to focus more on mental health and not just the
physical counterpart of it. Dementia is a disease where-in mental ability of a
person is hindered to such an extent that his/her daily life gets interfered.
Its a wide term that illustrates an extensive range of symptoms, ranging from
communication problems to visual impairment to memory loss. According to
medical sciences, Dementia is a result of damage of brain cells which can
happen due to any of the factors such as depression, side effects of medicines,
excessive consumption of alcohol or smoking, health problems such as thyroid or
vitamin deficiencies and early signs of Dementia include short-term memory
loss, trouble finding the correct words, mood swings, struggling while
completing normal day-to-day tasks, confusion beyond normal and being
repetitive.
Statistically, approximately 46
million people are currently suffering from dementia all over the world, being
4 million in India only. It is also said that every 3 seconds, someone develops
dementia around the world. According to World Alzheimer Report, 2015 the
numbers of dementia cases worldwide are expected to increase manifolds by 2050
with more than one-fifth of cases occurring in lower-middle income countries,
owing to faster rates of increase in aging population as depicted in Figure 8.
The lower-middle income countries not only have high number of dementia cases
but also are embedded with high-cost health care. Dementia is a proliferating
disease estimated to cost US$ 818 billion worldwide in the year 2015 and the
social cost is projected to increase up to US$ 2 trillion by 2030, such huge
costs exceeds the market values of large companies like Apple (Prince, Wimo,
& et.al., 2015).
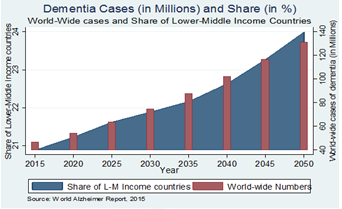
Figure 8: World-Wide cases of Dementia and Share of
Lower-Middle Income Countries.
Dementia is not only restricted
to developed world but is becoming an increasing concern for the developing
nations like India. The burden of Dementia is expected to multiply manifolds in
coming years as projected in Dementia India Report, 2010 and depicted in Figure
9 the number of dementia cases will almost double in less than a decade with
Uttar Pradesh having the highest number of patients in 2006 and 2011.
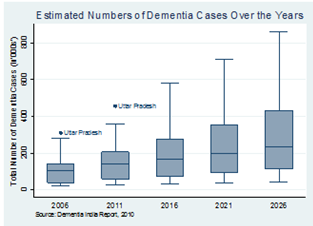
Figure 9: Estimated Number of Dementia Cases (in 000’s)
in India over the Years.
Similar to differentials in the
pace of demographic transition across different groups of Indian states, there
are stark variations in the burden of dementia across different state groups as
depicted in Figure 10.
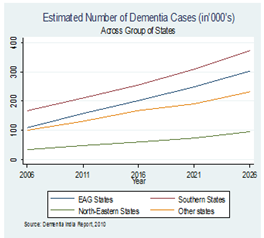
Figure 10: Estimated Number of Dementia Cases (in 000’s)
across Different India States.
Figure 10 clearly shows that the
southern states that are experiencing fast changes in demographic structure
have notably highest estimated numbers of Dementia cases across years. EAG
states which started with comparative numbers to other states like Delhi,
Punjab, Haryana, etc. are following similar trend as southern countries with
regard to the estimated number of dementia cases. North-Eastern states have
already started with low numbers are expected to experience a minor increase in
the number of Dementia cases.
The differences are not
restricted to group of states but also vary across age groups as depicted in
Figure 11.
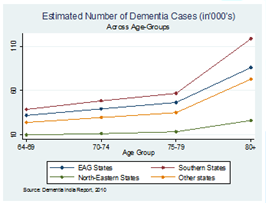
Figure 11: Estimated Number of Dementia Cases (in’000’s)
across age groups.
Figure 11 asserts that
irrespective of state group, the estimated numbers of dementia cases are
positively associated with age-group. The numbers shoot-up for the age-group of
80+ and the numbers are very high for Southern states of India.
The states which are blessed with
exceptionally well demographic indicators like literacy rate, mortality rate
etc. which are relatively very low has highest number of estimated cases of
dementia. Southern states were amongst the first few states to recognise the
importance of public provision of health services in India. The effects of
which are clearly visible in the key health indicators like IMR, MMR etc.
However, the present scenario calls for an increased attention on the mental
health-being as a part of public health policy
to ensure both the physical as well as mental well-being of the elderlies.
Discussion, Conclusion and Policy
Recommendations:
Time has come to show Indias
strength to the world. Lets recognise our demographic dividend & present
image of a Skilled India to the world.
- Narendra Modi
Undoubtedly, India is blessed
with the demographic dividend and India is in the path of becoming one of the
strongest global economies and in order to achieve the full potential of the
large army of labour force it is essential to focus upon labour productivity
which is a direct function of ones health. (Sharma & Bothra, 2017). While
this phase of Demographic transition has large avenues of economic benefits
owing to increased workforce, the situation will change in the coming two
decades. There is a continuous decline in both birth and death rates in India
and thus in coming twenty years India will have a large pool of elderlies and
there will be immense pressure on the government to ensure that the longevity
in life is accompanied with social security, good health and well-being.
Along with demographic changes
India has witnessed changes in the lifestyle and shifts in the composition of
food intake which is relatively unhealthy these factors combined with
age-specific diseases calls for a transformation in the health care market. The
changes have been observed in the social institution as well and breaking-up of
Hindu joint family structure and separation of children from parents in flight
of getting good jobs or personal reasons are examples of social change. This
change directly affects the mental well-being of elderlies. Dementia is one such
disease that should be our topmost precedence and requires a lot of
consideration since the disease has direct association with the persons ability
to perform his day-to-day activity.
In a follow up study of 10 years
done on Dementia by Mathuranath et al (2012), it was found that the cases of
these diseases are much higher in Southern India as compared to rural north
India. Not only these cases are more than those reported in China but also,
they are only marginally lower than those in Western countries. (Mathuranath,
et al., 2012) The present research has indicated similar findings that southern
states which are relatively more fast-paced in terms of improving literacy and
combating mortalities are and in future will be home to highest number of
dementia cases. These differences across group of states clearly indicate the
need for specific target-oriented health a policy that vary across states, but
is directly aimed at improving mental health-being.
With so many views and studies of
different researchers, the studies on India have been intensifying as well. It
is also asserted that in a few years, the cases of Dementia and other mental
problems will be more than doubled. Consequently, the need has started to
comprehend that more research on these diseases should be carried forward to
protect future generation and to make them aware with the means of saving
themselves from suffering from it. (Das, Pal, & Ghosal, 2012)
Dementia is no longer being
restricted to old-age but is increasingly prevalent even in youngsters. Keeping
the urgency in mind, many organisations have been formed and many help lines
are formed to provide aid to people suffering from these diseases or their
family members. Various portals have been established to help elderly people to
seek treatment by themselves and all these resources, help lines and portals
have been segregated as per the age groups and the disease to provide
specialised treatment.
However, even after realizing the
urgency and despite all these efforts and thorough studies, the resources to
treat people suffering from Dementia or Alzheimers disease are not sufficient
in India. Despite of the fact that more than 4 million people in India are
suffering from some form of Dementia, still the proper treatment and diagnosis
is not yet available in the country. Finally, if we see the behavioral pattern,
in spite of this disease prevailing at a very high number, the proper awareness
is still not there among patients and people and due to lack of proper
knowledge, people tend to overlook the symptoms and dont consult or seek a proper
treatment. Dementia and other mental illness further remains underreported
owing to societal stigma attached to it.
Modern technology, change in
lifestyle and others, has many repercussions on human health. Dementia
is one such repercussion which hinders the normal day-to-day working of a
person and might lead to other hazardous diseases like Alzheimers disease,
Jakobs disease etc. With Dementia, come other self-destructive symptoms and
activities like taking excessive stress, increasing mental work as compared to
physical and being socially isolated that only puts more harm to the person
suffering from it and those around him.
Therefore, it can be cured by
taking counselling for depression starting from school level and maintaining a
balance between mental work load and physical work load. Morning walks,
reduction in consumption of alcohol and increasing social interactions along
with rejuvenating activities such as yoga, meditation and doing exercises are
some of the mainstream solutions to it. Apart from these, government should
take preventive measures by increasing awareness among people so as to prevent
themselves from this disease before the need of curing it arises.
Thus there is a need for
transition in the healthcare markets which are not well equipped to meet the
rising demands of changing disease pattern is required. There is an
indisputable need to expand the present health infrastructure to include the
use of modernized equipment, better infrastructure and quality doctors to
provide the social good named as “Health for All” to all the age groups and
particularly the ageing group which in turn will have a high demand for health
services. The epidemiological transition has speeded up and along with increase
in non-communicable diseases, mental issues like stress, depression, Dementia
are also-increasing and curing them requires not only intensive research on the
possible diagnosis and treatment measures but also on increasing awareness
amongst the masses. This includes collective efforts of government and public
owing to large resource requirement and thus calls for an increased
Public-Private partnerships and Corporate Social Responsibility in the health
sector.
References
1. Nadkarni
JK. All about India: A health care market in transition (2013) Centre for
Health Market Innovations.
2. Omran
AR. The Epidemiologic Transition: A Theory of the Epidemiology of Population
Change (1971) The Milbank Memorial Fund Quarterly 49: 509-538. https://www.jstor.org/stable/3349375
3. Mackenbach
JP. The epidemiologic transition theory (1994) Journal of Epidemiology and
Community Health 48: 329-331. https://dx.doi.org/10.1111%2Fj.1468-0009.2005.00398.x
4. Omran
AR. The Epidemiologic Transition: A Theory of the Epidemiology of Population
Change (2005) The Milbank Quarterly 83: 731-757. https://dx.doi.org/10.1111%2Fj.1468-0009.2005.00398.x
5. Lindahl
JF, Grace D. The consequences of human actions on risks for infectious
diseases: a review. (2015) Infection Ecology & Epidemiology 5: 48. https://dx.doi.org/10.3402%2Fiee.v5.30048
6. Frenk
JTF, Bobadilla J, Stern C, Lozano R, Sepúlveda J, et al. The epidemiologic
transition in Latin America (1991) Pan American Sanitary Bureau 111: 485-496.
7. Suh
G, Shah A. A review of the epidemiological transition in
dementia--cross-national comparisons of the indices related to Alzheimers
disease and vascular dementia (2001) Acta Psychiatr Scand 104: 4-11. https://doi.org/10.1034/j.1600-0447.2001.00210.x
8. Rizzi
L, Rosset I, Roriz-Cruz M. Global Epidemiology of Dementia: Alzheimers and
Vascular Types (2014) BioMed Research International, 908915. http://dx.doi.org/10.1155/2014/908915
9. Wimo
A, Jönsson L, Bond J, Prince M, Winblad B. The worldwide economic impact of
dementia 2010 (2013) Alzheimers and Dementia 6.
10. Prince,
M., Bryce, R., Albanese, E., Wimoc, A., Ribeiro, W., & Ferri, C. P. (2014).
The global prevalence of dementia: A systematic review. Alzheimers &
Dementia, 63-75. https://doi.org/10.1016/j.jalz.2012.11.007
11. Ayushi
Gudwani PM. India Healthcare: Inspiring possibilities, Changing Journey (2012)
Mckinsey&Company.
12. Subaiya
L. Demographics of Population Ageing in India: Trends and. BKPAI Working Paper
No. 1 (2011) United Nations Population Fund (UNFPA), New Delhi, India 1-32.
13. P.M.Kulkarni
(2014) Demographic Transition in India.
14. Aiyar
S, Mody A. The Demographic Dividend: Evidence from the. IMF Working Paper
(2011) WP/11/38.
15. David
S, Jones, SH. The Burden of Disease and the Changing Task of Medicine (2012)
The New England Journal of Medicines 13569.
16. McKeown
RE. The Epidemiologic Transition: Changing Patterns of Mortality and Population
Dynamics (2009) American Journal of Lifestyle Medicine 3: 19S-26S. https://doi.org/10.1177/1559827609335350
17. Popkin
MB. An overview on the nutrition transition and its health implications: the
Bellagio meeting (2002) Public Health Nutrition 5: 93-103.
18. Wahdan
M. The epidemiological transition (1996) Eastern Mediterranean Health Journal
2: 1.
19.Prince
PM, Wimo PA. The Global Impact of Dementia An analysis of prevalence,
incidence, cost and trends. London (2015) Alzheimers Disease International
(ADI).
20. Sharma
S, Bothra M. Health Expenditure and its Repercussions on Health Status: An
Analysis of South-Asian Countries (2017) International Journal of Current
Research 9: 7.
21. Mathuranath
PS, George A, Ranjith N, Justus S, Kumar MS, et al. Incidence of Alzheimers
disease in India: A 10 years follow-up study (2012) Neurology India 60:
625-630. https://doi.org/10.4103/0028-3886.105198
22. Das
SK, Pal S, Ghosal MK. Dementia: India Scenario (2012) Neurology India 60:
618-624.
*Corresponding author:
Manisha
Bothra,Assistant Professor,
Economics and Public Policy, IILM Institute for Higher Education, New Delhi,
India, Email: manishabothra06@gmail.com
Citation:
Sharma
S, Bothra M. Changing Demographics & Dementia: A Reflection
on the Challenges Ahead for India (2018) Nursing and Health Care 2: 1-8




{kind=link}