Introduction
Hypertension is a prevalent
predictor of cardiovascular problems and considers a leading risk factor for
mortality worldwide especially in low- and middle-income countries [1]. It is
estimated to have caused 9.4 million deaths and 7% of disease burden-as
measured in DALYs-in 2010 [2]. According to WHO, the global prevalence of
hypertension in 2014 among adults aged≥18 years was around 22% with the highest
prevalence was in Africa 30% and the lowest was in the Region of the Americas
18%. Males had slightly higher prevalence of hypertension than females [2].
Approximately one billion persons
are living with uncontrolled hypertension worldwide [3]. In spite of intensive
medical treatment, hypertension often remains uncontrolled in general practice.
Uncontrolled hypertension is the major cause of heart failure in females and
numbers two of most common cause heart failure in males [4]. It accounts for
40% of deaths from ischemic heart disease and 51%
of all stroke deaths worldwide
[4,5]. Uncontrolled hypertension can also cause myocardial infarction, stroke,
congestive heart failure, end-
Stage renal disease, peripheral
vascular disease, and retinal blood vessels damage [4-7].
Control of hypertension is
associated with low probability of hypertensions complication. A drop in
systolic blood pressure of 10 mmHg is associated with 22% drooping in coronary
heart disease, 41% drooping in stroke [8], and a 41-46% drooping in cardio metabolic
mortality [9]. The prevalence of controlled hypertension differs from one
country to another. It was reported in 6.6% of the hypertensive cases in India
[10], 11.8% in China [11], 19.9% in Romania [12], 15.8% in Iran [13] and 37% in
Saudi Arabia [14], 52.5% in Panama [15] and 46.5% in United States [16].
There are many reported risk factors related
to poor BP control; cigarette smoking, bad socio-economic status, lifestyle,
male sex, old age obesity and poor compliance to antihypertensive drugs [11,17,18].
Non-adherence to anti-hypertensive influences its effectiveness and increase
the possibility of uncontrolled hypertension and the subsequent complications
such as stroke and ischemic heart diseases [18]. Presence of co-morbidities and
intake of less aggressive treatment were significant barriers of controlling
blood pressure [19]. The aim of the study was to determine the prevalence of
uncontrolled hypertension among adult Yemeni patients and to identify the
associated risk factors.
Patients and
Methods
This cross-sectional study
involved adult patients consecutively presented to Cardiac Centre (CC) in Sanaa
with uncontrolled hypertension during 2016. This center serves large number of
population from all areas of the Republic of Yemen. Uncontrolled hypertension
is defined as an average systolic blood pressure ≥140 mmHg or an average
diastolic blood pressure ≥90 mmHg, among those who are under anti-hypertensive
treatment. Inclusion and Exclusion Criteria. All patients aged 18 year or more
who diagnosed as having hypertension for at least three months prior to
attending to the Centre and he/she under
treatment were included in this study. Newly diagnosed patients who have been
taking antihypertensive treatment for less than one month were excluded from
the study.
All patients were subjected to
through clinical examination including; blood pressure measurement, laboratory
investigations such as hemoglobin, serum creatinine, serum electrolytes lipid
profile ECG and echocardiogram. Other data such as age, sex, special habits,
and duration of hypertension, type of treatment and weight and height were
enquired about and recorded. We asked patient to come after 3 months for follow
up and investigation was repeated.
Definition: We considered control hyper tension if:
Systolic 120-139 mm Hg, diastolic 80-89 mm Hg.
Stage
1: Hyper tension if Systolic 140-159 mm Hg, diastolic
90-99 mm Hg.
Stage
2: Hyper tension if Systolic 160 mm Hg or greater,
diastolic 100 mm Hg or greater.
Data
Analysis: All data was coded entered in to
PC. And analyzed by SPSS program version
22. Frequency (%) was used to describe the qualitative variables. Quantitative
variables were described by mean and standard deviation as the data were
normally distributed. Chi- square (Chi-square and Chi-square with Yate
correction) tests were used to show the significant of association between the
outcome and other independent variables. P-values of <0.05 were considered
significant.
Ethical
Consideration: Permission to conduct this study was
granted by Arab Board of Medical in particular the Research Committee.
Results
A total number of hypertensive
patients participated in this study was 277. There were 187 (67.5%) males and
90 (32.5%) females. Age of the patients ranged from 27 to 100 year and main age
57.5 year ± 12.3. The general characters
of the patients are illustrated in Table
1.
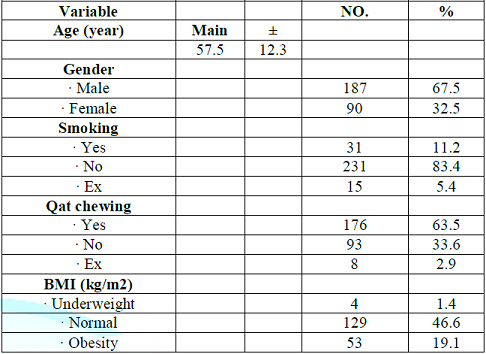
Table 1: General characteristics of the patients presented with hypertension (n=277).
Among the total patients, 31
(11.2%) were current smokers and 176 (63.5%) were Qat (Chat) chewers. Body mass
index in 144 (52%) patients, either they were overweight 91(32,9%) or found to
be obese 53(19.1%).
Uncontrolled blood pressure were
found in 243 patients of them 61 patients(22.0%) had
stage I hypertension ( HTN) and 182 Patients(65.7%) were in stage II ( HTN). The pattern of uncontrolled
hyper tension is shown in Table 2.
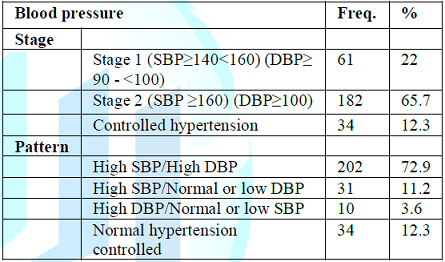
Table 2: Stages and pattern of uncontrolled hypertension among study patients (243).
In this study, the prevalence of
uncontrolled hypertension was 243 (87.7%). Most of the hypertensive patients in
this study took combined antihypertensive drugs 124 (51.0%), the combination
either two drugs which represented 93 (38.3%) or more than two drugs 31
(12.7%). However, 119 cases were used one drug only Table 3.
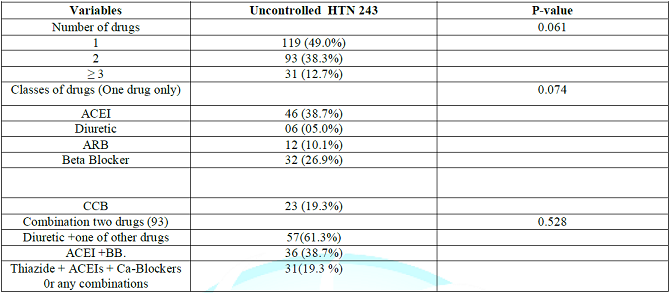
Table 3: Distribution of uncontrolled hypertensive patients by antihypertensive drugs.
Those patients who achieved target BP (<140/90 mmHg)
were 34 (12.3 %) Patients. Of whom 18 patients (53.0%) were under 2 medications
& 16(47. 0%) on mono-therapy. The most common combined therapy were ACEI +
Diuretic and the most common prescribed mono-therapy was ACEI then Beta blocker
drugs in both groups. The classes of antihypertensive agents had no influence
on the blood pressure controlled.
Associated comorbidity and risk
factors with uncontrolled hypertension patients is shown in Table 4. Elder patients with age more than 65 years, IHD,
LVH, high creatinine level, found to be significant risk factors for
uncontrolled hyper tension with P value (0.031, 0.015, 0.010 and 0.041)
respectively.
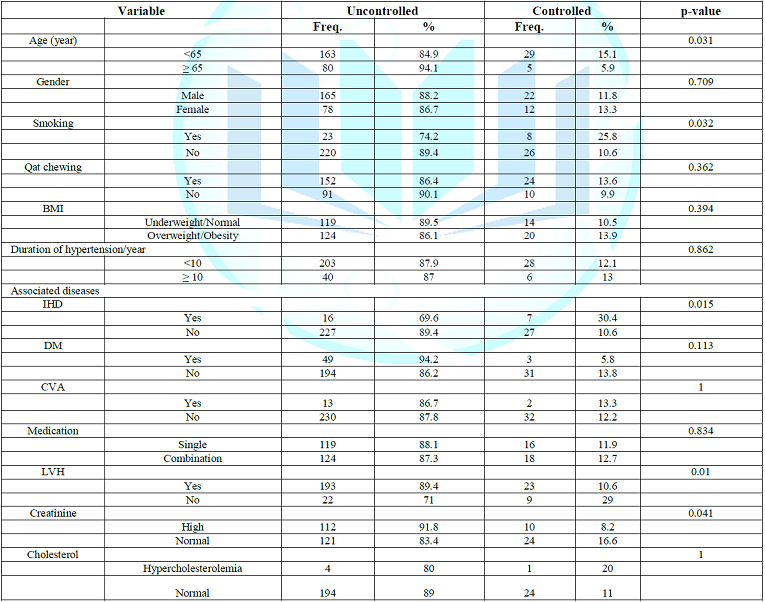
Table 4: Association between comorbidity and risk factors with uncontrolled hypertension patients.
There were no significant
association between uncontrolled hypertension and other variables (gender, Qat
chewing, BMI, duration of hypertension, associated diseases, DM, CVA,
medication and blood cholesterol level as shown in Table 4.
Discussion
In this study we found that, only
34 (12.3 %) of patients their blood
pressure have been controlled and achieved target BP (<140/90 mmHg). This
figure was less than the previous reported from neighbors countries such as Oman, Saudi
Arabia & Bahrain, they reported ((39%), 25% and 16.5%) respectively
[20-22]. Globally hypertension
control rates vary from one country to
another ranging as low as 5.4% in
Korea to as high as 58% in Barbados which clearly
demonstrate the world wide
difficulty in achieving satisfactory blood pressure control [23].
There are numerous potential
reasons for low rates of BP control in
our patients among these could be, poor access to health care, unaffordable to
pay medications & lack of adherence
with long term therapy for a condition that is usually asymptomatic [24]. Moreover, the immediate
benefit of the therapy may be not obvious to the patients and make patient redundant to continue with
drugs. Other reason the drug may interferers with the patients quality of life.
Our study the majority (87%) of
hypertensive patients failed to reach the targeted BP goals and exposed patients
to the risk of heart attack, strokes and other hypertension related disease
with consequent impact on morbidity
and mortality [25]. Wong et al(2003),estimated
that control of hypertension to
levels recommended by the JNC could prevent 19-50% to coronary heart disease
events in men and 31-57% of coronary
heart disease events in women
depending on the BP achieved
[26]. So that, substantial number of cardiovascular events can be prevented by
improving BP control.
Despite that most of our patients
were taking 2 or more medications and their counterpart were taking
mono-therapy, the controlled blood pressure in both groups had no significant
difference. This finding seem
to be contradicted with what
was concluded by major clinical trial
that effective BP control is better
achieved with 2 or more
antihypertensive medications for most patients [27,28]. Reality our
patients who were under two medications were most of them had left ventricular
hypertrophy which may reflect longstanding uncontrolled hypertension or other
comorbidity diseases which may play negative role in controlling blood
pressure.
In this study we found positive
association between left ventricular hypertrophy, renal impairment and
uncontrolled hypertension, this result coincide with reports from other studies
[29]. However, ischemic heart disease was found to be relatively associated
with better BP control, such a positive effect was observed by other studies as
well [30,31]. This result might be explained by better compliance in those
patients or more aggressive treatment they received.
Conclusion
Hypertension was not adequately
controlled in the majority of the treated patients. Comorbidity diseases such
as renal impairment, left ventricular hypertrophy and ageing found to be
associated factors for uncontrolled hyper tension.
Recommendation
1. Further effort is needed from
attendant physicians to explain the major complications of uncontrolled
hypertension to the patient & his family to support the patient compliance
to his medications.
2. Country wide study is needed
to identify those patients with uncontrolled hypertension and to develop National
hypertension control program.
Limitations
Important limitation in our study
were difficulty in convincing the patient for regular follow up and recurrent
visit because significant number of patient were coming from outside Sana a
city.
Acknowledgment
The authors would like to thank
Dr. Farook Alkadasi for his generous help with the statistical part of the
study.
References
1.
Narayan KV, Ali MK and Koplan JP.
Global non- communicable diseases-where worlds meet (2010) N Engl J Med 363:
1196-1198. https://doi.org/10.1056/NEJMp1002024
2.
Global status report on
non-communicable diseases (2014) World Health Organization.
3.
European Society of Hypertension
(ESH) and of the European Society of Cardiology (ESC) (2013) Eur Heart J 34:
2159-2219.
4.
Di Cesare M, Bennett JE, Best N,
Stevens GA, Danaei G and et al. The contributions of risk factor trends to
cardiometabolic mortality decline in 26 industrialized countries (2013) Int J
Epidemiol 42: 838-848. https://doi.org/10.1093/ije/dyt063
5.
Staessen JA, Kuznetsova T and Stolarz
K. Hypertension prevalence and stroke mortality across populations (2003) JAMA 289:
2420-2422. https://doi.org/10.1001/jama.289.18.2420
6.
Mancia G, Fagard R, Narkiewicz K,
Redon J, Zanchetti A and et al. 2013
ESH/ESC guidelines for the management of arterial hypertension: the Task Force
for the Management of Arterial Hypertension of the European Society of
Hypertension (ESH) and of the European Society of Cardiology (ESC) (2013)
European Heart J 34: 2159-2219. https://doi.org/10.1097/01.hjh.0000431740.32696.cc
7.
Talaei M, Sadeghi M, Mohammadifard
N, Shokouh P, Oveisgharan S, et al. Incident hypertension and its predictors:
the Isfahan Cohort Study (2014) J
Hypertens 32: 30-38. https://doi.org/10.1097/HJH.0b013e32836591d4
8.
Mendis S, Puska P and Norrving B.
Global Atlas on cardiovascular disease prevention and control (2011) Geneva:
World Health Organization.
9.
Law MR, Morris JK and Wald NJ.
Use of blood pressure lowering drugs in the prevention of cardiovascular disease:
meta-analysis of 147 randomised trials in the context of expectations from
prospective epidemiological studies (2009) BMJ 338: 665. https://doi.org/10.1136/bmj.b1665
10. Manunta
P, Cusi D, Barlassina C, Righetti M, Lanzani C, et al. Alpha-adducin
polymorphisms and renal sodium handling in essential hypertensive patients
(1998) Kidney Int 53:1471-1478. https://doi.org/10.1046/j.1523-1755.1998.00931.x
11. Kaur
P, Rao SR, Radhakrishnan E, Rajasekar D and Gupte MD. Prevalence, awareness,
treatment, control and risk factors for hypertension in a rural population in
South India (2012) Int J Public Health 57: 87-94. https://doi.org/10.1007/s00038-011-0303-3
12. Cai
L, Liu A, Zhang L, Li S and Wang P. Prevalence, awareness, treatment, and
control of hypertension among adults in Beijing, China (2012) Clin Exp
Hypertens 34: 45-52. https://doi.org/10.3109/10641963.2011.618206
13. Saeed
AA, Al-Hamdan NA, Bahnassy AA, Abdalla AM, Abbas MA, et al. Prevalence, awareness,
treatment, and control of hypertension among saudi adult population: a National
Survey (2011) Int J Hypertens 2011: 174135.
https://doi.org/10.4061/2011/174135
14. Dorobantu
M, Darabont RO, Badila E and Ghiorghe S. Prevalence, awareness, treatment, and
control of hypertension in romania: results of the SEPHAR study (2010) Int J
Hypertens 2010: 970694. http://dx.doi.org/10.4061/2010/970694
15. McDonald
A, Motta J, Roa R, Fontes F, Batista I, et al. Prevalencia de Factores de
Riesgo Asociados a Enfermedad Cardiovascular (2012) Instituto Conmemorativo
Gorgas de Estudios de la Salud, Panama, USA.
16. Disease
Control and Prevention. Vital Signs: Awareness and treatment of uncontrolled
hypertension among adults - United States, 2003 -2010 (2012) Morbidity and
Mortality Weekly Report 61: 703-709.
17. Hussain
AA, Elzubier AG and Ahmed ME. Target organ involvement in hypertensive patients
in Eastern Sudan (1999) J Human Hypertension 13: 9-12. https://doi.org/10.1038/sj.jhh.1000719
18. Fatma
Mostafa Mahrous. Factors affecting compliance of hypertensive patients toward
therapeutic regimen (2015) Life Sci J 12: 62.
19. Al-Saadi
R, Al-Shukaili S, Al-Mahrazi S and Al- Busaidi Z. Prevalence of uncontrolled
hypertension in primary care settings in Al seeb wilayat, oman (2011) Sultan
Qaboos Univ Med J 11: 349-356.
20. Rashid
Al-Saadi, Sulaiman Al-Shukaili, Suleiman Al-Mahrazi and Zakiya Al-Busaidi.
Prevalence of Uncontrolled Hypertension in Primary Care Settings in Al Seeb Wilayat
(2011) SQU MED J 11: 349-356.
21. Al-Rukban
MO, Al-Sughair AM, Al-Bader BO and Al-Tolaihi BA. Management of hypertensive
patients in Primary health care setting: Auditing the Practice (2007) Saudi Med
J 28: 85-90.
22. Al
Khaja KA, Sequeira RP and Damanhori AH. Treatment of hypertension in Bahrain
(2003) Ann pharmacother 37: 1511-1517. https://doi.org/10.1345/aph.1C430
23. Chobanian
AV, Bakris GL, Black HR, Cushman WC, Green LA, et al. The seventh Report of the
joint National committee on Prevention, Detection, Evaluation, and treatment of
high blood pressure: The JNC 7 report (2003) JAMA 289: 2560-2572. https://doi.org/10.1001/jama.289.19.2560
24. Wang
TJ and Vasan RS. Epidemiology of uncontrolled hypertension in the United States
(2005) Circulation 112: 1651. https://doi.org/10.1161/CIRCULATIONAHA.104.490599
25. Greenland
P, Knoll MD, Stamler J, Neaton JD, Dyer AR, et al. Major risk factors as
antecedents of fatal and non-fatal
coronary heart disease events (2003) JAMA 290: 891. https://doi.org/10.1001/jama.290.7.891
26. Wong
ND, Thakral G, Franklin SS, Lltalien GI, lacobs Mj, et al. Preventing heart
disease by controlling hypertension: Impact of hypertensive subtype, stage,
age, and sex (2003) Am Heart J 145: 888-895.
https://doi.org/10.1016/S0002-8703(02)94787-3
27. Fox
JC Leight K, Sutradhar SC, Demopoulos LA, Gleim GW, Lewin AJ, et al. The JNC -7
Approch compared to conventional treatment in diabetic patients
with hypertension; A double –blind trial
of initial monotherapy vs combination therapy (2004) J Clin
Hypertens (Greenwich) 6: 437-442.
28. Neutel
JM, Smith DH, Weber MA, Schofield L, Purkatastha D, et al. Efficacy of
combination therapy for systolic
blood pressure in patients with
severe systolic hypertension: The systolic
Evaluation of Lotrel Efficacy
and Comparative Therapies
(SELECT) study (2005) J Clin Hypertens
7: 641-646. https://doi.org/10.1111/j.1524-6175.2005.04615.x
29. Almahrezi
A, Al-Zakwani I, Al-Aamri A, Al-Khaldi S, Al-Zadjali N, et al. Control and
management of hypertension at a university health center in Oman (2006) SQU Med
J 8: 179-184.
30. Deqli
Esposti E, Di Martino M, Sturani A,
Russo P, Dradi C, et al. Risk factors
for uncontrolled
hypertension in Itally (2004) J Hum
Hypertens 18: 207-213. https://doi.org/10.1038/sj.jhh.1001656
31. Knight
EL, Bohn RI, Wang PS, Glynn RJ,
Mogun H, et al, Predictors of
uncontrolled hypertension in ambulatory
patients (2001) Hypertension 38: 809-814. https://doi.org/10.1161/hy0901.091681
*Corresponding author:
Al-Aghbari Khaled, Associated professor of internal Medicine, Sana University, Yemen, Tel: 967711118376, E-mail: dr_khaled_alaghbari@yahoo.com
Citation:
Khaled AA, Mohammed B and Faiza A. Uncontrolled hypertension among treated hypertensive patients (2018) Clinical Cardiol Cardiovascular Med 2: 12-16.