The purpose of this article is to provide podiatric physicians with the strategies for identifying, assessing and responding to patients who may have changes in opioid pharmacokinetics and pharmacodynamics due to sex and age differences and disease states. First of all, possible opioid drug interactions that exist within the context of patient demographics and disease states are presented and described. Secondly, both pharmacokinetic and pharmacodynamics changes of opioid agents within certain patient demographics are presented. Lastly, the art of clinical coping mechanism to prescribe opioids to patients that may be elderly or presenting with disease states that may alter opioid pharmacokinetics.
Introduction
Physicians
during their role of patient pain management frequently prescribe opioids.
Clinicians have an ethical obligation to prescribe responsibly yet cautiously
to diminish the potential for opioid diversion and help minimize the growth of
the current epidemic of opioid abuse. Analgesic opioid therapy has been the
cornerstone of pharmacotherapeutic management of acute and chronic pain.
Ideally, opioid analgesics are prescribed by balancing beneficial and adverse
effects. Further, the foot and ankle specialist must remember that comfort is
the ultimate goal when using any medication, including opioids, to manage pain
[1,2]. Opioid selections are based on patient specific factors such as age,
renal function, and sex differences.
The use
of an opioid agent requires a practitioner to be comfortable with their use,
especially in the presence of both either demographic or disease states like
age, obesity, diabetes mellitus, kidney disease, congestive heart disease, and
sex differences. Clinicians have been directed to select immediate-release
opioid formulations over extended-release or long-acting opioids because they
are safer, regardless of whether the drug is used for acute or long-term
treatment.
Due to a
medication’s pharmacodynamics and pharmacokinetic profile or a patient’s
response to an opioid agent, no single opioid analgesic product may be a
perfect choice for a clinician to rely on, in order to treat all types of pain.
Although no opioid seems to be superior in relieving pain, certain products are
clearly inferior because of increased risks of toxic effects [1-3]. Opioid
pharmacologic regimens must be individualized based on subjective, objective,
and clinical findings. As part of opioid stewardship, this review highlights and
describes opioid pharmacodynamic and pharmacokinetic especially in the presence
of disease states like diabetes mellitus, kidney disease, congestive heart
disease, and sex differences to assist and empower the podiatric physician to
prescribe an opioid agent for maximizing opioid analgesic effects and decrease
opioid possible adverse effects.
First of
all, alterations in pharmacokinetics and pharmacodynamics due to age,
illnesses, and sex will be presented as a foundation. Second, building on these
clinical alterations in pharmacokinetics and pharmacodynamics that will be
applied, and opioid pharmacology will be presented. Finally, methods of
clinical coping centered on opioid prescribing will be applied to patients who
may present with alterations in pharmacokinetics secondary to age, illness, or
sex.
Pharmacokinetic Changes
Given,
the change in physiological, pharmacological, and psychological aspects of the
aging adult of the symptom of pain in the elderly population is especially
difficult to treat. Opiates and opioids are the mainstay of pain treatment
throughout all age groups, but special attention must be paid to the efficacy
and side effects of these powerful drugs when prescribing to a population with
impaired metabolism, excretion, and physical reserve [4]. As a patient becomes
elderly, important age-related changes might alter opioid drug pharmacokinetics
and result in unwanted side effects.
The
process aging is characterized by structural and functional changes affecting
all organ systems, which results in reduced homeostatic capacity over time.
Although the function of a particular system may be maintained during resting
conditions, the reduction of functional reserve is responsible for an increased
vulnerability to stress [5]. Changes in body composition and that in hepatic
and renal function are responsible for an increase in the volume of
distribution of lipid-soluble drugs and reduced clearance of lipid-soluble and
water-soluble drugs. All these changes lead to a prolong plasma elimination
half-life, leading to greater drug plasma levels. Moreover, significant
pharmacodynamics changes occur that cause an increased sensitivity to many
drugs. Finally, a reduced body functional reserve itself also leads to an
increase in sensitivity by impairing homeostatic compensatory mechanisms [5].
Opioids
are highly varied and generally thought to possess similar pharmacokinetic
activity. Opioids are rapidly absorbed in the gut, have high rate of first pass
in the liver, are conjugated in the liver, have metabolites, and vary in
distribution based on their differing protein affinity, and then they are
excreted via bile to feces or via kidneys. Opioid pharmacodynamics effects are
complex and depend upon poorly measured variables such as receptor function and
intracellular response, which can alter drug action. Pharmacokinetic actions of
drug absorption, distribution, and elimination are more measurable [5,6].
As a
patient ages, the rate at which certain drugs are absorbed can be altered in
adults because of a decrease in gastrointestinal transit time and increase
gastric pH secondary to the use of proton pump inhibitors, H2 receptor
antagonists, or antacids to treat age related gastrointestinal aliments. With
aging, there are changes in body composition, such as increase in adipose
tissue, decrease in lean body mass, and decrease in total body water. These
changes can affect drug distribution. Therefore, lipophilic drugs tend to have
greater volume of distribution and can take more time to be eliminated from the
body. Aging can also bring reduction in hepatic blood flow and volume, which
can decrease metabolism of drugs [5-8].
Additional
impairments in drug metabolism can occur with impaired Phase I reactions, which
include oxidation, hydroxylation, and dealkylation. This can specifically
reduce the first pass effect of opiates in the elderly. Elimination of drugs
can be altered with age-related reductions in renal blood flow and Glomerular
Filtration Rate (GFR). For opiates that have primary renal clearance, such as
morphine and hydromorphone, decreases in GFR lead to more side effects [5-9].
Obesity
which has been identified to be a clinical trait of Type 2 diabetes mellitus
affects all four aspects of pharmacokinetics. For example, when a clinician
utilizes weight-based dosing they must accept that a drug’s fate is based on
total body weight that may be affected by obesity resulting in under dosing or
overdosing patients, depending on the characteristics of the drug. The
pharmacodynamics profile of drugs may also be affected, e.g. the risk of
respiratory depression and loss of airway patency is greater with sedatives and
narcotics. Careful therapeutic drug monitoring is important in obese patients.
Morbidly obese people are often excluded from clinical trials during the drug
development process, so data is limited on the correct dosing of many drugs.
Therefore
using clinical judgment, combined with interpretation of drug pharmacokinetics
is often required by the clinician when they prescribe a medication. Obesity
causes increased absorption of oral medications, increased gastric emptying and
a decreased subcutaneous absorption is due to poor subcutaneous blood supply.
Decreased subcutaneous absorption is due to poor subcutaneous blood supply.
Intramuscular administration may fail if needles are too short to pierce the
skin. Opioid distribution is markedly affected by ratio of adipose tissue to
lean body mass if a drug has high lipid solubility then its volume and
distribution will result in an accumulation in fat stores [10]. Literature
outlining the research between medication fates within the disease process of
Diabetes Mellitus is cited below. Diabetes mellitus has been found to affect
protein, lipid, and carbohydrate metabolism, and the biochemical pathways that
are involved in drug biotransformation. Four principles of pharmacokinetics
that may be influenced by diabetes mellitus include absorption, distribution,
biotransformation, and excretion. Diabetic changes in subcutaneous and muscle
blood flow, and delayed gastric emptying may influence the way a drug is
absorbed [11-16].
Non-enzymatic
glycation of albumin secondary to diabetes mellitus may affect a medication’s
distribution within the body. Gastric emptying is frequently abnormal in
patients with long-standing type 1 and type 2 diabetes mellitus. Symptoms
commonly associated with delayed gastric emptying include nausea, vomiting,
bloating, and epigastric pain. These patients are also at risk of malnutrition,
weight loss, impaired drug absorption, disordered glycemic control, and having
a poor quality of life. It although many studies have reported
diabetes-mediated changes in gastric emptying time, the magnitude of the delay
is modest, and at this time, some authors may not consider it clinically
important [11-13].
Drug
metabolism is enzyme-mediated structural modification to a drug that changes
its biological activity and/or water solubility. These enzymatic reactions
result in metabolites that may be active or rendered inactive. The
gastrointestinal wall, lungs, liver, and blood possess enzymes that metabolize
drugs. Drug metabolism by the liver occurs through one or both
biotransformation reactions classified as either Phase I or Phase II reactions.
Building on the assertion centered on the direct relationship between diabetes
mellitus and obesity, the effect of obesity on cytochrome P450 appears to be
isozyme-specific with the activity of cytochrome P450 3A4 decreasing. The
clearance of Cytochrome P450 (CYP) 3A4 substrates is lower in obese patients in
comparison with non-obese patients [14-16].
Conversely,
researchers saw trends indicating higher clearance values via the following
Cytochrome P450 isoenzymes: CYP1A2, CYP2C9, CYP2C19 and CYP2D6.16 Opioid
drug-drug interactions are presented to assists clinicians to prevent drug harm
and drug misadventure in obese and diabetic patients in Table 1.
There
are complex interactions within the body’s neuro-endocrine systems in response
to opioids include alterations in the autonomic nervous system (sympathetic and
parasympathetic nervous system), the renin-angiotensin-aldosterone system and
anti-diuretic hormone. In addition, other mechanisms are also involved,
including dehydration, rhabdomyolysis, and urinary retention. Changes in the
sympathetic and parasympathetic nervous systems affect the kidney by altering
renal blood flow and glomerular filtration rate.
These
changes occur at several levels including the heart and kidney. Usually the
autonomic nervous system controls vital body functions with the sympathetic and
parasympathetic innervation acting antagonistically based on need. In the
cardiovascular system, the Sympathetic Nervous System (SNS) increases heart
rate and myocardial contractility as well as raises peripheral vascular
resistance and arterial blood pressure via vasoconstriction [17].
In
chronic kidney diseases, there is an increase in morphine in the mean peak concentration
and the area under the concentration-time curve for both active and principle
metabolites. With chronic kidney diseases, the metabolites of merperidine are
present for longer, can decrease the seizure threshold, and should be avoided
for chronic use. Extended effects of codeine and dihydrocodeine with chronic
kidney disease have been reported. Specific drug pharmacokinetics and
pharmacodynamics may differ between men and women. [18] Soldin and Mattison
report that reviews of the Food and Drug Administration’s Adverse Events
Reporting System (AERS) suggest that women experience more drug-related adverse
events, and often these adverse events are described as more serious.
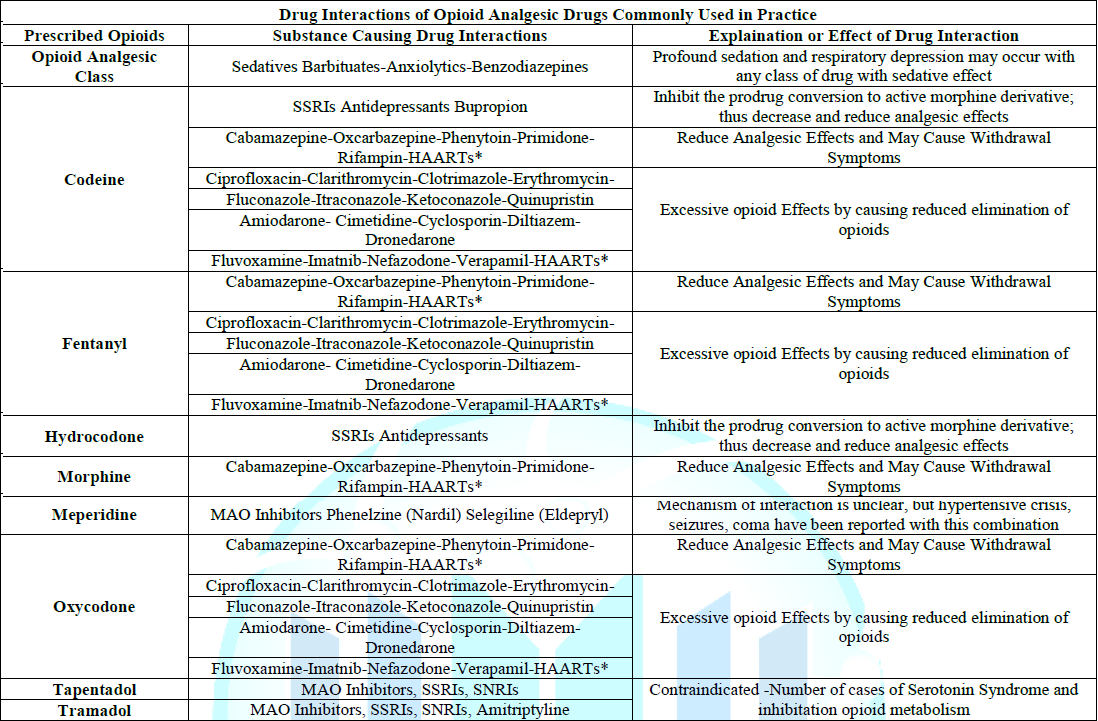
Table 1: Drug Interactions of Opioid
Analgesic Drugs Commonly Used in Practice.
Physiological
differences between males and females have been observed in plasma volume, body
mass index, plasma proteins, body fat, cardiac output, liver blood flow, and
hepatic enzyme activity, thus influencing the Hepatic clearance of drugs.
Further,
there are known sex differences with all three major renal functions:
glomerular filtration, tubular secretion, and tubular reabsorption [17,18].
Morphine has long been considered the gold standard of opioid agents [19].
Morphine has been shown to be more potent and exhibiting a slower onset and
offset in women [20,21]. It has been established that women perceive more pain
and require greater dosages of morphine to achieve the same antinociceptive
effect as in men [21-23].
Offer an
explanation for this as higher mu-receptor binding in various cortical and
subcortical brain regions exhibited in women than in men, which reveal that
women appear to be more sensitive to pain and are more vulnerable to chronic,
widespread, and post-procedural pain conditions [24]. Finally, Averitt et al.
present evidence that demonstrates a neural basis implicating sex differences
in opioid metabolism and neuroimmune signaling with a focus on the
periaqueductal gray as a sexual dimorphic core of descending opioid-induced
inhibition. They summarize the data to state that both preclinical and clinical
research indicate that opioids are less effective in females to explain why
women are more likely to be prescribed opioids at higher doses and for longer
periods of time than men [25].
Clinical Coping and Opioid Dosing
In the
context of opioid stewardship, clinical coping is expending conscious effort to
solve potential opioid dosing problems due to the Impact of presenting
demographics and disease states that may cause opioid adverse effects, opioid
misuse, or opioid abuse disorder, thus seeking to master, minimize, or tolerate
these possible issues or conflicts. The effectiveness of this clinical coping
efforts depends on the type of opioid issue and/or conflict, the particular
individual, and the particular circumstances. Clinical coping suggestions with
regard to dosing opioids in the context of demographics and disease states is
summarized and presented in Table 2.
In the
management of chronic pain in the elderly, physicians should consider a
multimodal therapy approach to include nonpharmacologic therapy and non-opioid
pharmacologic therapy before initiating opioids [26]. Opioid use should be
implemented only when alleviation of pain and improvement of function outweigh
the risks to the patient. When selecting non-opioid pharmacologic therapies
that may include antidepressants, antiarrhythmic, anticonvulsants,
tranquilizers and regional anesthesia, the provider should be aware of the
possibility of both drug-drug interactions as well as patient demographic
interactions that may result with co-administration of these agents. As always,
goals of chronic pain therapy in the elderly are to decrease pain, increase
function, and improve overall quality of life. It is recommended that opioids
be prescribed at the lowest effective dose, which is approximately 25% to 50%
of the starting dose recommended for adult, and then it must be slowly titrated
to minimize adverse effects for patients older than age 70 years.The dosage
should be reassessed one to four weeks after initiation or dose escalation.
Immediate-release formulations of opioids should be initiated before
extended-release or long-acting opioids are attempted [27].
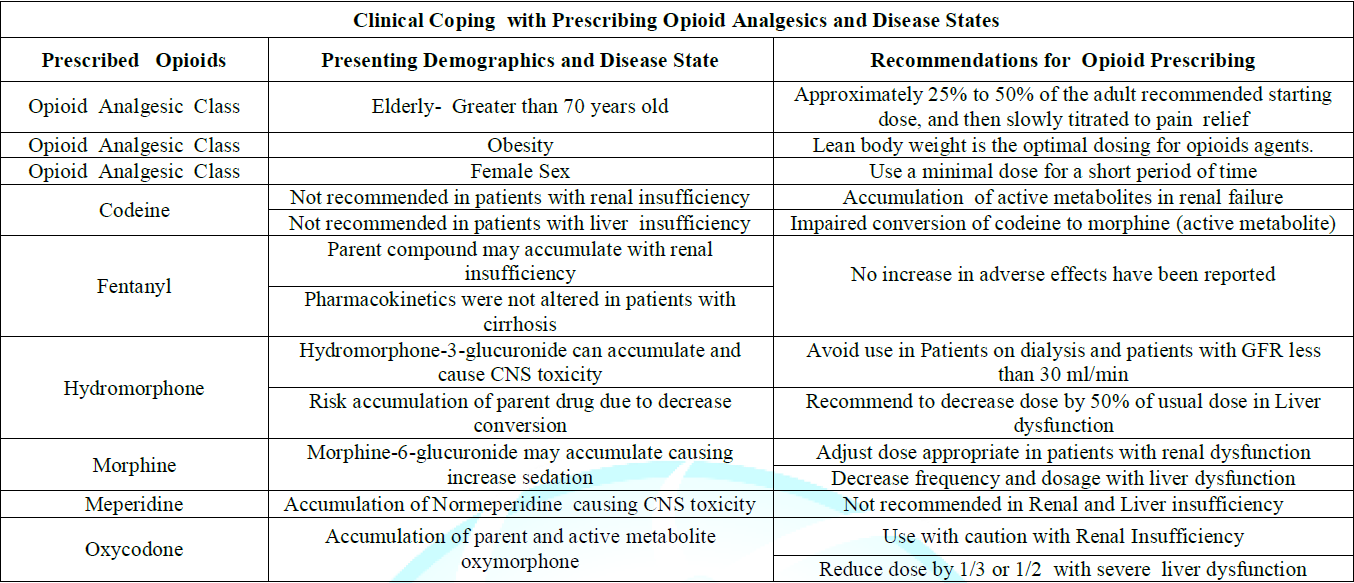
Table 2: Clinical Coping with Prescribing
Opioid Analgesics and Disease States.
At the
time clinicians prescribe opioids to patients with renal or hepatic dysfunction
receive opioid analgesics, it is essential to understand and consider how
opioid pharmacokinetics can be altered. This is necessary to ensure appropriate
pain relief for the patient while limiting serious and potentially preventable
adverse effects, such as respiratory depression, hypotension, or central
nervous system toxicity from either the parent drug or its metabolites.
Patients
with severe liver disease should be prescribed lower doses of opioids, with
extended dosing intervals when multiple daily doses of opioids are needed to
relieve pain. Opioids should be used cautiously in patients with severe renal
and hepatic dysfunction because of the possible accumulation of the parent drug
and/or metabolites.
Usual or
adjusted doses may be appropriate for patients prescribed morphine,
hydromorphone, and hydrocodone. Oxycodone should not be used in hemodialysis
patients, and codeine and meperidine should be avoided at all times. Methadone
and fentanyl can be carefully used in patients with renal dysfunction or on
dialysis, and methadone is not advised in severe liver failure. For most patients
with renal or hepatic dysfunction, either morphine or hydromorphone should be
the opioid agents prescribed.
Awareness
of the pharmacology of the commonly used opioids is necessary for safe and
effective care of morbidly obese patients. Changes in cardiac output and
alterations in body composition affect the distribution of numerous opioid
drugs. The physician should use a patient’s lean body weight is the most
optimal method to dose opioids agents. The increased incidence of obstructive
sleep apnea and fat deposition in the pharynx and chest wall places the
morbidly obese at increased risk for adverse respiratory events secondary to
opioid agents, thus altering the pharmacokinetic and pharmcodynamic properties
of opioid agents [10].
Acute
pain may often be managed with non-opioid medication. If opioids are used,
prescribe the lowest dose for the shortest duration and avoid prescribing
refills to reduce the risk for dependency. Literature sources have found that
greater use and misuse of prescription medications among older women may be
connected to the loss of a partner, low income, mental health issues, or poor
overall health. Clinical recommendations for prescribing opioids to women of
child-bearing age include the following: assess pregnancy risk in all women of
childbearing age prior to prescribing an opioid, avoid prescribing opioids to
pregnant women and educate pregnant women about the known risks of opioids to
both the mother and the fetus. If opioids must be prescribed to a pregnant
woman for acute pain, prescribe the lowest dose and duration appropriate.
Provide proper pain control and education to lactating women experiencing acute
pain following birth and surgical procedures to avoid opioid adverse effects to
the mother and the child [28,29].
A
multi-level collaborative health care team approach using an Opioid Stewardship
Program (OSP) can provide the necessary frame work to change the current opioid
analgesic culture and practice. An OSP can address opioid prescribing,
treatment for opioid use disorder, use both educational initiatives and
information technology to assist with appropriate opioid prescribing and thus
be a helpful tool to curtail the opioid crisis. The acronym “MORPHINE” will be
introduced and defined to assist clinicians to appreciate OSPs. The word
morphine was selected as an acronym because of its historical significance.
Morphine has long been considered the “gold standard” when it comes to pain
relief [30-32].
“M” is for multimodal analgesic
strategies. A multimodal analgesic approach is likely to produce superior
analgesia over the use of an opioid based approach because multimodal analgesic
agents target a variety of pain pathways [31-33]. Multimodal analgesic agents
target a variety of pain pathways. Many non-opioid multimodal agents to
include: heat, ice, massage, physical therapy benefit patients by resulting
lower consumption of opioids. It should be acknowledged that opioid medications
may provide some measure of relief, but opioids are associated with the health
risks of both weight gain and altered glycemic regulation. Further, the use of
opioids in a diabetic patient can influence their ability to monitor and
control their diabetes by altering their perceptions of activities of daily
living to include eating habits, making it more difficult to control your blood
glucose levels and the ability to manage your diabetes.
“O” is for the development of an
opioid formulary. An opioid formulary identifies those opioids that offer the
greatest benefit to a geriatric patient while minimizing risks. Important
considerations for objective opioid selection included drug efficiency, safety,
patient acceptability, and cost. OSPs can limit opioid initiation by creating
prescribing guidelines for providers specializing in treating older patients.
Both morphine or fentanyl may be the opioid of choice for an obese or a
diabetic patient with careful monitoring. There is always a risk of
accumulation of the metabolite of morphine in renal insufficiency [32,33].
“R” is for risk reduction from
opioid harm. Therapeutic success depends on proper candidate selection,
assessment before administration of opioid therapy, and close patient
monitoring. Beyond taking a good medical history via an effective patient
interview, there are several risk assessment tools available in OSPs to help
identify patients who may be at risk. The clinician should appreciate how the
sedative opioid adverse effects may potentiate a sedentary life style that may
affect patients with wounds that are potentiated by pressure if a patient
cannot off weight them as part of their treatment regimen.
“P” is for pharmacokinetics and
pharmacodynamics of opioids. All opioids are metabolized by the liver with age
related reduction in CYP3A4 function that affects opioids [34]. Providers must
be aware of dangerous combinations of medications, Over-the-counter (OTC)
products, and herbal supplements to avoid deadly drug-drug interactions with
opioids. Avoid concurrent opioids and benzodiazepines whenever possible [35].
“H” is for help. Pain management
specialists can empower a patient’s ability to function and improve their
quality of life. Patients who present with complex comorbid pathophysiology as
well as multiple drug regimens provide an individual complex challenge for
staff and administrators attempting to provide safe and high-quality care for
older adults with substance use disorders. Patients with substance use
disorders with medically legitimate pain sufficient to justify opioids must be
closely monitored [32-33].
“I” is for use of information
technology. OSPs can influence electronic records to provide oversight adhering
to regulatory changes and evolving state laws that influence prescribing,
mandatory prescription drug monitoring program queries, consent for minors for
opioid use, and prompts for the initiation of control substance agreements
[32].
“N” is for the number of Morphine
Milligram Equivalents (MME). Ideally, OSPs can assist geriatric providers to
prescribe lower mme amounts to patients by using data collected stored by
information technology. Prescribe the lowest effective dosage, carefully
reassess benefits and risks when considering increasing dosage to 50 morphine
milligram equivalents or more per day [32-34].
“E” is for education to medical
professionals, patients, and patient caregivers. It is paramount that an open
dialog can be fostered so that expectations of opioid therapy can be
appreciated by all parties.31-32 Opioid stewardship principles should become a
priority with all opioid prescribers.
Conclusions
Opioid
stewardship requires the podiatric physician to acknowledge that opioid
pharmacodynamics and pharmacokinetic parameters may be altered in the presence
of the following age or disease states: diabetes mellitus, kidney disease,
obesity, and sex differences that may impact opioid’s beneficial and possible
adverse effects. As a foundation, alterations in opioid pharmacokinetics and
pharmacodynamics due to age, illnesses, and sex differences were presented.
Second,
building on these clinical alterations in pharmacokinetics and pharmacodynamics
were applied to opioid pharmacology to describe possible adverse effects.
Finally, methods of clinical coping centered on opioid prescribing were
presented and applied to patients who may present with alterations in
pharmacokinetics secondary to age, illness, or sex.
References
1. Smith
RG. Opioid prescribing: podiatric implications (2018) Podiatry Management 37: 161-169.
2.
Smith
RG. A review of opioid analgesics frequently prescribed by podiatric physicians
(2006) J Am Podiatr Med Assoc 96: 367-373. https://doi.org/10.7547/0960367
3.
Campomizzi
ME. Pharmacologic management of acute pain: the basics (2004) Pharmacy Practice
News 31.
4.
Chau
DL, Walker V, Pai L and Cho LM. Opiates and elderly: Use and side effects
(2008) Clin Interv Aging 3: 273-278.
5.
Mangoni
AA and Jackson SHD. Age-related changes in pharmacokinetics and
pharmacodynamics: basic principles and practical applications (2003) Br J Clin
Pharmacol 57: 6-14. https://doi.org/10.1046/j.1365-2125.2003.02007.x
6.
Hughes
SG. Prescribing for the elderly patient: why do we need to exercise caution?
(1998) Br J Clin Pharmacol 46: 531-533. https://doi.org/10.1046/j.1365-2125.1998.00842.x
7.
Linnebur
SA, O’Connell MB, Wessell AM, McCord AD, Kennedy DH, et al. Pharmacy practice,
research, education, and advocacy for older adults (2005) Pharmacotherapy 25: 1404-1405.
8.
Tegeder
I, Lötsch J and Geisslinger G. Pharmacokinetics of opioids in liver disease
(1993) Clin Pharmacokinet. 37: 17-40. https://doi.org/10.2165/00003088-199937010-00002
9.
Davies
G, Kingswood C and Street M. Pharmacokinetics of opioids in renal dysfunction
(1996) Clin Pharmacokinet 31: 410-422. https://doi.org/10.2165/00003088-199631060-00002
10.
Ingrande
J and Lemmens HJ. Dose adjustment of anaesthetics in the morbidly obese (2010)
Br J Anaesth 105: 6-23. https://doi.org/10.1093/bja/aeq312
11.
Dostalek
M, Akhlaghi F and Puzanovova M. Effect of diabetes mellitus on pharmacokinetic
and pharmacodynamic properties of drugs (2012) Clin Pharmacokinet 51: 481-499. https://doi.org/10.1007/bf03261926
12.
Gwilt
PR, Nahhas RR and Tracewell WG. The effects of diabetes mellitus on
pharmacokinetics and pharmacodynamics in humans (1991) Clin Pharmacokinet 20: 447-490.
https://doi.org/10.2165/00003088-199120060-00004
13.
Ma
J, Rayner CK, Jones KL and Horowitz M. Diabetic gastroparesis diagnosis and
management (2009) Drugs 69: 971-986. https://doi.org/10.2165/00003495-200969080-00003
14.
Benet
LZ, Kroetz DL and Sheiner LB. Pharmacokinetics: The dynamics of drug
absorption, distribution, and elimination. Hardman JG, Limbird LE (Eds.) (1996)
Goodman and Gilman’s The Pharmacological Basis of Therapeutics, McGraw Hill,
New York pp. 3-27.
15.
Hansten
PD and Horn JR. Drug interaction mechanisms: enzyme induction. In: Hansten and
Horn’s Drug Interactions Analysis and Management. Facts and Comparison (2003)
St. Louis pp. PM1-PM15.
16.
Bauer
LA. Clinical Pharmacokinetics and pharmacodynamics. Dipro JT (Ed)
Pharmacotherapy: A Pathophysiologic Approach (1999) Appleton and Lange, Stamford,
USA pp. 21-30.
17.
Mallappallil
M, Sabu J, Friedman EA and Salifu M. What Do We Know about Opioids and the
Kidney? (2017) Int J Mol Sci J 18: 223. https://doi.org/10.3390/ijms18010223
18.
Soldin
OP and Mattison DR. Sex differences in pharmacokinetics and pharmacodynamics (2009)
Clin Pharmacokinet 48: 143-157. https://doi.org/10.2165/00003088-200948030-00001
19.
Smith
RG. Using clinical-based evidence as the sextant to prescribe and navigate
through the opioid crisis (2018) Foot Ankle Quarterly 29: 143-157.
20.
Soldin
OP, Chung SH and Mattison DR. Sex differences in drug disposition (2011) J
Biomed and Biotech 2011: 1-14. https://doi.org/10.1155/2011/187103
21.
Sarton
E, Olofsen, Romberg R, Hartigh J, Kest B, et al. Sex differences in morphine
analgesia: An experimental study in healthy volunteers (2000) Anesthesiology
93: 1245-1254. https://doi.org/10.1097/00000542-200011000-00018
22.
Pieretti
S, Di Giannuario A, Di Giovannandrea R, Marzoli F, Piccaro G, et al. Gender differences
in pain and its relief (2016) Ann Ist Super Sanita 52: 184-189.
23.
Craft
RM. Modulation of pain by estrogens (2007) Pain 132: 3-12. https://doi.org/10.1016/j.pain.2007.09.028
24.
Fillingim
RB, King CD, Ribeiro-Dasilva MC, Rahim-Williams B and Riley JL. Sex, gender,
and pain: A review of recent clinical and experimental findings (2009) J Pain
10: 447-485. https://doi.org/10.1016/j.jpain.2008.12.001
25. Averitt
DL, Eidson LN, Doyle HH and Murphy AZ. Neuronal and glial factors contributing
to sex differences in opioid modulation of pain (2019) Neuropsychopharmacology
44: 155-165. https://doi.org/10.1038/s41386-018-0127-4
26. Dowell
D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain
(2016) United States, MMWR Recomm Rep 65: 1-49. https://doi.org/10.15585/mmwr.rr6501e1er
27.
Koda-Kimble
M and Young L. Applied Therapeutics: The Clinical Use of Drugs (2001)
Philadelphia, PA: Lippincott Williams and Wilkins
28. Hemsing
N, Greaves L, Poole N and Rose Schmidt. Misuse of Prescription Opioid Medication
among Women: A Scoping Review (2016) Pain Res Manag. https://doi.org/10.1155/2016/1754195
29. Opioid
Use and Opioid Use Disorder in Pregnancy. ACOG Committee Opinion No. 711.
American College of Obstetricians and Gynecologists (2017) Gynecol 130: e81-e94.
https://doi.org/10.1097/aog.0000000000002235
30. Lapane
KL, Quilliam BJ, Chow W and Kim MS. Pharmacologic management of non-cancer pain
among nursing home residents (2013) J Pain Symptom Manage 45: 33-42. https://doi.org/10.1016/j.jpainsymman.2011.12.285
31. Sandbrin
F and Uppal R. The time for opioid stewardship is now (2019) Jt Comm J Qual
Patient Saf 45: 1-2.
32. Perrone
J, Weiner SG and Nelson LS. Stewarding recovery from opioid crisis through
health system initiatives (2019) West J Emerg Med 20: 198-202. https://doi.org/10.5811/westjem.2018.11.39013
33.
Weiner
SG, Price CN, Atalay AJ, Harry EM, Pabo EA, et al. A health system-wide
initiative to decrease opioid-related morbidity and mortality (2019) Jt Comm J
Qual Pat Saf 45: 3-13.
34.
Naples
JG, Gellad WF and Hanlon JT. The role of opioid analgesics in geriatric pain
management (2016) Clin Geriatr Med 32: 725-735. https://doi.org/10.1016/j.cger.2016.06.006
35.
Dowell
D, Haegerich TM and Chou. CDC Guideline for Prescribing Opioids for Chronic
Pain-United States (2016) JAMA 315: 1624-1645. https://doi.org/10.1001/jama.2016.1464
*Corresponding
author: Robert G
Smith, Shoe String Podiatry, 723 Lucerne Circle, Ormond Beach, Florida 32174,
USA, Tel: 386-673-9933, Email: asamaan@cfl.rr.com
Citation
Smith RG. Clinical coping with
prescribing opioids within the context of obesity and diabetes mellitus (2019)
J Obesity and Diabetes 3: 39-44.