Introduction
Endothelial
dysfunction/injury is the prime reason for the development of
atherosclerosis and its sequel (vulnerable plaque) which likely results into
Acute Coronary Syndrome [1-5]. Till date, therapy is directed towards
antiplatelet, lipid-lowering and thrombus removal by drugs or intervention in
ACS [6,7]. Healthy endothelium has the antiplatelet/antithrombotic and
fibrinolytic property [8-11].
Literature is lacking in the strengthening of endothelium and
utilizing the above properties
in ACS. Therefore this study focuses upon endothelial cells strengthening
in ACS and to observe its impact upon the clinical profile of ACS. Triphala a
mixture of Amla (Phyllanthus emblica),
Harad (Terminalia chebula), Behda (Terminalia bellirica) as strong properties
to support endothelium. Previous studies have found the pivotal role of Amla in
increasing ATP synthesis and removing oxidative stress at the cellular level
[12-14].
Methods
This is a double-blind randomized interventional control
trial. Arbitrarily 80 cases of ACS coming to the emergency department of an
institute were selected and randomized for study between 1st April 2017 to 30th
September 2018 (recruitment period/randomization period) [15]. The cases were
randomly divided into two groups. Group 1 (n=40, control), group 2 (n=40,
intervention). This stratification was not based upon severity into cases and
controls. Randomization protocol was decided even before the registration of
first case through random number generated by computer, alternate patients were
given into cases and controls. First case was allotted to group 1 and next case
was allotted to group 2. If any case in group 2 was excluded at any time, the
next was allotted to group 1. Alternate sequence was followed till the
recruitment of last case.
Further stratification into subgroups A and B was based upon
the clinical profile into UA (subgroup B) or STEMI (subgroup A). The age group
was 35-65 years, all males. Complete history and examination including pulse
rate, blood pressure,
respiratory rate, and oxygen saturation were recorded. Informed written consent
(especially requirement of urgent intervention) and approval of institutional
ethical committee was taken. In both groups cases having STEMI were categorized
into subgroup A i.e. Subgroup 1A (n=20) and 2A (n=20) respectively. Cases
having UA were categorized into subgroup B i.e. Subgroup 1B (n=20) and 2B
(n=20) respectively. No follow-up protocol after the discharge from the
hospital was planned.
Inclusion Criteria
Cases coming with chest pain typical of coronary artery disease
suggestive of Acute
Coronary Syndrome along with ECG changes (depression or elevation) were
selected for the study.
Exclusion Criteria
Patient
coming with severe chest pain requiring morphine, breathlessness, shock, any
degree of block or arrhythmia
in ECG and any past history of cerebrovascular accident or patients requiring
urgent cardiac intervention (thrombolysis/ coronary angiography) were excluded.
Intervention:
Intervention was done during shifting to ICU (Intensive Care Unit) from the
emergency unit and a close watch was kept on the patients.
Group1: (control)
Patients were given clopidogrel 300 mg, aspirin 300 mg, and atorvastatin 80 mg
stat with 10 grams of lactobacillus
powder dissolved in a cup of water with subjected to thrombolysis or CAG if
required.
Group 2: (Intervention)
Patients were given clopidogrel 300 mg, aspirin 300 mg, and atorvastatin 80 mg
stat with 10 grams of Triphala powder dissolved in a cup of water with
subjected to thrombolysis or CAG if required. Flavored essence and the
artificial color were added to both liquids to make liquids identical.
Outcome Measurement
1. Relief in chest pain (at 50
minutes).
2. ECG changes- initial ST-T
changes like elevation or depression was
compared with ST-T changes at 50 minutes.
3. Echocardiography changes-
regional wall abnormality and LV functions (Left Ventricular) initial were
compared with changes at 50 minutes in 2D and M-mode Echocardiography (GE
vivid s 6 probe M4s/RS machine).
4. The requirement of
pharmaco-invasive therapy-Patients requiring thrombolysis in view of ongoing
chest pain/ECG changes and not willing for CAG (during or after 50 minutes).
5. The requirement of urgent coronary angiography-
Patients requiring CAG in view of ongoing chest pain/ECG changes (during or
after 50 minutes).
Sympathetic Activity Assessment
(Done
at the time of admission by 2 methods)
1. Heart rate measurement in
ECG (>100/minute, overt increase)
2. SSR (Sympathetic Skin Response)-
Recorded without any stimulation only at room temperature of 22-240C in ICU by
applying 2 EMG electrodes over palm and forearm RMS (Recorder and Medicare
System) at the time of admission, if spike response is present then it suggests
high basal sympathetic discharge [16].
Statistical Analysis
The collected data were entered in a Microsoft Excel sheet.
Statistical analysis was carried out by using SPSS 20.0 Statistical software.
The appropriate test of significance was applied (Chi-square test).
Results
1. Maximum
cases (90%) presented within the first 6 hours of symptoms. These cases were
asymptomatic i.e. no chest pain, no discomfort before 24-48 hours.
2. Sympathetic activity
assessment- In group 1 and 2 mean pulse rate/minute was 84 and 86 (admission
time), 15% cases had an overt increase in sympathetic activity, in SSR spike
response was present in almost 90% cases suggestive of increased basal
sympathetic discharge.
3. In group 1 and 2 mean blood
pressure in mm Hg was 156/84 and 158/82 (admission time) and 152/80 and 148/84
(during last one year) mean Hba1c% (glycosylated hemoglobin)
was 8.5 and 8.8 (admission time), and 8.9 and 8.6 (during last one year) mean
LDL mg% (Low Density Lipoprotein) was 130 and 138 (admission time) and 141 and
139 respectively (during last one year). History of smoking/tobacco intake was
10%.
4. In intervention group 2 as
a whole, there was significant relief in chest pain, settling down of ST-T
changes in ECG, and improvement in regional wall motion in echocardiography as
compared to group 1(p<0.001).
5. In intervention subgroups
2A and 2B, there was significant relief in chest pain, settling down of ST-T
changes in ECG, and improvement in regional wall motion in echocardiography as
compared to group 1A and 1B (2A v/s 1A, 2B v/s 1B, p<0.001) (Figures 1-7) No
major side effects like fall in blood pressure, tachycardia were observed only
minor side effects like nausea and upper abdominal discomfort was present in 5%
of cases.
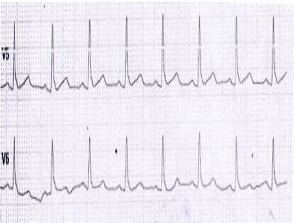
Figure 1: USA- (Pre) lead V5-V6- ST up sloping.
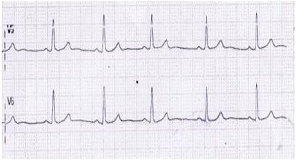
Figure 2: USA (Post) lead V5-V6- ST settling down.
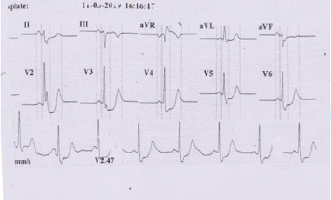
Figure 3: STEMI- Pre-acute infero posterior MI with
reciprocal changes in anterior leads (presented after 24 hours, ongoing chest
pain).
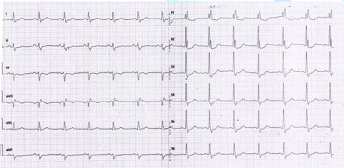
Figure 4: STEMI- Post- ST settling down in inferior leads and
reversal of reciprocal changes in anterior leads, relief in chest pain.
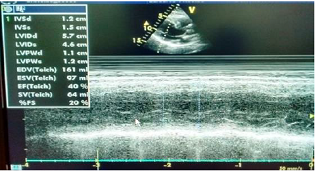
Figure 5: STEMI presented in one hour- Echocardiography
showing hypokinetic posterior wall (M-mode).
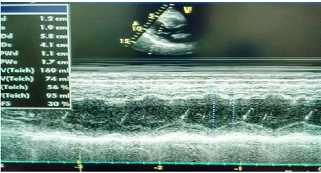
Figure 6: STEMI- Normal wall motion of posterior wall
(M-mode).
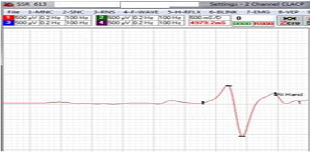
Figure 7: Increased basal sympathetic discharge (spike
response in all groups).
Discussion
Endothelial dysfunction/injury is found to be the prime
reason for the development of atherosclerosis and its sequel (vulnerable
plaque) which likely leads to ACS [1-5]. In this modern time with development
in various horizons of medicine, the therapeutics is mostly directed towards
antiplatelet, lipid-lowering and thrombus removal by drugs or intervention in
ACS [6,7]. Literature related to endothelial strengthening in ACS is lacking,
therefore, the study was planned to see the effect of endothelial strengthening
on clinical profile in ACS. Triphala powder a mixture of Amla (Phyllanthus emblica), Harad (Terminalia chebula), Behda (Terminalia bellirica) has strong
properties to support endothelium [12-14]. This is a double-blind randomized
interventional control trial. 80 cases from the emergency department of an
institute were randomly selected for the study. Cases having chest pain typical
of coronary artery
disease, history suggestive of ACS with ECG changes were included for the
study. The cases were randomly divided into two groups. Group 1 (n=40,
control), group 2 (n=40, study). In both groups cases having UA were
categorized into subgroup B i.e., Subgroup 1B and 2B respectively.
Cases having STEMI were categorized into subgroup A i.e.
Subgroup 1A and 2A respectively. The age group was 35-65 years, all males in
both groups and subgroups. All cases in subgroup 1A, 1B, 2A, 2B were given
clopidogrel, aspirin, and atorvastatin. In addition intervention subgroups 2A
and 2B were given Triphala powder, whereas control subgroups were given lactobacillus powder dissolved in a cup
of water. The results were observed at 50 minutes for outcome measurement for
relief in chest pain, ECG changes, Echocardiography changes, and the
requirement of thrombolysis or CAG. After 50 minutes, in subgroups 2B v/s 1B,
there was significant relief in chest pain (100% v/s 10%), ST-T changes
settling down in ECG (100% v/s 10%) and improvement in ECHO findings (100% v/s
5%) (p<0.001). After 50 minutes, in Group 2A v/s 1A, there was significant
relief in chest pain (90% v/s 10%), ST-T changes settling down in ECG (80% v/s
5%) and improvement in ECHO findings (75% v/s 5%) (p<0.001) (Table 1,2).
We revise our
findings/interpretations
1. Acute development of
symptoms/findings of UA/STEMI in an asymptomatic person in less than 24 hours
suggested by history, ECG, ECHO findings.
2. Presence of one or more
risk factors for atherosclerosis like hypertension/diabetes/dyslipidemia/smoking
etc. in almost 70% in all groups and subgroups for last many years.
3. No significant change in
blood pressure/ diabetes status (HbA1c)/ lipid (LDL) values at the time of
admission and the mean value for the past 12 months.
4. Increased basal/overt
sympathetic discharge in all groups and subgroups at the time of admission. SSR
showed spikes in 90% of cases.
5. A significant response to
treatment in chest pain, ECG, ECHO findings (p<0.001) in subgroup 2A and 2B,
as compared to subgroup 1A and 1B respectively.
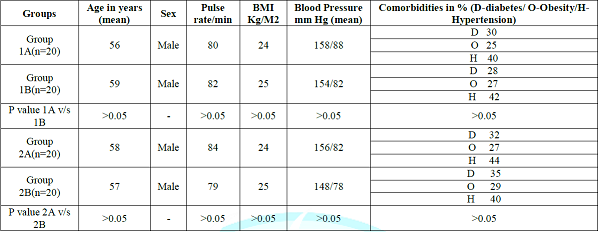
Table 1: Basic characteristic of the patients.
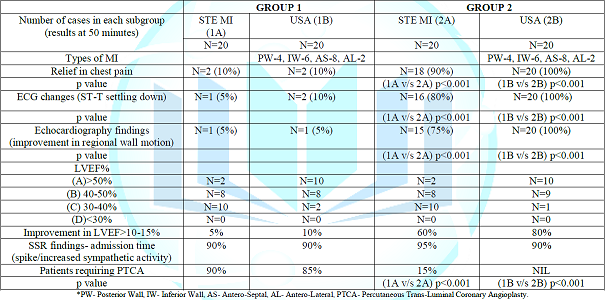
Table 2: Clinical profile/ECG/Echocardiography findings.
Endothelial
dysfunction (A possible mechanism)
In
the current study history was classical for ACS and suggestive of acute
development of symptoms i.e. person asymptomatic one day back and symptomatic
very next day. How healthy endothelium becomes unhealthy? (Healthy endothelium
behaves normally to exercise, changes in weather like from winter to summer or
summer to winter by increasing or decreasing the ATP level according to the
demand. Endothelial dysfunction is the compromise of normal function of
endothelial cells leading to the inability of arteries and arterioles to dilate
fully in response to an appropriate stimulus which can be further elaborated
into atherosclerosis and rupture of vulnerable plaque) [17,18]. In both groups
and all subgroups atherosclerosis
risk factors remained grossly unchanged during the last 12 months and at
admission time, therefore how these factors become critical in less than 24
hours? So their role in the development of ACS remains uncertain. Previous
literature hasnt discussed acute blockade in vasa vasorum (blood supply to
coronaries) [19,20].
A possible explanation remains in cellular energy metabolism.
In the presence of normal blood supply to coronary endothelial cells, ATP
production occurs at a normal rate and no endothelial dysfunction occurs (ATP
is the final energy source for all cells, synthesized in mitochondria of each
cell via aerobic respiration by oxygen and glucose), If there is sudden change
in ATP requirement then despite normal availability of oxygen and glucose
supply cells are unable to cope up with new rate of ATP synthesis and a
mismatch (demand/synthesis of ATP) occurs. Increased sympathetic activity
present at the time of admission (basal/overt) increases ATP requirement [21].
Other reasons for ATP mismatch may be exposure to sudden environmental
temperature change. In the current study sudden development of ACS, symptoms
could be attributed to a mismatch in ATP supply at the cellular level (coronary endothelial cells)
which results in endothelial dysfunction. Endothelial dysfunction results in the
inability of coronary vessels to dilate in response to various stimuli,
symptoms of angina arise, in severe cases breach in endothelial cells layer
occur, there is entry of platelets, inflammatory cells, cascade of events
occur, endothelium is unable to hold the plaque, plaque ruptures into the lumen
there is block in lumen of coronary vessels, results in STEMI [22-26].
Endothelial cells
strengthening: (A possible mechanism)
Triphala
powder contains Amla, which increases spare mitochondrial respiratory capacity
to increase the synthesis of ATP, a difference between basal ATP synthesis and
maximum ATP synthesis. Sufficient availability of ATP prevents cellular
dysfunction/breach in coronary endothelium [27]. Amla also stimulates the
antioxidant system, has cytoprotective
effect removing oxidative stress. Amla has a cooling property whereas harad
and behda have a warm effect to the body. Combination of all three makes
suitable for all seasons and protects from a change in ATP requirement due to
seasonal change or BMR. The overall effect is stabilization or strengthening of
the endothelium. Once the endothelium is stabilized/ strengthened then it
behaves like healthy endothelium quickly normalizes the flow in the coronary
vasculature, and removes findings of ACS in the following way (Figure 8).
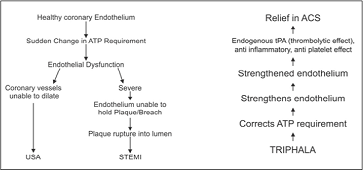
Figure 8: Endothelial Cell Dysfunction/Endothelium
Strengthening- Possible Mechanism.
Unstable
Angina: After endothelial stabilization, endothelium exerts effects
like healthy endothelium in normal circulation i.e., vasodilatory effect which
reduces angina pain, removes micro thrombi, removes the possibility of breach
in endothelium, inhibits accumulation of platelets, entry of inflammatory
cells, lipids, and overall plaque is no more unstable. Clinically effect is
observed in the form of symptomatic improvement in chest pain, ECG and
echocardiography findings (Subgroup 2B) [18,27-33].
STEMI: Besides all
effects observed above additional advantage is observed in the form of
thrombolytic effect by the support to the extra release of endogenous tPA (Tissue Plasminogen
Activator) normally released from damaged endothelium. Clinically effect is
observed in the form of improvement in chest pain, ECG and echocardiography
findings (subgroup 2A) [27-33].
Summary
Sudden mismatch or unavailability in ATP supply in
endothelial cells resulted in endothelial dysfunction. ATP mismatch occurred
primarily due to an increase in sympathetic discharge (overt or basal).
Endothelial dysfunction results in the development of ACS. Triphala increases
mitochondrial capacity, therefore, increases ATP synthesis corrects ATP
mismatch, strengthens endothelium which now behaves like healthy endothelium.
Strengthened endothelium, inhibits entry of platelets, inflammatory cells and
supports the release of endogenous tissue tPA to lyse thrombus. The overall
effect is significant relief in ACS. Study finds a positive role of endothelial
strengthening in ACS with Triphala.
Limitations of the
study- small sample size
Suggestions: Study with
large sample size and use of other plants or drugs [Ginseng a Chinese medicine
and Ashwagandha (Withania Somnifera)]
which have potential to support mitochondrial activity may be used for
endothelial strengthening to further consolidate the findings of the study [34,35].
References
1.
Mudau
M, Genis A, Lochner A and Strijdom H. Endothelial dysfunction: the early
predictor of atherosclerosis (2012) Cardiovascular J Africa 23: 222. https://doi.org/10.5830/cvja-2011-068
2.
Chhabra
N. Endothelial dysfunction- A predictor of atherosclerosis (2009) Internet J
Med Update 4: 33-41.
3.
Osto
E and Cosentino F. The role of oxidative stress in endothelial dysfunction and
vascular inflammation (2010) (2nd Edn) Ignarro LJ (Ed) Nitric Oxide:
Biology and Pathobiology, London: Academic Press, London pp. 705-754. https://doi.org/10.1016/b978-0-12-373866-0.00022-8
4.
Kinlay
S and Ganz P. Relationship between endothelial dysfunction and acute coronary
syndrome: implications for therapy (2000) Am J Cardiol 19: 10J-13J.
5.
Trepels
T, ZeiherAM and Fichtlscherer S. The endothelium and inflammation (2006)
Endothelium 13: 423-429. https://doi.org/10.1080/10623320601061862
6.
Choi
D, Hwang KC, Lee KY and Kim YH. Ischemic heart disease: current treatments and
future (2009) J Contr Release 140: 194-202.
7.
Tang
EH and Vanhoutte PM. Endothelial dysfunction: a strategic target in the
treatment of hypertension? (2010) Pflugers Arch 459: 995-1004. https://doi.org/10.1007/s00424-010-0786-4
8.
Jonathan
WY, Teoh H and Verma S. Endothelial cell control of thrombosis (2015) BMC
cardiovasc Disord 15: 130. https://doi.org/10.1186/s12872-015-0124-z
9.
VanHinsbergh
VW. Endothelium-role in regulation of coagulation and inflammation (2012) Semin
immunpathol 34: 93-106.
10.
Ezihe-Ejiofor
JA and Hutchinson N. Anticlotting mechanisms 1: physiology and pathology (2013)
Continuing Educatn Anaesthesia Cri Care Pain 13: 87-92. https://doi.org/10.1093/bjaceaccp/mks061
11.
Altun
I, Oz F, Arkaya SC, Altun I, Bilge AK, et al. Effect of statins on endothelial
function in patients with acute coronary syndrome: a prospective study using
adhesion molecules and flow-mediated dilatation (2014) J clinic med res 6: 354.
https://doi.org/10.14740/jocmr1863w
12.
PradyumnaRao
T, Okamoto T, Akita N, Hayashi T, Kato-Yasuda N, et al. Amla (Emblica
officinalis Gaertn.) extract inhibits lipopolysaccharide-induced procoagulant
and pro-inflammatory factors in cultured vascular endothelial cells (2013) Br J
Nutrition 110: 2201-2206. https://doi.org/10.1017/s0007114513001669
13.
Krishnaveni
M and Mirunalini S. Therapeutic potential of Phyllanthus emblica (Amla): the ayurvedic wonder (2010) J Basic
Clin Physiol Pharmacol 21: 93-105. https://doi.org/10.1515/jbcpp.2010.21.1.93
14.
SaiRam
M, Neetu D, Deepti P, Vandana M, Ilavazhagan G, et al. Cytoprotective activity
of amla (Emblica officinalis) against chromium (VI) induced oxidative injury in
murine macrophages (2003) Phytother Res17: 430-433. https://doi.org/10.1002/ptr.1157
15.
https://en.wikipedia.org/wiki/Acute_coronary_syndrome
16.
Saxena
T, Patidar S and Saxena M. Assessment of left ventricular ejection force and
sympathetic skin response in normotensive and hypertensive subjects: A double
blind observational comparative case- control study. https://doi.org/10.1016/j.ihj.2015.12.005
17.
Patel
JC. Functions of endothelium (2001) Indian J med sci 55: 165-166.
18.
Rajendran
P, Rengarajan T, Thangavel J, Nishigaki Y, Sakthisekaran D, et al. The vascular
endothelium and human diseases (2013) Int J bio sci 9: 1057. https://doi.org/10.7150/ijbs.7502
19.
Mulligan-Keh
JH and Simons M. Vasa vasorum in Normal and Diseased arteries (2014) Circulation
129: 2557-2566. https://doi.org/10.1161/circulationaha.113.007189
20.
Gordan
R, Gwathmey JK and Xie LH. Autonomic and endocrine control of cardiovascular
function (2015) World J cardiol 7: 204. https://doi.org/10.4330/wjc.v7.i4.204
21.
Saxena
T, Khichi G and Saxena M. Cell Death in Stroke: Role of Metabolism (2017) Austin
J Cerebrovasc Dis and stroke 4: 1059. https://doi.org/10.26420/austinjcerebrovascdisstroke.2017.1059
22.
Saxena
T, Patidar S, Saxena M and Bhabrawala A. Asthma treatment Role of metabolism (2018)
Exploratory Research and hypothesis in Medicine 3: 6-13.
23.
Hall
JE. Guyton and Hall Text book of medical physiology (2016) (13th
Edn) Mario Vaz, AnuraKurpad and Tony raj (Eds) Elsevier, USA.
24.
Saxena
T, Maheshwari S and Saxena M. Aetiopathogenesis of Type-2 Diabetes Mellitus:
Could Chronis Stress Play an Important Role? (2014) JAPI 62: 24-29.
25.
Kumar
V, Abbas A and Aster J. Robbins and Cotran- Pathologic Basis of Disease: South
Asia edition (2016) RELX India private limited, New Delhi pp. 497-501.
26.
Boron
W and Boulpaep E. Medical physiology: a cellular and molecular approach (2011)
(2nd Edn) PA: Elsevier Saunders, Philadelphia, USA.
27.
Yamamoto
H, Morino K, Mengistu L, Ishibashi T, Kiriyama K, et al. Amla enhances
mitochondrial spare respiratory capacity by increasing mitochondrial biogenesis
and antioxidant systems in a murine skeletal muscle cell line (2016) Oxidative
med cellular longevity. http://dx.doi.org/10.1155/2016/1735841
28.
Patel
SS and Goyal RK. Emblica officinalis Geart: a comprehensive review on
phytochemistry, pharmacology and ethnomedicinal uses (2012) Res J Med Plant 6:
6-16. https://doi.org/10.3923/rjmp.2012.6.16
29.
Usharani
P, Fatima N and Muralidhar N. Effects of Phyllanthus emblica extract on
endothelial dysfunction and biomarkers of oxidative stress in patients with
type 2 diabetes mellitus: a randomized, double-blind, controlled study (2013) Diabetes,
Metabolic Syndrome Obesity: Targets and Therapy 6: 275-284. https://doi.org/10.2147/dmso.s46341
30.
Anila
L and Vijyalaxmi NR. Flavanoids from Emblica officinalis and Magnifera
indica.Effectiveness for dyslipidemia (2002) J Ethnopharmacol 79: 81-87.
31.
Antony
B, Merina B, Sheeba V and Mukkadan J. Effect of standardized Amla extract on
atherosclerosis and dyslipidemia (2006) Indian J Pharm Sci 68: 437-441. https://doi.org/10.4103/0250-474x.27814
32.
Rijken
DC and Lijnen HR. New insights into the molecular mechanisms of the
fibrinolytic system (2009) J thrombosis haemostasis 7: 4-13.
33.
Huber
D, Cramer EM, Kaufmann JE, Meda P, Masse JM, et al. Tissue-Type Plasminogen
Activator (t-PA) is stored in Weibel-Palade bodies in human endothelial cells
both in vitro and in vivo (2002) Blood 99: 3637-3645. https://doi.org/10.1182/blood.v99.10.3637
34.
Vidyashankar
S, Thiyagrajan OS, Varma SR, Sharath Kumar LM, Babu VU, et al. Ashwagandha (Withania somnifera) supercritical CO2
extract derived Withanolides mitigates Bisphenol A induced mitochondrial
toxicity in HepG2 cells (2014) Toxicol Rep 1: 1004-1012. https://doi.org/10.1016/j.toxrep.2014.06.008
35. Li XT, Chen R,
Jin LM and Chen HY. Regulation on energy metabolism and protection on
mitochondria of Panax ginseng polysaccharide (2009) Am J Chin Med 37: 1139-1152.
*Corresponding author:
Tarun Saxena, Senior Consultant, Department of Internal Medicine,
Mittal Hospital and Research Centre, Ajmer, Rajasthan, India, Tel: +91-982 908
9284, E-mail: yogdiab@gmail.com
Citation:
Saxena T, Patidar S, Verma S, Ali OA and Saxena
M. Endothelial cells strengthening: Improving functions in management of acute
coronary syndrome (A double blind randomized interventional control trial)
(2019) Clinical Cardiol Cardiovascular Med 3: 17-22.