Introduction
The individual response to exercise is an
important clinical assessment tool because it provides a composite assessment of
the respiratory, cardiac, and metabolic systems. The current gold standard for
assessing ones aerobic exercise response is the maximum incremental
cardiopulmonary exercise test. However, most daily activities are performed at
submaximal levels of exertion; thus, using submaximal functional tests would
provide a more realistic simulation of ones physical capability [1-4]. The ability to walk
for a distance is a quick, easy, and inexpensive way to assess the physical
function of an individual. It is also an important component of quality of life
as it reflects the ability to undertake day-to-day activities. Balke developed
a simple test to examine the functional capacity by measuring the distance
walked during a defined period of time [5]. A 12-minute performance test was then developed to evaluate
the physical fitness of healthy individuals [6]. This test was subsequently modified for use in patients with
chronic bronchitis [7].
To allow patients with respiratory diseases for whom walking a 12-minute
distance was too demanding, a shortened version, of 6 minutes, was found to
provide comparable clinical information [8]. A recent review of functional walking tests concluded that
the six-minute-walk test (6MWT) is easy to perform with better acceptability by
participants, and provides a better reflection of activities of daily living
than other walk tests [4].
The American Thoracic Society has also recently endorsed and published
guidelines for performing the 6MWT in clinical settings [9]. The 6MWT has been frequently used to
measure outcomes before and after treatment in patients with moderate to severe
heart and lung diseases [10].
The aim of the study
·
To estimate the incapacity
of cardiac patients through the 6-minute walk test (6MWT) data.
·
To compare data of cardiac
patient group (PG; n =
100) with those of control group (CG).
Subjects
The Patients
One hundred cases (100) cases (52 males and 48 females) were
suffering from cardiac diseases (42 suffering from CHD, 38 suffering from RHD
and remaining 20 cases suffering from cardiomyopathy).
The Control
One hundred (100) healthy children (50 males, 50 females).From
primary, preparatory and secondary schools from the same age category of the patients.
Inclusion
criteria
All children have cardiac diseases from age of 5 to 18 years.
Exclusion
criteria
·
Children with acute
respiratory condition.
·
Children with chronic
systemic illness like respiratory, hepatic, renal, neurologic, or GIT
conditions.
·
Children with skeletal
disorders.
·
Children with hemodynamic
disorder like anemia or heart failure.
Tools
of study
·
All
cases (patients and control) included in the study were subjected to Anthropometric measures like (weight and height) according to
methods described by Reiter and
Rosenfield.
·
6MWT was performed according
to the guidelines of the American Thoracic Society.
Patient preparation
All patients worn comfortable clothes, appropriate shoeses for
walking were worn, the patients usual medical regimen was continued, a light
meal was taken before the test and patients were not exercised vigorously 2
hours
before the test.
Safety issues
The test was performed in pediatric cardiology unit at Assiut
University children hospital, where rapid response to an emergency was
possible. Oxygen source and telephone were in place to enable a call for help.
Technical aspects of the 6MWT
Location
The 6MWT was performed in pediatric cardiology unit at Assiut University
children hospital, where a long, flat, straight, enclosed corridor at a course
of 30 Meters was assigned. The length of the corridor was marked
every 3 m. The turnaround point was marked with a cone.
Results
The study was
conducted on pediatric cardiac patients from 5 years to 18 years of age admitted
at cardiology unit at Assiut University Children Hospital over one year in the
period from the 1st of August, 2016 to the 31th of July,
2017 and 100 healthy children age and sex matched with the patients.
Discussion
This study is a cross sectional study, that was conducted in the
pediatric cardiology unit at Assiut University children hospital to demonstrate
the effect of cardiac diseases on the functional capacity of children. It
included 100 children with heart disease and 100 age and sex matched control
children. The higher prevalence of children coming from rural areas in our
studied cases (Table 1) represents
the pattern of patients attending Assiut University Hospitals rather than
increased incidence of heart diseases in children of rural areas. However, Okello et al. [11], reported that there was a trend towards increased cardiac diseases
in children in association with overcrowding, unemployment and consanguinity
marriage.
Congenital heart defects represent the most common heart disease
in children 12]. Rheumatic heart disease in children still represents a major
cause of cardiac morbidity in developing countries [13]. Our results in this regard were in agreement with these authors.
It was found that congenital heart disease comprised 42 of the patients and 38%
have rheumatic heart diseases as showed in Table 2 and Figures
1-7.
Table 3 showed that mean of the
weight of the patients was 28.46 ± 12.892 , while that of the control was 37.05
±17.391 this difference was statistically significant (p. value <0.001),
also mean of the height was 130.12 ± 21.720 in the patients ,while in the
control it was 139.45 ± 22.321 which also statistically significant (p.value =
0.003) , this can be explained by that cardiac diseases are chronic diseases
that affect growth and development of the patients, and this was in agreement
with Nasiruzzamarrt et al.[14]who reported that children having heart diseases were more prone
to developed growth and developmental delay. This growth retardation in
children with heart diseases is due to recurrent infections and long hospitals
stay [15].
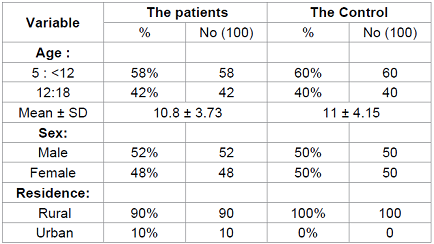
Table 1: Demographic Data.
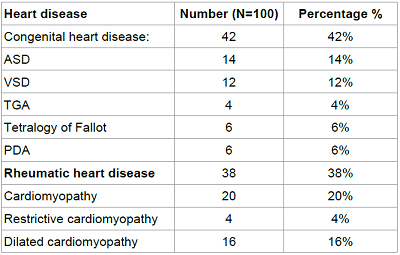
Table 2: Cardiac diseases among the studied patients.

Figure 1: The age distribution of the patients.

Figure 2: The age distribution of the Control.
Figure 3: The sex distribution of the patients.
Figure 4: The sex distribution of the control.
Figure 5: The residence distribution of the patients.
Figure 6: The residence distribution of the control.
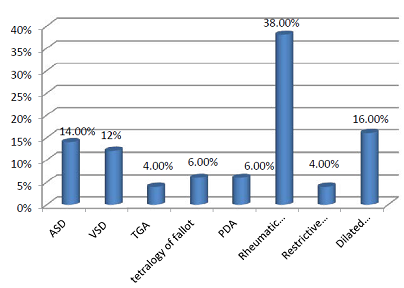
Figure 7: Cardiac diseases among the studied patients.
During exercise there is increase in oxygen consumption and
increase carbon dioxide production which leading to increase work of breathing
(RR) to compensate increased level of oxygen consumption and to eliminate
carbon dioxide, also during exercise blood flow to the muscles is increased due
to increase oxygen consumption , which requires increase in cardiac output. The
cardiac output is increased by both a rise in the heart rate and the stroke
volume attributable to a more complete emptying of the heart by a forcible
systolic contraction. Regarding blood pressure during exercise there is only a
moderate increase in blood pressure secondary to the rise in cardiac output.
This is caused by stretching of the walls of the arterioles and vasodilatation.
Despite increase oxygen consumption during exercise oxygen saturation not
significantly affected due to increase work of breathing (RR) and cardiac
output (HR and stroke volume). This is matched with our results in Tables 4 & 5 which show that mean HR
of the patient before the 6MWT was 100 ± 12.7 and after test was 130 ± 11.06,
which was statistically significant (p.value = 0.001), regarding mean HR of the
control before 6MWT was 89 ± 12.18 and after the test was 109 ± 9.47 , which
also statistically significant (p.value = 0.001). About mean RR of the patient
it was 24 ± 5.73 before the 6MWT and 42 ± 6.007 after the test with statistical
significance (p.value = 0.001), regarding mean RR of the control it was 20 ±
2.24 before the test and 32 ± 4.59 after the test with statistical significance
(p.value = 0.001). Regarding mean systolic / diastolic BP for the patients it
was 108 ± 9.22/65 ± 6.7 before the test and 117 ± 8.9/72 ± 6.2 after the test
with statistical significance (p.value = 0.001), also mean systolic / diastolic
BP of the control was 103 ± 10/ 62 ± 11.3 before the 6MWT and 108 ± 9.22 /65 ±
6.7 after the test with statistical significance (p.value = 0.001). Oxygen
saturation showed no statistical significance for both the patients and the
control. And this in agreement with Deborah et al., (2004) [16], who reported that exercise increase cardiac output (HR and stroke volume),
increase work of breathing (RR) with moderate increase in blood pressure. But
oxygen saturation not affected.
Table 6 showed comparison between
HR, RR, BP and SPO2 of the patients and the control before the 6MWT, about mean
HR of the patients was 100 ± 12 and for that of the control was 89 ± 12.18
which was statistically significant (p.value = 0.001). Regarding mean RR it was
24 ± 5.73 for the patients and 20 ± 2.24 for the control, which was also
statistically significant (p.value = 0.001).mean Systolic / diastolic BP of the
patients was 108 ± 9.22/65 ± 6.7 and of the control was 103 ± 10/ 62 ± 11.3, which
was statistically significant (p.value = 0.005 for systolic and 0.023 for
diastolic). Regarding oxygen saturation it was 95 ± 8.48 for the patients and
was 98 ± 0.488 for the control, which was statistically significant (p.value =
0.005). This can be explained by recurrent infections and recurrent attacks of
heart failure for which patients are exposed, and this in agreement with Jayaprasad[17], reported that the clinical features suggestive of heart failure in
children include tachypnea, tachycardia, feeding difficulty and diaphoresis.
Table 7 showed comparison between
HR, RR, BP and SPO2 of the patients and the control after the 6MWT, about mean
HR of the patients was 130 ± 11 and for that of the control was 109 ± 9.47
which was statistically significant (p.value = 0.001). Regarding mean RR it was
42 ± 6 for the patients and 32 ± 4.59 for the control, which was also
statistically significant (p.value = 0.001). mean Systolic / diastolic BP of
the patients was 120 ± 10/72 ± 8.1 and of the control was 109 ± 10/ 65 ± 6.2,
which was statistically significant (p.value = 0.029 for systolic and 0.023 for diastolic). Regarding oxygen saturation it was 93 ± 9.7 for the
patients and was 95 ± 8.48 for the control, which was statistically significant
(p.value = 0.034). Table 8 shows that the mean of the 6MWD of the males in the controls was
630 ± 90.12, which was in agreement with a study done by Albert et al., (2007)[18], who reported that the mean of 6MWD of his studied male subjects
was 680.9 ± 65.3, also in our study the mean of the 6MWD of the males in the
patients was 342.5 ± 102, which was 288 M less than the controls, and it was statistically significant (p.value = 0.001). Also Table 8 shows that the mean of the
6MWD of the females in the controls was 575 ± 63.2, which was in agreement with
a study done by Albert et al. [18], who reported that the mean of 6MWD of his studied female subjects was 642.7 (58.9), also in
our study the mean of the 6MWD of the females in the patients was 308 ± 118.2,
which was 267 M less than the controls, and it was statistically significant
(p.value = 0.001), this indicate that heart diseases affect the daily physical
activities of the patients, which was in agreement with NeslihaN et al. [19]who reported that cardiac
diseases, their assessment and treatment are major challenges for health care
providers throughout the world , it was found that patients with cardiac
diseases reported problems with diverse activities.

Table 3: Anthropometric parameters of the patients and the controls.
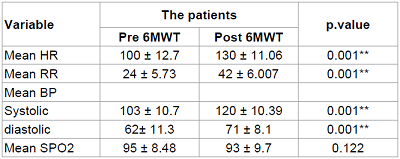
Table 4: Vital signs (HR, RR, BP, SPO2) pre and post 6MWT of the patients.

Table 5: Vital signs (HR, RR, BP and SPO2) pre and post 6MWT of the control.
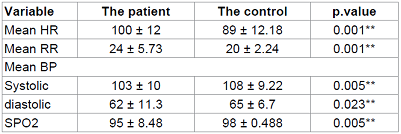
Table 6: Vital signs (HR, RR, BP and SPO2) pre 6MWT of the patient and control.

Table 7: vital signs (HR, RR, BP and SPO2) post 6MWT of the patient and the control.

Table 8: Mean of the 6MWD of both the patients group and the control
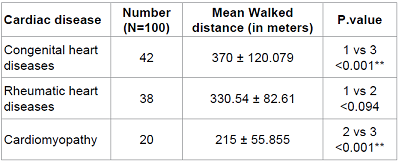
Table 9: Mean of the 6MWD of each category of cardiac diseases.
Table 9 shows that the mean of the
6MWD in patients suffering from cardiomyopathy was 215 ± 55.855, while that of
the patients having congenital heart diseases and rheumatic heart diseases was
(370 ± 120.079 and 330.54 ± 82.61) respectively for patients, which was
statistically significant (p.value <0.001), this is in agreement with Susanna et al.[20], who reported that large number of patients with dilated
cardiomyopathy undergo heart transplantation due to effect of cardiomyopathy in
quality of life. Which mean that the functional capacity of patients having
cardiomyopathy affected more than that of patients with CHD or RHD, this
because patients with cardiomyopathy may have impaired systolic and diastolic
functions which reflect on the function capacity.
Conclusion
The 6MWT is a simple, applicable test with a significant value in
the demonstration of the effect of cardiac diseases on the functional capacity
of pediatric cardiac patients. In our study we concluded that cardiac diseases
affects daily activities of affected children by decreasing the distance that they
can walk and cardiomyopathy affect the functional capacity more than other
cardiac diseases, cardiac diseases are common in low socioeconomic
nations, congenital heart diseases and rheumatic heart diseases are the most common
cardiac diseases in children and cardiac diseases affect growth and development
of pediatric cardiac patients.
Recommendations
1.
The 6MWT is a useful measure
of functional capacity targeted at people with at least moderately to severe impairment.
2.
The test should be widely
used for preoperative and postoperative evaluation and for measuring the
response to therapeutic interventions for pulmonary and cardiac disease.
3.
It is recommended to make a
data base for 6MWT in Egypt as up to our knowledge there is no study done about
the test in Egypt in Egyptian children.
4.
Early treatment and surgical
intervention if indicated in pediatric cardiac patients to avoid complications
and to avoid growth and development affection in those patients.
References
1. ATS
Committee on Proficiency Standards for Clinical Pulmonary Function
Laboratories. ATS statement: Guidelines for the Six Minute Walk Test (2002) Am
J Respir Crit Care Med 166:111-117.
2. Kierkegaard
M, Harms-Ringdahl K, Edstrom L, Widén Holmqvist L, Tollbäck A. Feasibility and effects of a physical
exercise programme in adults with myotonic dystrophy type 1: a randomized
controlled pilot study (2011) J Rehabil Med 43: 695-702.
3. Bartels
B, de Groot JF, Terwee CB. The Six-Minute Walk Test in Chronic Pediatric
Conditions: A Systematic Review of Measurement Properties (2012) Phys Ther 93:
4.
4. Solway
S, Brooks D, Lacasse Y, Thomas S. A
qualitative systemic overview of the measurement properties of functional walk
tests used in the cardiorespiratory domain (2001) Chest 119: 256-270.
5. Balke
B. A simple field tests for the assessment of physical fitness (1963) Rep Civ
Aeromed Res Inst US 53: 1-8.
6. Cooper
KH. A means of assessing maximal oxygen intake: correlation between field and
treadmill testing (1968) JAMA 203: 201-204.
7. Mcgavin
CR, Gupta SP, Mchardy GRJ. Twelve-minute walking test for assessing disability
in chronic bronchitis (1976) BMJ 1: 822-823.
8. Butland
RJA, Pang J, Gross ER, Woodcock AA, Geddes DM. 2, 6 and 12-minute walking tests
in respiratory disease (1982) BMJ 284:
1607-1608.
9. American
Thoracic Society. American Thoracic
Society statement: Guidelines for the six-minute walk test (2002) Am J Respir
Crit Care Med 166: 111-117.
10. Enright
PL. The six-minute walk test (2003) Respir Care 48: 783-785.
11. Okello
E, Kakande B, Sebatta E, Kayima J, Kuteesa M et al. Socioeconomic and
Environmental Risk Factors among Rheumatic Heart Disease Patients in Uganda
(2012) PLoS ONE 7: e4391.
12. Kalimuddin
Aziz. Incidence of Heart Disease in
Children at the National Institute of Cardiovascular Diseases (2010) JPMA 34:
300
13. Aly
A. Rheumatic fever (2011) Core concepts of pediatrics, University of Texas,
USA.
14. Nasiruzzamarrt,
MZ Hussain, MA Baki, MA Tayeba, MN Mollah. Growth and Developmental Status of
Children with Congenital Heart Disease (2011) Bangladesh Medical Journal 40: 2.
15. Costello
CL, Gellatly M, Daniel J, Justo RN, Weir K. Growth Restriction in Infants and
Young Children with Congenital Heart Disease (2015) Congenit Heart Dis 10:
447-456.
16. Deborah
Anne Burton, Keith Stokes, George M Hall.
Physiological effects of exercise; Continuing Education in Anaesthesia
(2004) Critical Care and Pain 4: 185-188.
17. Jayaprasad
N. Heart failure in children (2016) Heart Views 17: 92-99.
18. Li
AM, Yin J, Au JT, So HK, Tsang T, et al. Standard Reference for the
Six-Minute-Walk Test in Healthy Children Aged 7 to 16 Years (2007) Am J Respir
Crit Care Med 176: 174-180.
19. Neslihan
Duruturk, Eda Tonga, Metin Karatas, Ersin Doganozu. Activity performance
problems of patients with cardiac diseases and their impact on quality of life
(2015) J Phys Ther Sci 27: 2023-2028.
20. Susanna
L, Flipse DHK, Van der Meulen MH, Backx PCM, Marchie Sarvaas G et al.
Six-Minute Walk Test as a Predictor for Outcome in children with Dilated
Cardiomyopathy and Chronic Stable Heart Failure (2017) Pediatr Cardiol 38:
465-471.
*Corresponding author:
Mohammed Sayed Elyan, Pediatrics
department, Faculty of Medicine, Assiut University, Egypt, Tel: +201063540529, E-mail:
mohammedelyan645@gmail.com
Citation:
Elyan MS, Ahmed SEA, Farghaly HS. Six-Minute
Walk Test in Pediatric Cardiac Patients (2017) CCCM 1: 13-17.