
 PDF
PDF
Advances in Knowledge
· Physiotherapists
are suggested to include assessment of hand function as a part of regular
musculoskeletal assessment for shoulder pain.
· We suggest to
physiotherapist that even if the shoulder is full and free if the hand is not
in the functional state the rehabilitation of the shoulder is not complete.
· Following this
study, people who treat shoulder conditions will give due attention to hand
function training as a part of shoulder pain rehabilitation which is seldom
practiced currently.
Application to Patient Care
Based upon the
study recommendations the patients with shoulder pain
· Will be trained
for hand function activities too.
· The patients will
be rehabilitated completely to become functionally fit to take part in skilled
activities as well
· The patients work
efficiency will be enhanced
· These patients
will utilize less energy for hand function activity that can contribute to the
endurance there by promote the work efficiency.
Introduction
Hand function
assessment has been included as mandatory in physical examination of many neurological
conditions, where the Hand Function is affected viciously, apart from other
functions of the upper limb. A classic example of such a condition is
hemiplegia following stroke [1]. The assessment of Hand Function helps in the
intervention designing and also in the prognosis of stroke rehabilitation. When
there is no direct impairment of the hand, like elbow and shoulder impairments,
the HF examination is ignored. This is true in the case of most of the
musculoskeletal conditions that affect the shoulder. But the fact is, proximal
stability is a prerequisite for distal mobility, be it a gross motor activity
or fine motor activity. This is true in both the upper limb and lower limb
where the proximal muscles significantly contribute to the distal muscle
activity. While attempting to grasp any object with hand, the resultant is
simultaneous muscle contraction at the elbow and shoulder [2,3].
It is proved in
the past that before the limb muscle contracted the trunk and proximal muscles
contracted in an anticipatory manner to give a proper background for distal
muscle activity [4]. This has strong physiological support as many neurons of
the motor cortex have outputs that innervate a spinal motor neuron pool of both
proximal muscles and intrinsic muscles of the hand. This claim was reinforced
when it was proved by the Spike-triggered averaging of EMG activity which
showed that neurons of the motor cortex have either facilitatory or inhibitory
effects on the motor neuron pools of shoulder, elbow, wrist and hand muscles
[5]. When the motor cortex is stimulated through a weak stimulus, a
monosynaptic Excitatory
Postsynaptic Potential (EPSPs) is produced in the motor neuron of the
distal and proximal muscles of both forelimb and the hind limb [6]. In most of
the shoulder conditions that present with pain and functional limitations,
there is always an associated impairment in muscles, skeleton, ligaments,
cartilage, and nervous system, which results in musculoskeletal dysfunction.
Despite a strong physiological and anatomical relationship between the proximal
and distal musculatures being established scientifically, there exists no
consideration for Hand Function assessment when assessing and treating painful
shoulder. This study was conducted to analyze the HF and HEC among subjects
with shoulder conditions resulting in pain and disability.
Methodology
This
cross-sectional study was conducted at the outpatient department of UCA College
of Physiotherapy, Chennai from August 2018 to August 2019. Ethical clearance
was obtained for the study from the institutional ethical committee, Saveetha
University on 12th April 2018. All the subjects who participated in the study
were clearly explained about the study before participation and were requested
to sign an informed consent. A total number of 82 subjects with shoulder pain
were screened for the study inclusion criteria and 47 subjects were selected
for the study.
Inclusion
criteria
· Both males and
females between 30 to 60 years were selected for the study.
· Subjects with a
history of shoulder dysfunction for a minimum period of one-month duration and
a maximum of 42 months. Shoulder dysfunction was defined for this study as “any
condition of the shoulder that has resulted in path-mechanical changes at
shoulder joint complex which has resulted in the altered functional activity of
the shoulder”.
· A variety of
shoulder conditions like bicipital tendonitis, supraspinatus tendonitis,
capsulitis at Glenohumeral
Joint (GHJ), degenerative conditions of the shoulder complex, were included in
the study.
Exclusion
criteria
· Subjects who had
a history of fracture, internal fixation anywhere in the affected upper limb or
cervical spine, subjects with bilateral shoulder complaints, any associated
problems of the affected upper limb or the cervical spine that might influence
the HF were excluded from the study.
· Subjects with
altered sensation, altered eyesight (using a spectacle), severe systemic
problem and general health depleted subjects were not considered for the study.
· All the subjects
were assessed for a shoulder disability, hand function, and hand-eye
coordination skills. SPADI
scale was used to evaluate the subject’s severity of pain and the associated
disability among the samples [7].
Apart
from this shoulder evaluation, the Purdue pegboard task was administered to find
the hand function/dexterity. Two blinded assessors were used in the analysis of
hand-eye coordination. One assessor was responsible for measuring the time
using a standard stopwatch, and the other was used to monitor the task for both
HF and HEC tests.
There
were three tasks performed by every subject three times with a gap of 60
seconds between each attempt. The first subtask required the subject to place
as many pegs as possible in 30 seconds in the target holes provided in the
pegboard. This task was performed with both hands consecutively. For the first
attempt hand was selected randomly. Task number two required the subjects to
place as many pegs as possible using both hands, by placing pegs simultaneously
[8]. The third task required the subject to place the peg, then the washer and
followed by the collar in a sequence prescribed by the guidelines. (Leslie,
Davidson and Batey, 1985) A battery of hand-eye coordination tests was
administered to the patient as follows.
Drill 1-Balloon
tossing task:
The subject had to bounce a balloon vertically up, back and forth with the
affected hand, as long as possible, followed by the normal hand. The task had
to be continued as long as possible and the subjects were not allowed to catch
the balloon. The task was repeated three times on each hand. The best score for
each hand was added and then used for statistical analysis.
Drill 2-Wall Ball
Bounce task:
The subjects stood 2M away from a wall and tossed a tennis ball onto the wall
in a self-passed manner. The subject had to catch the ball on return with a
single hand at first attempt without fumbling. The number of times the subject
successfully performed the task in 60 seconds was measured. The test was
performed with both hands. The task was performed only once and the score thus
obtained for each hand was added and was used for statistical analysis.
Results
A total number of 94 subjects were screened for the study out of which 58 subjects fulfilled the selection criteria. Out of the selected, 11 subjects opted out during the actual performance of the study tests, particularly the hand-eye coordination activity. The reasons for unwillingness to participate were apprehension to move, failure to succeed in task and few did not cite any reason but withdrew. 47 subjects participated in the study and completed all the tests. The demographic details of the subjects are provided in (Table 1).
Table 1: Demographic data of the participants.
The
scores of SPADI were correlated with the scores of Purdue pegboard scores and
the hand-eye coordination scores using a Spearman’s correlation as the data
were ordinal. SPSS version 24 was used for the data analysis. The SPADI scale
was correlated to the HF and Hand-eye coordination using its pain and
disability component separately, for the sake of in-depth analysis. We believed
that such analysis will give an idea about which component is strongly related
to the Hand Function and Hand-eye coordination.
The
mean and standard deviation values of SPADI pain component for the 47 subjects
was 25.3 (3.92), SPADI disability component was 28.8511 (5.15), HF scores on
PURDUE pegboard was 72.31 (4.64), hand-eye coordination in test 1 was 20.0426 (3.57)
and test 2 was 39.4043 (3.23).
The Spearman’s rank correlation test for the SPADI pain component revealed that there was a negative correlation with HF (R= -0.596, p< 0.001), but there was no correlation with HEC1 (R= -0.260, p= 0.078) and HEC2 (R= -0.217, p= -0.144). Though there was no correlation a negative relationship was observed between the variables. In the correlation of SPADI disability component there was a perfect negative correlation with HF (R= -0.870, p<0.001), with HEC1 (R= -0.588, p<0.001) and HEC2 (R= -0.541, p<0.001). In all the correlation a clear negative relation prevailed. The scatter plot representation of the data is shown in (Figure 1 and 2).
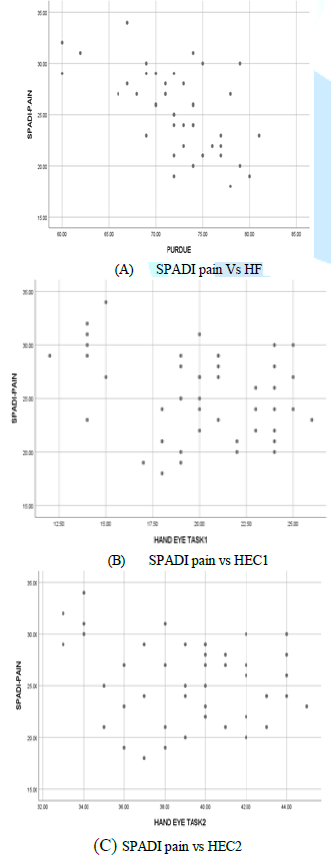
Figure 1: Correlation between SPADI pain component with HF and hand eye coordination.
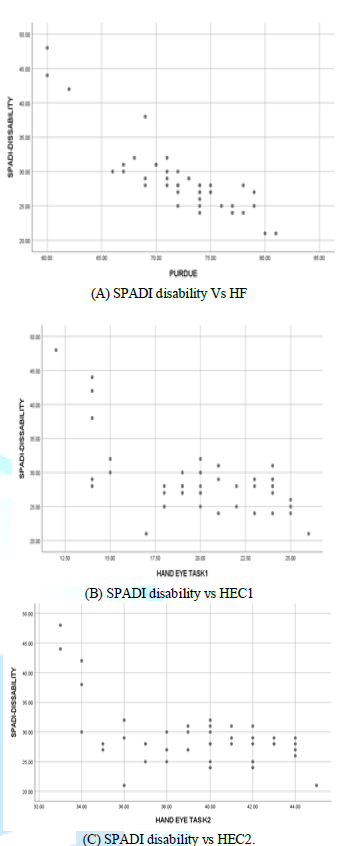
Figure 2: Correlation between SPADI disability
Discussion
In this study, an
effort was taken to find out the influence of shoulder
Pathology in HF and hand-eye coordination. Such a comparison was needed
because we perceived that proximal stability was a prerequisite for any distal
performance. For testing this hypothesis we adopted a cross-sectional study
where we correlated the pain and disability component associated with the
shoulder Pathology with HF and hand-eye coordination of the affected limb. For
this, we selected an age group that was vulnerable to shoulder pathology.
Almost 45% of the subjects fell into the age group of 30 to 40 years out of
which 90% of the subjects had rotator cuff injury and bicipital tendonitis. 34%
of the subject fell into 40 to 50 years category who were predominantly
suffered from supraspinatus tendonitis and adhesive capsulitis. Subjects with
50 to 60 years constituted just 21% who are predominantly affected by the
degenerative condition of glenohumeral joint, capsulitis and combined
presentation. In the study male and female ratio was 2 is to 1 respectively.
Male suffered more tendinopathy (63%) whereas females suffered more with
capsulitis and degenerative conditions (59%).
This can be
attributed to the work nature of the male and female. 42% of the dominant hand
pathology involved supraspinatus tendonitis and bicipital tendonitis, which was
in line with a systematic review which stated that the vulnerability of rotator
cuff tear is very higher on the dominant side [9]. 39% of the non-dominant hand
involvement was capsulitis and degenerative condition which was in line with
Katsuhiro Toda’s study which concluded that the right and dominant shoulders
were less frequently affected in subjects with frozen shoulder. Industry
analysis we found that a variety of pain was in subjects to had an acute
presentation of 1 to 6 months duration, whereas disability was more in case of
chronic presentation (more than 24 months). This trend is similar to the
reports in 2018, which stated that the disability rate hiked with duration of
ailment that resulted in more absenteeism among workers suffering from a wide
range of medical conditions [10,11].
The analysis of
the current study displayed an inverse relationship between the variables,
which signifies that when pain and disability of the shoulder were on a raise
the HF and HEC were compromised correspondingly. This is the first success of
the study, where the hypothesis
is not been explored before. As there was no prior documentation, comparing
shoulder conditions with HF and hand-eye coordination, our effort can be
considered unique and novel. There are previous studies that documented the
relationship between the shoulder and hand musculature. The shoulder muscles
were found to be active while the hand performed strong prehension activity. The
rotator cuff muscles, which are the stabilizers of the shoulder, were more influenced
than mobilizes during the hand activity recorded by EMG analysis [12,13].
Similarly, the
current study results showed shoulder pain was associated significantly with
the Hand Function, but there was no significant influence on Hand-Eye
Coordination whereas shoulder disability was significantly associated with
poor HF and HEC. This clearly states that shoulder disability rate influenced
the HF and HEC more than shoulder pain. As a matter of known fact disability in
such conditions develops in due course of time where the shoulder ranges of
motion deteriorated, limiting the freedom of movement. Some studies showed that
prolonged hand immobilization or injury can cause weakness in shoulder muscles and
the current study proved that this may happen vice versa too. The current study
did not use more objective measures like EMG, which may be a limitation but the
outcome measures used for the study are highly valid and reliable. Future
studies can concentrate on comparing other variables like handgrip strength the
effect of different body posture, shoulder position in the relationship of hand
and shoulder and influence of restricted shoulder ROM in hand performance
[14-16].
Conclusion
This study
concludes that shoulder pain negatively influences the Hand Function, whereas
the shoulder disability negatively influences both hand function and hand-Eye
Coordination. The major clinical inference from this study is that the
therapist should consider assessing and treating Hand Function and Hand-Eye
Coordination in patients with shoulder pain and disability.
References
1. Woldag H and
Hummelsheim H. Evidence-based physiotherapeutic concepts for improving arm and
hand function in stroke patients: A review (2002) J Neurol 249: 518-528.
https://doi.org/10.1007/s004150200058
2. Angst F,
Schwyzer HK, Aeschlimann A, Simmen BR and Goldhahn J. Measures of adult
shoulder function: Disabilities of the Arm, Shoulder, and Hand Questionnaire
(DASH) and Its Short Version (QuickDASH), Shoulder Pain and Disability Index
(SPADI), American Shoulder and Elbow Surgeons (ASES) Society Standardized
Shoulder (2011) Arthritis Care Res 63: 174-188.
https://doi.org/10.1002/acr.20630
3. Schieber MH
and Santello M. Hand function: peripheral and central constraints on
performance (2004) J Appl Physiol 96: 2293-2300. https://doi.org/10.1152/japplphysiol.01063.2003
4. Hodges P,
Cresswell A and Thorstensson A. Preparatory trunk motion precedes upper limb
movement (1999) Exp Brain Res 124: 69-79. https://doi.org/10.1007/s002210050601
5. McKiernan BJ,
Marcario JK, Karrer JH and Cheney PD. Corticomotoneuronal Postspike Effects in
Shoulder, Elbow, Wrist, Digit and Intrinsic Hand Muscles During a Reach and
Prehension Task (2017) J Neurophysiol 80:1961-1980.
https://doi.org/10.1152/jn.1998.80.4.1961
6. Clough BYJ,
Kernellt D and Phillip CG. The University Laboratory of Currents (3rd Ed)
(1968) 145-166.
7. Roach KE,
Budiman-Mak E, Songsiridej N and Lertratanakul Y. Development of a shoulder
pain and disability index (1991) Arthritis Care Res 4: 143-149.
https://doi.org/10.1002/art.1790040403
8. Mathiowetz V,
Wiemer DM and Federman SM. Grip and pinch strength: norms for 6- to
19-year-olds (1986) Am J Occup Ther 40: 705-711.
https://doi.org/10.1002/art.1790040403
9. Sayampanathan
AH, Hwee T and Andrew C. Orthopaedic Surgery a Systematic review on risk
factors of rotator cuff tears (2017) J Orth Surg 25: 1-9.
10. Toda K.
Orthopedic & Muscular System : Current Research Left and Non-Dominant
Shoulders Were More Frequently Affected in Patients with Frozen Shoulder : A
Systematic Review and Meta-Analysis (2018) Orthopedic & Muscular System 7:
1-3.
11. Zaidel CS,
Ethiraj RK, Berenji M and Gaspar FW. Health Care Expenditures and Length of
Disability Across Medical Conditions (2018) J Occup Environ Med 60: 631-636.
https://doi.org/10.1097/JOM.0000000000001308
12. Hospital O,
Palmerud G, Development L and Herberts P. “Influences of handgrip on shoulder
muscle activity (1995) Eur J Appl Physiol 71: 485-492.
https://doi.org/10.1007/BF00238549
13. Hakan S,
Gunnar P and Peter H. Hand grip increases shoulder muscle activity: An EMG
analysis with static handcontractions in 9 subjects (1996) Acta Orthopaedica
Scandinavica 67: 485-490. https://doi.org/10.1007/BF00238549
14. Budoff JE.
The Prevalence of Rotator Cuff Injured Hands (2004) J Hand Surg 29: 1154-1159.
https://doi.org/10.1016/j.jhsa.2004.06.006
15. Horsley I,
Herrington L, Hoyle R, Prescott E and Bellamy N. Do changes in hand grip
strength correlate with shoulder rotator cuff function? (2016) Shoulder Elbow
8: 124-129. https://doi.org/10.1177/1758573215626103
16. Antony NT and Keir PJ. Effects of posture, movement and hand load on shoulder muscle activity (2010) J Electromyogr Kinesiol 20: 191-198. https://doi.org/10.1016/j.jelekin.2009.04.010
*Corresponding author
Mohammad Sidiq, Research Coordinator, Rehabilitation Medicine Department, King Khalid Military City Hafar al Baten, P.O Box 10018, PC 31991 Kingdom of Saudi Arabia. Tel: +966596589667, Email:sidufatima@gmail.com
Citation
Kumar BS,
Subbaiah S, Ramachandran A, Sidiq Mohd, Yadav M, et al. Will musculoskeletal
conditions of shoulder affect the hand function and hand-eye coordination? a
cross-sectional analysis (2020) Rheumatic dis treatment J 1: 17-20.
Keywords
Shoulder Rehabilitation, Shoulder Physiotherapy, Hand
Function, Hand Eye coordination and SPADI.
