

Ameloblastoma is a common odontogenic tumor with the potential of local invasion and recurrences. Moreover, it has a variable presentation and many challenges surrounding the management of the condition [1]. From public health perspectives through to molecular aetiopathogenesis it paints the portrait of heterogeneity and complexity [2-4]. For example, gender and age distribution, presenting complaints, the clinical record keeping scenarios in developing countries compared to the developed countries, the aggressive potential for local invasion, possibility for malignant transformation etc. Moreover, choosing the optimal mode of management (radical vs conservative surgery) poses a dilemma to the clinician. Findings of retrospective studies on de-identified case notes retrieved for varying follow-up periods provides the major source of scientific evidence on management of ameloblastoma.
We studied randomly selected clinical records retrieved, for clinically diagnosed odontogenic tumors that were histopathologically confirmed as ameloblastoma among selected public Oral and Maxillofacial Units in the Western Province of Sri Lanka. This descriptive analysis was based 35-cases of ameloblastoma reported from 2011 to 2018.
According to age of patients, the mean age was 40.03 ± 19.12 years ranging 12-82 years. These findings were in agreement with similar studies revealing 4th decade of life as the predominant age of presentation despite having a wide variation. As shown in Table 1, ameloblastoma could affect adolescent, younger and older age groups but the highest burden is carried by economically productive age group. Moreover, the gender ratio of males to females was 1:1.05 which was in agreement as well as disagreement with other studies conducted elsewhere [2,3].
Painless swelling of the face was the presenting complaint of half of the cases while another 22.9% cases had additional symptoms accompanied with it. In contrast, some other studies reported pain and tumor formation as presenting status [2]. Moreover, in developing country context dominated by problem based health care visits, ameloblastoma could commonly present at late stages of the advanced disease especially when the swelling is painless. This was corroborated with the finding as the majority (28.6%) had tumor length >5 cm.
The histological type of ameloblastoma influences the management of the condition and the follicular type was the dominant in accordance with other studies. There were 2 cases of ameloblastic carcinomas and notably 25.7% were reported as ameloblastoma without histological subtype. As shown in the results, of a majority of clinical records the basic information such as size, texture, radiological findings were missing as 48.6%, 54.3% and 62.9% respectively.
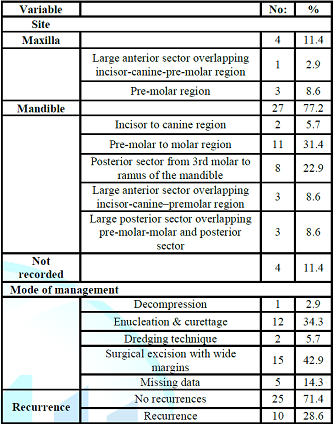
As shown in Table 2, the mandible was the predominantly affected jaw (77.2%) with pre-molar to molar sub-site (31.4%). These findings were in agreement with similar studies [2,3]. According to the mode of management, the majority 42.9% were managed by surgical excision with wide margins and another 34.3% was managed by enucleation and curettage. Another 5.7% were management by dredging technique which is a conservative mode of management of ameloblastoma among young patients. Moreover, 28.6% of cases were recurrent cases but the data on the follow up period was not available [5].
In
conclusion, present retrospective case-series analysis revealed the potential
impact of painless swellings and missing information with regard to ameloblastoma cases in a developing
country context. This could hamper the early detection and the need for long
term follow up due to the biological behavior of the tumor. Moreover, many
deficiencies in maintaining comprehensive, retrievable patient data bases on
conditions like Ameloblastoma are lacking in developing country contexts with
many constraints and overcrowded public health care settings. Hence,
urgent corrective measures are warranted in this regard in order to improve the
existing status.
For Table 1 and 2 click the below links
References
1. Effiom OA, Ogudana OM, Akinshipo AO and Akinotype SO. Ameloblastoma: current etiopathological concept and management (2018) Oral Dis 24: 307-316. https://doi.org/10.1111/odi.12646
2. Moraes FB, Cardoso RMN, Rodrigues SV, Dutra MVF, Pereira UR, et al. Ameloblastoma: a clinical and therapeutic analysis of six cases (2014) Rev Bras Ortop 49: 305-308. https://dx.doi.org/10.1016%2Fj.rboe.2014.04.006
3. Fregani ER, da Cruz Perez DE, de Almeida OP, Kowalski LP, Soares FA, et al. Clinicopathological study and treatment outcomes of 121 cases of Ameloblastomas (2010) Int J Oral Maxillofac Surg 39: 145-149. https://doi.org/10.1016/j.ijom.2009.11.022
4. Chukwuneke FN, Anyanechi CE, Akpeh JO, Chukwuka A, and Ekwueme OC. Clinical characteristics and presentation of ameloblastomas: an 8-year retrospective study of 240 cases in Eastern Nigeria (2015) Br J Oral Maxillofac Surg 54: 384-387. https://doi.org/10.1016/j.bjoms.2015.08.264
5. Laborde A, Nicot R, Wojcik T, Ferri J and Raoul G. Ameloblastoma of the jaws: Management and recurrence rate (2017) Eur Ann Otorhinolaryngol Head Neck Dis 134: 7-11. https://doi.org/10.1016/j.anorl.2016.09.004
*Corresponding author
Irosha Perera, Preventive Oral Health Unit, National Dental Hospital (Teaching), Colombo, Sri Lanka, E-mail: irosha_rukmali@yahoo.com
Citation
Chandima S, Perera I, Gunathilake S, Shanmuganathan S and Silva D. The profile of ameloblastoma and the status of routine clinical records from a developing country context (2019) Dental Res Manag 3: 45-46

{kind=link}
{kind=link}