Introduction
Deep overbite refers to the
increase of overlap of maxillary incisors to the mandibular incisors, which
also exhibits abnormal skeletal and dentoalveolar characteristics such as a
lower facial height, a deep curve of Spee, a higher
anterior teeth alveolar height and so on. While the mini-implant technique is
widely applied, it is common to use this technique to control vertical malocclusion after aligning
and leveling the upper and lower dentition [1,2]. The lingual orthodontic
appliance is also a powerful toll to treat the deep overbite.3-dimensional
evaluation showed that lingual appliance obtained significant lower incisors
intrusion [3].
Pregnancy
is quite a challenge for the patients who are undergoing orthodontic treatment,
so many researchers are investigating in the topic of patients are pregnant
during orthodontics process. In animal study, it was found that while the
number of osteoclasts was
significantly decreased during pregnancy, but pregnancy could not significantly
decrease the amount of tooth movement in the linear phase [4]. We do not
suggest patients to have orthodontic treatment when they plan
to have baby during the treatment process, but sometimes the accidental
pregnancy happen. Therefore, the orthodontist should be more carefully when
they treated this kind of patients during this special period.
Methods
and Results
Diagnosis
and Etiology
A
25-year-old woman came to us for lingual orthodontic treatment. Her main
complaint was deep overbite and lateral incisors protrusion (Figure 1). Her gum smile was obviously
when she smiled. A deep overbite of 7 mm and a serve curve of Spee (5mm) were
observed. The upper central incisors and lower incisors present a lingual
inclination. The crowding of the both maxilla and mandible arches: 2 mm (Figure 2). The periodontal disease was
severe with gum swelling and
blooding.
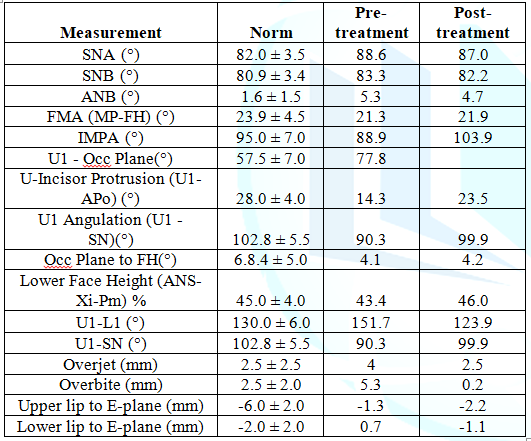
The result of cephalometric measurement that the patient was Class Ⅱ
skeletal relationship (SNA 88.6°, SNB 83.3°, ANB 5.3°)
with a protrusive maxilla, lingual declined upper incisors (U-Incisor
Protrusion 14.3°) and deep overjet 4.0 and overbite 5.3 (Table 1).
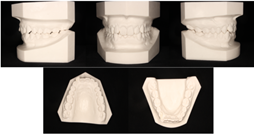
Figure 2: Pretreatment
dental casts.
Treatment
Objective
The
following treatment objectives were set;
1.
Improved
the deep overbite and obtained a natural overjet and overbite.
2.
Achieved
Class I canine and molar relationship.
3.
Alignment
of the upper and lower dentition and obtained a more health periodontal
environment which would be easier to keep clean.
4.
Improved
the smile (Figure 3).
Treatment
Alternatives
Extraction
orthodontic treatment:
while the patient’s Class Ⅱ skeletal was obviously, extraction of
upper first premolar and lower second premolar was one of the treatment
alternatives. However, the upper and lower incisors were inclined to the
lingual side and the crowding in the upper and lower dentition was slight.
Non-extraction
orthodontic treatment:
While the crowding was 2 mm in both the upper and lower dentition and the upper
and lower incisors were inclined to the lingual side, the non-extraction orthodontic
treatment
plan could be considered. What’s more, while the patient was with a skeletal
Class Ⅱ relationship between the maxillary and
mandible, but the canine and molar relationship were not so severe.

After
we discussed with the patient, the patient quiet happy to choose non-extraction
plan and she preferred to use the lingual orthodontic appliance (Figure 4).

Treatment
Progress
The
customized lingual
orthodontic appliance
Incognito was ordered from 3M Company and fabricated in German. The alignment
and leveling of the patient’s upper dentition were finished in 3 months after
the first bonding. And almost at the same time, the patient reported that she
was pregnant. So, the patient and her husband were asked to visit our
department. And we told the couple the tree alternatives which we could
offered: 1) stopped the treatment forever; 2) stopped the treatment
temporarily, debond the brackets and ordered a new bracket after the patients
delivered the baby; 3) continued the treatment and stop the treatment several
months around the period of baby delivering. (Figure 5-9).

While
the couple chooses the third alternative, and we told the predictable risks,
such as the treatment time would be prolonged, the brackets could interrupt the
special examination during the pregnancy, the brackets could be dangerous
during the baby delivering, and so on. And the patient and her husband should
take these predictable and unpredictable risks. And they signed the informed
consent which included the content discussed above. And we asked that patient
to inform the obstetrician, who was in charge to help her for baby delivering
before she had the baby that would give the doctor enough time to prepare some
special treatments for her if necessary.
One
year after the patient started orthodontic treatment, the patient stopped
treatment, rested at home and waited for baby delivery. And 19 months after
treatment, the patient visited us again, and after checked, we found that there
were only four brackets were debond by the patient during meal in period of
baby delivering. And after another 3 months fine adjustment, the patient
satisfied the result and preferred to finish the treatment and save time for
family.

Figure 6: Photographs of
post-treatment.

Figure 7: Radiographs
post-treatment: A. Cephalometric radiograph; B. Panoramic radiograph.
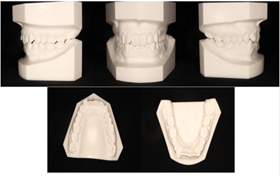
Figure 8: Post-treatment
dental casts.
Treatment
Result
All
the treatment objectives were achieved. The deep overbite was corrected, and a
natural overjet and overbite was obtained. The upper and lower dentition were
aligned and leveled. The inclined incisors were corrected. The patient’s periodontal disease was treated too.
The periodontal tissue was more health and the aligned and leveled dentition
was easier to be kept clean. The CBCT results neither showed that there was no
significantly root resorption after the treatment (Figure 6-9). The patient’s smile was improved (Figure 10).
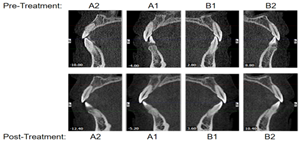
Figure 9: Complement of
incisors (A1,A2,B1,B2) pre-treatment and post-treatment.

Figure 10: The photograph
of the patient’s smile: A. pre-treatment, B. postpartum, C. post-treatment.
Comparing
the result of cephalomertic
measurement
between pre-treatment and post-treatment (Table
1, Figure 10), we could found that while the skeletal Class Ⅱrelationship
was not significantly changed but the Class Ⅰdental
relationship was achieved, the lingual inclined incisors were corrected (U1
Angulation (U1-SN) 99.9, U-Incisor Protrusion (U1-APo) 23.5), the natural
overjet and overbite was obtained (overjet 2.5 and overbite 0.2).
Figure 11: Superimposed
pre-treatment (Red) and post-treatment (Green).
Discussion
The
relationship between orthodontic treatment and pregnancy had been discussed by
some researchers. On the one hand, the pregnancy is maybe a factor to influence
adult facial changes. However, result from Bondevik O in clinical study showed
that few of the differences between adult males and females in facial changes
are caused by pregnancies [5]. On the other hand, the orthodontic is maybe a
risk element during the baby delivering. So, before we continued the
orthodontic treatment. The predictable and unpredictable risked should be
informed to the patient and her husband. And the informed consent should be
signed by the couple before the treatment continued. However, we do not suggest
patient to be pregnant during having orthodontic treatment.
While
sometimes the accidental pregnancy happens, there are several options to deal
with this situation. And when the patient and her husband choose the option to
have the continue orthodontic treatment. The patient and the obstetrician, who
was in charge to help her for baby delivering, should be informed the
predictable risks and unpredictable risks by the orthodontist. All of these
were what we can do to help the patient to reduce the risks she will face. And
all of these will give the doctor enough time to prepare some special
treatments for her if necessary.
The
tree categories following should be the reasons for that lingual bracket
orthodontic is difficult: 1) Biomechanical issues; 2) Bracket design choices/constraints;
and 3) Lingual anatomy. On the one
hand, for the biomechanical issues, the orthodontist should keep on studying to
expand our knowledge and change our mind. On the other hand, for the bracket
design choices, and lingual anatomy, the faster development of science and
technology had offered new method to deal with them. For example, the
Computer-Aided Designed and Manufactured (CAD/CAM) technique could produce
customized wires the customized lingual bracket systems, which will overcome
the brackets and anatomy problem [6-8]. And the efficacy and efficiency of
CAD/CAM customized lingual bracket systems was outstanding [7].
For the patient in this study, the lingual customized lingual bracket system
was quite efficient in treating the deep overbite. And while the patient had to
eat a lot of food around the baby delivering and milking the baby that we could
find from the weight the patient had put on, but there only four brackets were
debond in half a year. This was due to the powerful bonding and positive lock
system of customized lingual orthodontic appliance.
There
were several methods for orthodontic vertical control such as mini-implants and
Forsus appliance [1,9]. The
lingual brackets system is powerful in controlling horizontal problems however
it is also efficient in vertical problem [10,11]. The Class Ⅱ
malocclusion with complex problems was treated with lingual orthodontic
brackets system in an efficiently way. Although the initial malocclusion and
periodontal conditions were unfavorable for the adult patients, it was reported
that after orthodontic treatment periodontal changes in adult patients were
like those in young adults [12]. In this study, the patient’s periodontal
disease was treated, and she not only obtained the health periodontal tissue (Figures 6-9, 11), but also had an
esthetic smile and the self-confidence (Figure
11).
Conclusion
Lingual
orthodontic appliance is one of the powerful tools to treat the deep over bite.
Orthodontics and obstetrician
should pay more attention to the patient who was pregnant and only in this way
can we reduce the risks the patient will face.
Acknowledgment
This research was supported by the National
Natural Science Foundation of China (31400808, 81570979 and 21402018). And it
is also supported by Natural Science Foundation Project of Chongqing
(CSTS2015JCYJA10039). This study is also supported by the Science and
Technology Research Project of Chongqing Municipal Education Commission of
China (KJ1600226) and Program for Innovation Team Building at Institutions of Higher
Education in Chongqing in 2016 (CXTDG201602006).
References
1.
Jung
MH. Vertical control of a Class II deep bite malocclusion with the use of
orthodontic mini-implants (2019) Am J Orthod Dentofacial Orthop 155: 264-275. https://doi.org/10.1016/j.ajodo.2018.08.016
2.
Krishnaswamy
NR. Vertical control with TADs: Procedures and protocols (2018) Seminars in
Orthodontics 24: 108-122.
https://doi.org/10.1053/j.sodo.2018.01.010
3.
Chardey
EK, Fastuca R, Beretta M, Di Blasio A, Vercellini N, et al. Digital Dynamic 3D
Monitoring of Lower Incisors Intrusion in Lingual Orthodontics. open dent J
2018 12: 104-117. http://dx.doi.org/10.2174/1874210601812010104
4.
Ghajar
K, Olyaee P, Mirzakouchaki B, Ghahremani L, Garjani A, et al. The effect of
pregnancy on orthodontic tooth movement in rats (2013) Med oral, patol oral cir
bucal 18: 351-355. https://dx.doi.org/10.4317%2Fmedoral.18465
5.
Bondevik
O. Does pregnancy or use of contraceptives influence adult facial changes?
(2010) J orofac orthop 71: 32-39. https://doi.org/10.1007/s00056-010-0816-z
6.
Nguyen
T and Jackson T. 3D technologies for precision in orthodontics (2018) Seminars
in Orthodontics 24: 386-392. https://doi.org/10.1053/j.sodo.2018.10.003
7.
Awad
MG, Ellouze S, Ashley S, Vaid N, Makki L, et al. Accuracy of digital
predictions with CAD/CAM labial and lingual appliances: A retrospective cohort
study (2018) Seminars in Orthodontics 24: 393-406. https://doi.org/10.1053/j.sodo.2018.10.004
8.
Jost-Brinkmann
PG, Bartels A, Gunawan A and Böhme A. CAD/CAM in lingual orthodontics (2001)
International Congress Series 1230: 1287-1288. http://dx.doi.org/10.1155/2014/164164
9.
Bayram
M. Combined orthodontic-orthopedic treatment of an adolescent Class II Division
2 patient with extreme deepbite using the Forsus Fatigue Resistant Device
(2017) Am J Orthod Dentofacial Orthop 152: 389-401. https://doi.org/10.1016/j.ajodo.2016.07.023
10.
Wang
X-D, Lei F-f, Liu D-W, Zhang J-N, Liu W-t, et al. Miniscrew-assisted customized
lingual appliances for predictable treatment of skeletal Class II malocclusion
with severe deep overbite and overjet (2017) J Orthod Dentofacial Orthop 152: 104-115.
https://doi.org/10.1016/j.ajodo.2016.06.053
11.
Yanagita
T, Nakamura M, Kawanabe N and Yamashiro T. Class II malocclusion with complex
problems treated with a novel combination of lingual orthodontic appliances and
lingual arches (2014) J Orthod Dentofacial Orthop 146: 98-107. https://doi.org/10.1016/j.ajodo.2013.08.022
12.
Han
J, Hwang S, Nguyen T, Proffit WR, Soma K, et al. Periodontal and root changes
after orthodontic treatment in middle-aged adults are similar to those in young
adults (2019) J Orthod Dentofacial Orthop 155: 650-655. https://doi.org/10.1016/j.ajodo.2018.05.027
*Corresponding author
Xiaomian Wu, Chongqing
Key Laboratory of Oral Diseases and Biomedical Sciences, College of
Stomatology, Chongqing, Medical University, Chongqing, China, E-mail: wuxiaomian@hospital.cqmu.edu.cn
, wuxiaomian898@163.com
Citation
Hu X and Wu X.
Treatment of the deep overbite malocclusion with lingual orthodontic appliance
during the patient was pregnant (2019) Dental Res Manag 3: 24-27



